

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Retrieval of healthy oocytes is crucial to in vitro fertilization (IVF) treatment for infertile couples. Although mild ovarian stimulation has been introduced, most infertility centers still use conventional ovarian stimulation, which is defined as obtaining more than eight oocytes. Sometimes, however, only a few oocytes are obtained, leading to total fertilization failure or no transferrable embryos. This unsatisfactory circumstance, usually termed as poor ovarian response (POR), has a psychological impact and places an economic burden on infertile couples.
An enormous number of published studies have addressed the pathogenesis, prediction, and possible treatments of POR; however, a uniform definition of POR has not yet been agreed upon.1,2,3,4 A systemic review of 47 randomized trials showed that 41 different definitions were used for poor ovarian response.3 With the lack of a uniform definition, researchers are unable to effectively estimate and compare the incidences thereof. Accordingly, the European Society of Human Reproduction and Embryology (ESHRE) working group proposed the Bologna criteria for defining POR to ovarian stimulation for IVF in 2011.5
According to the Bologna criteria, at least two of the following three features must be present: 1) advanced maternal age (≥40 years) or any other risk factor for POR; 2) a previous POR (≤3 oocytes with a conventional ovarian stimulation protocol); or 3) an abnormal ovarian reserve test (ORT), antral follicle count (AFC) <5-7 or serum anti-Mullerian hormone (AMH) <0.5-1.1 ng/mL. Those with advanced maternal age or abnormal ORT are to be classified as "expected POR." Therefore, the most important component in the Bologna criteria is a previous POR.
In order to reach a common and universal definition, all components thereof should be selected based on scientific evidence. Although the Bologna criteria have emerged as a definition for POR,6,7 several criticisms have arisen against the criteria: first, patients included in their study were very diverse.8 Second, although maternal age and previous POR were well defined, detailed risk factors for POR were not described.5 Third, the cut-off levels of ORT were not suggested with clear cut-off points for each ORT included, especially in the case of AMH; the wide range of the cut-off levels does not offer uniform criteria. Lastly, the Bologna criteria were not based on scientific experiments and were just combined from criteria reported in previous studies. In fact, POR was defined as an oocyte number of less than four (irrespective of oocyte maturity) in the Bologna criteria since this number is most often used in the literature. However, defining the number of oocytes for POR should be made on scientific and epidemiologic bases. The term POR should be determined based on IVF outcomes [e.g., a significant decrease in clinical pregnancy rate (CPR) and live birth rate (LBR)].9
Two approaches can be utilized for defining an appropriate oocyte number for POR. These include statistical and prognosis-based approaches. One common approach to defining a certain variable as "abnormal" is to define it as less than the 5th or 10th percentile among a normal distribution. In such statistical approaches, cut-off values should be interpreted on the basis of disease prevalence, and for POR, its prevalence may vary according to a women's age. Meanwhile, as POR reflects a poor prognosis, the likelihood of it occurring can be determined by assessing treatment outcomes (i.e., clinical pregnancy, ongoing pregnancy, or live birth).
Here, we verified the appropriateness of the Bologna criteria and developed a more sophisticated definition by assessing oocyte number for defining POR based on statistical and prognosis-based approaches. We also evaluated the diagnostic performance of various factors in predicting POR according to our new definition. Finally, both the Bologna criteria and our new definition of POR were adapted to our data in which the incidence of POR, as well as diagnostic and clinical performance, was assessed.
MATERIALS AND METHODS
A retrospective study was performed including 176 consecutive IVF/intracytoplasmic sperm injection (ICSI) cycles (137 patients) with conventional ovarian stimulation during 2009 to 2012 at a university-based hospital. The eligible cohort comprised all consecutive patients who fulfilled the following criteria: 1) having at least 1 year of infertility, 2) being treated with a long agonist or antagonist protocol regimen (mostly GnRH antagonist protocol), and 3) having AMH values tested in our laboratory during the preliminary fertility workup at their first consultation. Cycles with mild stimulation protocol and cycles with total gonadotropin less than 500 IU were excluded. The study was approved by the Institutional Review Board of Seoul National University Bundang Hospital.
