

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pancreatic cancer is one of the leading causes of cancer death worldwide. Despite recent advances in therapy, overall survival (OS) is less than 6 months, and 5-year survival rates for unresectable pancreatic cancer patients are very low.12 Although gemcitabine was originally regarded as the standard chemotherapy agent for advanced pancreatic cancer, any benefit was marginal, with an objective response rate of only 5% and a median survival rate of 5.7 months.3 Throughout the last 20 years, a number of clinical trials with various combinations of anti-cancer drugs have been performed. Combination chemotherapy with folinic acid, fluorouracil, irinotecan, and oxaliplatin (FOLFIRINOX) and gemcitabine/nab-paclitaxel have shown a remarkable improvement in survival benefits for advanced metastatic pancreatic cancer.45 However, the OS for both regimens is still less than 1 year, and they cannot be prescribed to all patients with unresectable pancreatic cancer, due to their relatively severe toxicity profiles.
Owing to increased information on the molecular changes in cancer, cell-specific anti-cancer targeted agents have been introduced into clinical practice. This shift in the treatment paradigm is focused on magnifying the anti-tumor effects while minimizing off-target adverse effects, which are the most common concern in patient management. There have been several clinical trials to assess the benefits of targeted agents including erlotinib, bevacizumab, and cetuximab for pancreatic cancer. To date, only erlotinib has been accepted as a standard drug when combined with gemcitabine.6 However, there are several issues with using gemcitabine-erlotinib combination chemotherapy for advanced pancreatic cancer, the most important being that there is no predictive factor for response to these drugs. In lung cancer, there are several well-known genetic predictive factors for response to tyrosine kinase inhibitors. 78 Thus far, most studies have concentrated on the relationship between genetic differences and response to erlotinib. However, it is also necessary to examine the clinical profiles of advanced pancreatic cancer patients, as they usually have coexisting diseases or conditions that require medications such as metformin or statins.9 In particular, statins have been evaluated for their potential anti-tumor effects. Recently, Nielsen, et al.10 reported that statin use in cancer patients is associated with reduced cancer-related mortality in 13 cancer types. Furthermore, several preclinical studies have suggested that statins have potential anti-cancer properties, including inhibition of cell proliferation, resulting in inhibition of tumor growth and angiogenesis.11121314 Other studies have demonstrated that the anticancer effect is due to statin-induced posttranscriptional modification of Ras and RhoA.151617
In this study, we attempted to determine the clinical factors that predict response to gemcitabine-erlotinib combination chemotherapy in advanced pancreatic cancer patients. We focused on the effect of concomitant statins on the oncologic outcomes of patients who received gemcitabine-erlotinib chemotherapy.
MATERIALS AND METHODS
Patients
This study included patients with unresectable or recurrent pancreatic cancer who received gemcitabine plus erlotinib as first-line chemotherapy at Severance Hospital (Seoul, Korea), between November 2006 and January 2014. All patients were histologically diagnosed with pancreatic adenocarcinoma and underwent dynamic computed tomography (CT) of the abdomen and pelvis. The tumors were classified as recurrent, locally advanced (including stage III), and advanced pancreatic cancer (including stage IV) using the American Joint Committee on Cancer (7th edition) guidelines. Patients were excluded if they had other malignancies, were unable to determine treatment response, had serum creatinine or total bilirubin levels >1.5×upper limit of normal (ULN), or had cardiomegaly on a chest radiograph.
Measurement of clinical factors
The clinical factors examined in this study were sex; age; history of diabetes mellitus, smoking, or chronic pancreatitis; type of operation; location or size of tumor; involvement of regional lymph nodes; number of metastatic organs; location of metastasis; locally advanced stage; involvement of major vessels; laboratory parameters including carbohydrate antigen (CA) 19-9, carcinoembryonic antigen (CEA), and bilirubin levels; and history of statin or aspirin treatment. Statins and aspirin could have been taken before or simultaneously with chemotherapy. Levels of CA 19-9, CEA, and bilirubin were evaluated before the first round of chemotherapy.
Treatment and assessment of therapeutic efficacy
Erlotinib was administered at a dose of 100 mg daily without interruption. Gemcitabine (1000 mg/m2) was administered by a 30-minute intravenous infusion on days 1, 8, and 15. The cycles were repeated every 28 days, provided that the absolute neutrophil count was >1500/µL, the platelet count was >100000/µL, bilirubin was <2×ULN, and serum creatinine was <1.5×ULN. Treatment was discontinued in cases of progressive disease, unacceptable adverse events, or withdrawal of patient consent. Tumor responses were assessed via CT every 8 weeks (two cycles) subject to the patient's condition or earlier in those with suspected progression based on the Response Evaluation Criteria in Solid Tumors.
