

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Atrial fibrillation (AF) is the most common cardiac arrhythmia, occurring in 1-2% of the general population.1 The incidence of AF is known to increase with age, and an estimated 8 million people are affected in China.2 Additionally, this number is increasing rapidly due to the accelerated aging of the population. AF is associated with substantial complications, including increased risk of stroke, heart failure, and mortality,3 resulting in a serious health threat and a costly health burden.
Diabetes mellitus (DM) is an established risk factor for cardiovascular diseases such as hypertension, coronary heart disease, and heart failure.4,5 Moreover, DM has been regarded as a risk factor associated with stroke in current stroke risk scores.6,7 In recent years, studies have reported an increased risk of developing AF in patients with DM.8,9,10,11,12 Therefore, AF and DM often coexist and make treatment complicated. Individuals with AF and DM are at increased risk of thromboembolic complications, most notably stroke. It was reported that the incidence of stroke in patients with DM and AF ranges between 3.6% and 8.6% per year.13,14 Furthermore, the presence of DM may enhance the progression from paroxysmal AF to persistent AF15 and mask the cardiac symptoms of AF possibly due to DM neuropathy,16 resulting in delayed diagnosis and treatment.
Previous studies have investigated the impact of DM on the outcomes of patients with acute coronary syndrome,17 heart failure,18 and those undergoing coronary artery bypass surgery.19 However, the clinical characteristics, treatment, and prognostic impact of DM in patients with nonvalvular AF have not been well understood in China. The aim of the present study was therefore to investigate the issue from a prospectively designed multicenter registry study in China.
MATERIALS AND METHODS
Study population
From November 2008 to October 2011, a total of 2016 consecutive patients presenting to the emergency department (ED) with AF in 20 hospitals around China were recruited. The 20 hospitals were selected to represent different levels of medical care (academic and non-academic, general and specialized, urban and rural). This was a multicenter, prospective registry study with the aim of evaluating the risk factors and treatment of AF, as well as the 1-year outcomes including mortality, stroke, non-central nervous system (non-CNS) embolism, and major bleeding. Study protocols were approved by the appropriate Institutional Review Boards of Fuwai hospital and complied with the declaration of Helsinki. All subjects were provided with written informed consent.
Baseline characteristics
Patients were included in the registry if they had documented (electrocardiographic evidence by electrocardiogram, Holter, and rhythm strip) AF at the time of ED visits, regardless of the reason. Baseline characteristics including sex, age, weight, admission blood pressure, heart rate, and medical histories were collected at admission, and if necessary, related data was also collected from the patients' hospital charts and electronic medical records. The diagnoses of all medical conditions were based on clinical records. The type of AF included paroxysmal, persistent, or permanent AF. Paroxysmal AF was defined as AF episodes that terminate spontaneously. Persistent AF was defined as AF episodes that do not terminate spontaneously, yet do convert with either electrical or pharmacological cardioversion. Cases of AF that did not terminate either spontaneously or with electrical or chemical cardioversion or in which cardioversion had not been attempted were all classified as permanent AF.
Follow-up and endpoints
Follow-up was carried out 1 year±4 weeks after enrolment by telephone, outpatient service, or delivery of medical records. The primary endpoint was all-cause mortality during the 12-month follow-up. Secondary endpoints were cardiovascular mortality, stroke, major bleeding, and combined endpoint events (CEE, including all-cause mortality, stroke, non-CNS embolism, and major bleeding). Outcomes were adjudicated by a committee blinded to the therapy patients according to standardized definitions.
The definitions of every event were as follows. Death and the cause were determined as reported by the relatives of the participants during follow-up by telephone, and if possible, medical records were obtained. Stroke was defined as focal neurological deficits lasting at least 24 h and confirmed by computed tomographic scans or magnetic resonance imaging. The imaging data were collected during follow-up. Non-CNS embolism was defined as an acute loss of blood flow to a peripheral artery, supported by evidence of embolism from ultrasound tests, surgical specimens, angiography, or other objective testing. Major bleeding was defined as bleeding in a critical location such as intracranial bleeding, bleeding leading to surgical intervention, overt bleeding associated with a drop in hemoglobin concentration of ≥20 g/L or leading to transfusion of 2 or more units of blood, or fatal bleeding. These data were also collected during follow-up.
The patients were divided into a DM group and a non-DM group according to coexistent DM. DM was defined as a previous history of diabetes (treated with insulin or an oral hypoglycemic agent), or a non-fasting blood glucose level ≥11.1 mmol/L (200 mg/dL). The group of DM patients was compared with non-DM patients in terms of demographics, clinical characteristics, and 1-year outcomes.