Analysis of oncologic outcomes
The primary goal was to determine any clinical factors that influenced the response to gemcitabine-erlotinib chemotherapy. Therefore, we defined "long-term response" as occurring when gemcitabine-erlotinib chemotherapy was proven to show a tumor stabilization effect after six cycles of chemotherapy. The parameters for evaluating the tumor stabilization effect included complete response (CR), partial response (PR), and stable disease (SD) rates. In addition, we analyzed progression-free survival (PFS) and OS rates.
Statin exposure assessment
We reviewed the drug name, the cumulative duration of statin use, and the cumulative dose of statin intake. Statin users were defined as patients who received statin medications for at least 30 days. The statins prescribed during the study period were atorvastatin, rosuvastatin, simvastatin, and pitavastatin. The brand names of statins used in this study were as follows: simvastatin (Cholesnone, Simvastar, Vytorin); atorvastatin (Atorva, LipiLOU, Lipitor); rosuvastatin (Crestor, Vivacor); pitavastatin (Livalo).
The cumulative dose was standardized for different statins using the defined daily doses (DDDs) recommended by the World Health Organization.1018 The DDD for the 30 mg formulation of simvastatin was used as a reference, and the DDDs for the other statins were used to convert each statin dose to a dose equivalent to 30 mg of simvastatin.
Statistical analysis
The clinical factors associated with response rates were investigated by using multivariable regression modeling. The influence of potential prognostic factors on OS and PFS was assessed by using the Cox hazards regression model to estimate the hazard ratio (HR). Values of p<0.05 were considered to be statistically significant. Statistical analysis was performed using SPSS software, version 21.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Patient characteristics
This study included 180 patients with unresectable pancreatic cancer who received at least 2 cycles of gemcitabine-erlotinib combination therapy as first-line palliative chemotherapy between November 2006 and January 2014. The characteristics of the patients are shown in Table 1. The median age was 65 years. Twenty-four of 180 patients (13.3%) had locally advanced disease, and 156 (86.7%) had metastatic disease or recurrent disease after curative resection. The metastasis had spread to at least two organs in 61 patients (33.9%) and to one organ in 95 (52.8%). The liver was the most frequently metastatic site in 122 patients (67.8%), and carcinomatosis occurred in 39 (21.7%). Pretreatment CA 19-9 levels >1000 U/mL were detected in 87 patients (50.3%), and the median level was 1020 U/mL. Pretreatment CEA levels >4.5 ng/mL were measured in 84 patients (50.9%), and the median level was 4.67 ng/mL. The median number of gemcitabine-erlotinib combination chemotherapy cycles was four.
An objective response after two cycles of chemotherapy was observed in 40 patients (0 CR and 40 PR), resulting in a response rate of 22.2%. The disease control rate was 63.3% after two cycles of chemotherapy. A "long-term response," which was defined as having achieved CR, PR, or SD after six cycles of chemotherapy, was observed in 54 patients (30%). The median PFS and OS were 3.9 and 8.1 months, respectively. At the time of final data analysis, 162 of 180 patients (90%) had died.
Among all 180 patients, 17 received statin. Atorvastatin was most commonly prescribed (n=8, 47.1%), followed by rosuvastatin (n=6, 35.3%), simvastatin (n=2, 11.8%), and pitavastatin (n=1, 5.8%), as described in Supplementary Table 1 (only online). Among the patients that received statins during the study period, the median duration of use was 182 days.
Statistical analysis to determine response factors after two cycles of chemotherapy
Univariate analyses of the clinical characteristics indicated that six different factors were associated with response after two cycles of chemotherapy (Table 2). The following clinical factors showed statistical significance: pancreatic tail cancer [odds ratio (OR), 0.31; 95% confidence interval (CI), 0.12–0.78; p=0.013], locally advanced stage (OR, 3.71; 95% CI, 1.5–9.1; p=0.004), one metastatic organ (OR, 0.36; 95% CI, 0.14–0.91; p=0.03), two or more metastatic organs (OR, 0.15; 95% CI, 0.05–0.47; p=0.001), carcinomatosis (OR, 0.15; 95% CI, 0.05–0.47; p=0.01), and a history of statin treatment (OR, 4.79; 95% CI, 1.71–13.40; p=0.003).
In the multivariate logistic regression model, which included six statistically significant clinical factors from the univariate model, three factors showed independent statistical significance (Table 2). The presence of one metastatic organ (OR, 0.30; 95% CI, 0.11–0.81; p=0.017) and carcinomatosis (OR, 0.17; 95% CI, 0.02–1.00; p=0.05) were unfavorable factors for response. A history of statin treatment was a favorable factor for response after two cycles of chemotherapy (OR, 4.69; 95% CI, 1.41–15.6; p=0.012).
Statistical analysis to determine "long-term response" factors
We used univariate and multivariate analyses to determine factors associated with "long-term response." Four different factors had an effect on "long-term response" in univariate analysis (Table 2). These included locally advanced stage (OR, 2.71; 95% CI, 1.13–6.51; p=0.025), liver metastasis (OR, 0.46; 95% CI, 0.24–0.89; p=0.023), history of statin treatment (OR, 3.86; 95% CI, 1.38–10.78; p=0.01), and CEA level <4.5 ng/mL (OR, 2.15; 95% CI, 1.08–4.29; p=0.029). Multivariate analysis identified only one clinical feature that may affect "long-term response": a history of statin treatment, which was an independent favorable factor (OR, 4.11; 95% CI, 1.28–13.2; p=0.017).