Statistical analysis
The baseline characteristics of the patients are presented as mean±standard deviation for continuous variables and compared by Student's t-test if the data were normally distributed; otherwise the Wilcoxon signed rank test was used. Categorical variables are presented as percentage and were compared by Pearson's chi-square test. Survival curves and cumulative hazard function were constructed using the Kaplan-Meier method. Log-rank tests were used to compare the curves of the two groups. Univariate and multivariate Cox proportional hazard regression models were performed to identify whether there was an association between DM and the 1-year outcomes, and the models were corrected for age, sex, weight, medical history, vital signs at admission, and main medications. The adjusted hazard ratios (HRs), along with their respective 95% confidence intervals (CIs), were calculated for the two groups. All statistical tests were 2-tailed, and p values were statistically significant at <0.05. All statistical analyses were carried out using SPSS statistical software, version 19.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Of 2016 AF patients, 331 patients with valvular AF and 41 nonvalvular AF patients with incomplete data were excluded; consequently, 1644 patients were analyzed, of which 277 patients (16.8%) had concomitant DM.
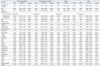
Table 1 summarizes the baseline characteristics in AF patients with and without DM. Compared with non-diabetic patients, patients with DM were more likely to be older (DM: 72.9±10.5 years; non-DM: 69.4±13.3 years; p<0.001) and heavier (DM: 66.6±11.4 kg; non-DM: 64.9±12.1 kg; p=0.029). As for cardiovascular histories, DM tended to coexist with coronary heart disease and hypertension, and the DM group also had a significantly higher percentage of stoke or transient ischemic attack, as well as myocardial infarction (MI) (all p<0.01). The admission systolic blood pressure in the DM group was higher than in the non-DM group (DM: 138.4±23.6 mm Hg; non-DM: 132.8±22.7 mm Hg; p<0.001), while diastolic blood pressure and heart rate was similar between the two groups (all p>0.05).
Table 2 shows the treatment during the 1-year follow-up. Those who were evaluated by CHADS2 scores and ≥2 (congestive heart failure=1, hypertension=1, age=1, diabetes=1, and stroke=2) were eligible for anticoagulation treatment. It was shown that a significantly higher percentage of patients with AF and DM needed anticoagulation treatment, compared with those without DM (DM: 93.5%; non-DM: 47.8%; p<0.001). However, anticoagulation with warfarin was adopted by only a small number of patients with DM (11.2%) and without DM (12.8%), and less than half of these patients reached the recommended international normalized ratio (INR) target. In contrast, more patients in the two groups (DM: 61.0%; non-DM: 55.7%) were prescribed with aspirin, and a small fraction of patients were prescribed clopidogrel instead of anticoagulation. In addition, patients in the DM group were more likely to be prescribed with beta-blocker, nondihydropyridine calcium channel blocker, angiotensin receptors blockers (ARB), and lipid-lowering agents (all p<0.05). Furthermore, for achieving and maintaining sinus rhythm, only a small portion of patients were treated with drug cardioversion (e.g., amiodarone), electrical cardioversion, or catheter ablation, and there was no significant difference between the two groups.
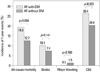
Fig. 1 shows the 1-year outcomes of the two groups. The overall 1-year all-cause mortality was 13.9% (228 of 1644 patients) in the present study. The all-cause mortality in the DM group was significantly higher than in the non-DM group (DM: 19.5%; non-DM: 12.7%; p=0.004). The overall incidence of stroke during the 1-year follow-up was 7.8% (129 of 1644 patients). However, the incidences of stroke between the two groups were comparable (DM: 10.1%; non-DM: 7.4%; p=0.141). The incidences of major bleeding were also comparable (DM: 0.3%; non-DM: 1.5%; p=0.166). The CEE rate in the DM group during the 1-year follow-up was significantly higher than that of the non-DM group (DM: 26.4%; non-DM: 20.4%; p=0.023).
The causes of death for the two groups are displayed in Table 3. It was observed that heart failure and infection were the major causes of death in both groups. The proportional mortality rate was similar between the two groups, except that the percentage of those who died of MI was higher in the DM group than in the non-DM group (DM: 9.3%; non-DM: 2.3%; p=0.036).
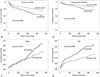
Fig. 2 shows the 1-year event curves of the two groups. It was observed that there were significant differences between the two groups in the survival curves of all-cause mortality (p=0.002), cardiovascular mortality (p=0.019), and cumulative CEE rates (p=0.004). However, the cumulative incidences of stroke between the two groups during the 1-year follow-up were comparable (p=0.127).
Table 4 displays the predictors of 1-year outcomes by univariate Cox analysis. It was found that DM was associated with increased risk of all-cause mortality (HR=1.596; 95% CI 1.176-2.116; p=0.003), cardiovascular mortality (HR=1.614; 95% CI 1.078-2.416; p=0.020), and CEE (HR=1.570; 95% CI 1.154-2.135; p=0.004), whereas it was not associated with an increased risk of stroke (HR=1.383; 95% CI 0.910-2.102; p=0.129).
Table 5 shows the results of a multivariate Cox analysis of 1-year outcomes. After adjusting the variables related with the outcomes of patients with AF, DM was still an independent risk factor for 1-year all-cause mortality (HR=1.558; 95% CI 1.126-2.156; p=0.007), cardiovascular mortality (HR=1.615; 95% CI 1.052-2.479; p=0.028), and CEE (HR=1.523; 95% CI 1.098-2.112; p=0.012); however, it was not an independent risk factor for stroke (HR=1.119; 95% CI 0.724-1.728; p=0.614).
DISCUSSION
The major findings from the present study are as follows. First, DM was prevalent among patients with nonvalvular AF, and more than 15% of nonvalvular AF patients suffered from concomitant DM. Clinically, most patients with nonvalvular AF and DM were at high risk for stroke; however, only a small amount of patients received anticoagulation treatment in China. Second, AF patients with DM had higher 1-year all-cause mortality, cardiovascular mortality, and CEE rates, yet had a similar incidence of stroke compared with those without DM. Third, after multivariate adjustment, DM was still an independent risk factor for 1-year all-cause death, cardiovascular death, and CEE, although it was not a risk factor for stroke.
The role of DM in cardiovascular risk and disease has been widely investigated. The adverse influence of DM on the cardiovascular system not only increases the risk of developing cardiovascular diseases but also exacerbates the outcome. Indeed, cardiovascular diseases are the most prevalent cause of morbidity and mortality in patients with DM.20 AF is the most common sustained cardiac arrhythmia in the population, and several epidemiologic studies have reported that DM is an independent risk factor for AF.2,4,5,9,10 Although the causal relationship between DM and AF remains to be elucidated,21 one likely explanation is that DM, directly or indirectly, affects cardiac electrophysiology supposedly by means of autonomic, electrical, and structural remodeling.22 Given the intimate relationship between AF and DM, further studies on the clinical characteristics of patients with AF and DM, as well as the impact of DM on clinical outcome in patients with AF, are of great importance for risk stratification and clinical management.
In our study, the prevalence of DM in patients with AF was 16.8%, similar to previous reports from western countries,23,24,25 though higher than data reported several years ago from China.26 With the development of social economy and an aging population, lifestyle changes related obesity, eating behavior, and physical activity may contribute to the increased prevalence of DM in general population, consistent with the findings in our study that patients with DM were more likely to be older and heavier. Meanwhile, patients with AF and DM had a higher prevalence of traditional cardiovascular risk factors such as hypertension, coronary heart disease, and stroke, which also demonstrated the association between DM and cardiovascular disease.
Anticoagulation is an important component in the management of AF, in that this arrhythmia is associated with an increased risk for stroke. In the present study, up to 93.5% of patients with AF and DM belonged to a high risk population stratified by CHADS2 risk scores.6 However, only 11.2% of these patients received warfarin for anticoagulation, and the number was even lower than those without DM (12.8%), in which the percentage of patients eligible for anticoagulation (47.8%) was lower than that of the patients with AF and DM (93.5%). Furthermore, less than half of the patients that received warfarin for anticoagulation reached the recommended INR target, indicating that the use and monitoring of warfarin remain to be improved. Although the overall proportion of patients that received anticoagulation with warfarin was low (12.5%) compared with that of the western countries,27 the number has been improved notably compared with several years ago in China (2.7%),2 reflecting progress in developing awareness for anticoagulation. However, more than half of the patients, regardless of whether they had DM or not, were prescribed aspirin or clopidogrel, which were confirmed to be ineffective in preventing thrombus.28 Moreover, about 20% of patients did not receive any prophylactic anticoagulation therapy, reflecting a huge gap between clinical guidelines and real-world practice in China. Fear of bleeding, the inconvenience of frequent INR monitoring, and excessive interaction between warfarin and other medications or foods may result in hesitating to select warfarin. It is expected that more AF patients will receive anticoagulation according to current guidelines by means of propaganda and education for both clinicians and patients. Moreover, it is anticipated that new oral anticoagulants characterized by safety, effectiveness, convenience, and also inexpensiveness will be widely available in China.