Prognostic factors for survival
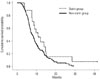
According to the Cox hazards regression model, liver metastasis was a prognostic factor that significantly affected OS (HR, 1.78; 95% CI, 1.05–3.01; p=0.031) and PFS (HR, 1.55; 95% CI, 1.09–2.19; p=0.013) (Table 3). A history of statin treatment, which was revealed to be the only favorable factor associated with "long-term response," was also significantly associated with OS after adjusting for all potential confounders (HR, 0.48; 95% CI, 0.26–0.92; p=0.026) (Fig. 1, Table 3).
DISCUSSION
Pancreatic cancer has a poor outcome, with a 5-year survival rate of only 5%.123 There have been significant medical advances, including targeted agents for unresectable advanced pancreatic cancer; however, the median survival time is approximately 6 months after the standard chemotherapy regimen of gemcitabine combined with erlotinib.6 Because of this very poor prognosis, a favorable response in the early chemotherapy cycles is important for longer survival times.
In this study, statins in combination with erlotinib and gemcitabine chemotherapy were associated with a good response in advanced pancreatic cancer for both short- and long-term chemotherapy. It is notable that concomitant use of statins showed a positive, long-term effect after >6 cycles of gemcitabine-erlotinib treatment. Considering that the median survival time of patients with advanced pancreatic cancer was approximately 6 months, the use of statins as chemoadjuvant treatment was meaningful in that it maintained tumor stabilization for the median survival time, assuming that the duration of one cycle of chemotherapy was equivalent to 1 month.
Many clinical studies have evaluated the potential anti-cancer effects of additional statin treatment. Colon cancer has been widely studied for associations between statin use and cancer incidence.192021222324 The protective effect of statins against the development of pancreatic cancer has also been presented.25 Khurana, et al.25 reported that statin administration for >6 months was associated with a reduced risk of pancreatic cancer by 67%. Statins are 3-hydroxy-3-methyl-glutaryl-coenzyme A (HMG-CoA) reductase inhibitors that reduce the synthesis of intracellular cholesterol by reversible inhibition of the conversion of HMG-CoA to mevalonate in the mevalonate pathway.26 This pathway also produces farnesyl pyrophosphate and geranylgeranyl pyrophosphate, both of which are involved in the posttranslational modification of cellular proteins including the Ras, Rab, Rac, and Rho families, which in turn influence cell proliferation, cell motility, and posttranslational modification. 2728 Statins block this pathway downstream, which may result in anti-cancer activity due to inhibition of tumor growth, angiogenesis, and metastasis.1214151629
Hong, et al.30 reported the first human clinical trial with statins used in combination with standard gemcitabine chemotherapy for advanced pancreatic cancer. This study showed that adding low-dose simvastatin to gemcitabine does not provide any clinical benefit when compared with gemcitabine plus a placebo.
However, we need to consider the potential synergic effect of statins and erlotinib referred to in many studies. By depleting mevalonate metabolites such as dolichol, farnesyl, and geranylgeranyl pyrophosphate through the inhibition of HMG-CoA reductase, statins have the potential to inhibit both epidermal growth factor receptor (EGFR) and its downstream signaling cascades.313233 Mantha, et al.34 reported that a combination of lovastatin and gefitinib, an anti-EGFR agent, showed significant synergistic anti-cancerous effects and enhanced EGFR inhibition.
Approximately 70–90% of pancreatic cancer patients are thought to have the v-Ki-ras2 Kirsten rat sarcoma viral oncogene homolog (KRAS).35 It is known that KRAS mutations are associated with a worse prognosis after anti-EGFR-targeted therapy in lung and colorectal cancer. It has been reported that statins may overcome resistance to anti-EGFR-targeted agents in colon cancer cells with the KRAS mutation.36 Our study also demonstrated that statins in combination with erlotinib were positively associated with a "long-term response." Therefore, statins may be a potential chemoadjuvant therapy along with anti-EGFR treatment for advanced pancreatic cancer patients with KRAS mutations.
In summary, this study suggests that statins have a favorable effect on the response to gemcitabine and erlotinib chemotherapy in advanced pancreatic cancer after six cycles of chemotherapy. As the median survival time of patients with advanced pancreatic cancer was approximately 6 months, statins may have a significant role as chemoadjuvant therapy for stabilizing long-term tumor growth. It is also important to note that statins have been used for a long time in cardiovascular disease with a proven safety record. Furthermore, prospective studies are needed to evaluate the efficacy of statins combined with chemotherapy containing anti-EGFR-targeted agents to overcome resistance to this treatment in advanced pancreatic cancer with KRAS mutations.



 XML Download
XML Download