The prognostic impact of DM in patients with AF deserves critical attention. In our data, the overall 1-year mortality was 13.9%, similar to a previous report from the Framingham Heart Study.29 However, patients with AF and DM had higher all-cause mortality, cardiovascular mortality, and CEE rates during the 1-year follow-up in patients with DM than those without DM, demonstrating the serious macrovascular damage of DM. Indeed, cardiovascular disease is the major cause of morbidity and mortality for individuals with DM. Although the precise pathophysiological and clinical relationships between DM and cardiovascular disease are not completely understood, it has been suggested that an association between hyperglycemia and intracellular metabolic changes can result in oxidative stress, low-grade inflammation, and endothelial dysfunction, which may accelerate atherosclerosis and increase cardiovascular risk.20 Moreover, DM may mask the cardiac symptoms during an ischemic heart attack and also influence the cardiac symptoms related to AF,16 which may lead to delayed treatment and poor outcome in patients with DM.
In the present study, the 1-year incidence of stroke was 7.8% in whole patients and 10.1% in patients with DM, higher than previous reports.14 One possible explanation was the low level of anticoagulation treatment in patients with AF. Furthermore, as was found in our study, DM was not associated with an increased risk of stroke during the 1-year follow-up. Although certain previous studies30,31 also came to similar conclusions, pooled data from earlier stroke trials32 all identified DM as an independent risk factor for stroke. Indeed, the presence of DM predisposes patients to hypercoagulability characterized by platelet activation, increased production and activation of clotting factors, and hyperviscosity status.13 Currently, DM is included in commonly used, validated stroke risk scores that are incorporated in international guidelines.6,7 A possible interpretation for our results is that a relatively short follow-up period (median: 1 year) may not detect a significant difference in the incidences of stroke between DM and non-DM groups, whereas in other studies, such as the Framingham Heart Study,33 the mean follow-up period was 4 years, and most other studies had more than 2 years of follow-up.14 However, a trend toward increased incidence of stroke was observed in patients with DM at the end of the follow-up from the Kaplan-Meier curves, and a long period of follow-up is required to further detect the long-term impact of DM on risk of stroke.
In view of the high prevalence of DM in patients with AF, the high risk for embolism among patient characteristics, and the adverse prognostic influence, aggressive strategies are required for those with DM and AF. The risk of stroke varies among DM patients with AF, and treatment relies on risk stratification [CHADS2 or CHA2DS2-VASc (vascular disease, age 65-74, sex category) scores] and appropriate anticoagulation therapy. Currently, catheter ablation may be beneficial in the treatment of AF-associated DM.7 Additionally, upstream therapy such as ARBs34 and thiazolidinediones35 may also be beneficial for patients with DM and AF. Our study also suggests that use of ARBs was associated with a decreased risk of all-cause mortality and CEE. Moreover, use of lipid-lowering agents was associated with a decreased risk of stroke in our study. Therefore, more studies are required to further evaluate the impact of these agents on long-term outcomes.
There are some limitations in our study that should be noted. First, hemoglobin A1c percentages and fasting blood sugars were not recorded, limiting insight into glucose control, a factor that may have an effect on outcomes. Second, the duration of DM prior to study enrolment was also not known, which may reflect the severity of DM and associated co-morbid conditions; such a potential confounder may also affect the prognosis. Third, DM status in patients with AF was evaluated at enrollment only; we did not ascertain cases of DM that developed during the study follow-up. In addition, despite multivariate adjustments, residual confounding may remain. Finally, in our study, the period of follow-up was relatively short. Therefore, the long-term prognostic impact of DM in patients with nonvalvular AF needs to be evaluated by a long-term follow-up.
In conclusion, DM was found to be a common morbidity coexisting with nonvalvular AF and was associated with increased 1-year all-cause and cardiovascular mortality, as well as a higher CEE rate. A 1-year follow-up identified the association of DM with increased risk for all-cause mortality, cardiovascular mortality, and CEE; however, there was no increased risk for stroke.




 XML Download
XML Download