Several numerical [age, body mass index (BMI), number of present children, number of previous IVF cycles, cycle number, serum AMH, serum follicle stimulating hormone (FSH), total gonadotropin dose administered, number of total and mature oocytes, and number of embryos transferred] and categorical variables (infertility diagnosis, previous ovarian surgery, having one ovary) were recorded. Blood samples were taken from the cubital vein in the early follicular phase (day 2 or day 3), before any IVF-related drug administration. Serum AMH was measured by enzyme-linked immunosorbent assay (ELISA) using the Beckman Coulter AMH ELISA kit (Immunotech, Marseilles, France). The basic IVF and embryo transfer (ET) protocol was performed as described previously.10 Clinical pregnancy was defined as visualization of a gestational sac on ultrasound with evidence of biochemical pregnancies. Live birth was defined as the birth of at least one live-born child. The basic clinical characteristics of the patients and IVF cycles are shown in Table 1.
Medcalc version 12.6 (Medcalc Software, Mariakerke, Belgium) was used for statistical analysis and the results were considered statistically significant at p-values of <0.05. The chi-squared test was used to compare proportions between two groups. Univariable and multivariable regression analyses were performed for several variables [AMH, FSH, age, BMI (kg/m2), number of previous IVF cycles, number of living child, total FSH administered]. Receiver operating characteristics (ROC) curve analysis was performed to show whether the numerical variables can predict outcomes. Finally cut-off levels of AMH and number of retrieved oocytes for defining poor ovarian response were obtained using ROC curves.
RESULTS
Statistical approach
We performed exploratory data analysis for number of total or mature oocytes. The number of retrieved oocytes did not show a normal distribution (Fig. 1). The median numbers were 5 (range 0 to 34) for total oocytes and 3 (range 0 to 20) for mature oocytes. The skewness was 1.5 for total oocytes and 1.7 for mature oocytes. The 5th and 10th percentiles were 0.3 and 1 for total oocytes and 0 and 0 for mature oocytes, respectively. When POR was defined as total oocytes ≤2 (25th percentile), the incidence of POR was 25.6% (45/176), and the pregnancy rate (PR)/ET in the POR group was 22.2% (6/27), which was lower than PR/ET for the non-POR group (41.7%, 53/127, p=0.058); 40% of the POR cycles did not enter ET. When POR was defined as mature oocytes ≤1, the incidence of POR was 31.3% (55/176) and the PR/ET in the POR group was 16.7% (6/36), which was significantly lower than PR/ET for the non-POR group (44.9%, 53/118, p=0.002); the percentage of POR cycles not entering ET was 34.5%.
Prognosis-based approach
We analyzed cut-off values of oocyte number using ROC curves to predict IVF outcomes. Interestingly, all cut-off values for oocyte number were the same for clinical or ongoing pregnancy and live birth (i.e., total oocytes >5 and mature oocytes >1) (Table 2). Taken together, our findings from both statistical and prognosis-based approaches supported 'mature oocytes ≤1' as a definition of POR. The choice of 'total oocytes ≤5' as a definition of POR might be unrealistic as the incidence of POR would be too high (50.6%).
Considering both the statistical and prognosis-based approaches, we speculated that it would be reasonable to choose total oocytes ≤2 or mature oocytes ≤1 as the definition of POR. When POR was defined as 'total oocytes ≤2' or 'mature oocyte ≤1', the incidence of POR was 34.1% (60/176) and the PR/ET in the POR group was 19.5% (8/41), which was significantly lower than PR/ET in the non-POR group (45.1%, 51/113, p=0.004). The percentage of POR cycles not entering ET was 31.7%.
Predictive performance for our definition to POR
In univariable and multivariable regression analysis of the numerical and categorical variables listed in the methods, serum AMH, serum FSH, and age were shown to be related with total oocyte number and mature oocyte number (data not shown).
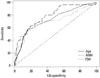
ROC curve analysis showed the cut-off values when POR was defined as total oocytes ≤2 or mature oocyte ≤1. For the purpose of screening method, the cut-off values of any predictor might be determined as those with low false positive rate, even though this reduces sensitivity. Therefore, we also presented the extreme cut-off values by setting a false positive rate of 5% (i.e., specificity 95%) (Table 3). The predictive performance of serum AMH was superior to both serum FSH, and age, although the differences therein were not statistically significant (Fig. 2). Combining the serum FSH or age did not enhance the predictive performance significantly (AUC 0.787 vs. AUC 0.823, p=0.246).
New definition of POR
Considering the best predictive performance of serum AMH with low false positive rate, we propose a new definition of POR: POR could be defined as total oocytes ≤2 or mature oocytes ≤1 obtained in a previous cycle or when serum AMH ≤0.76 ng/mL.
When these simple criteria were re-applied to our data, the incidence of predicted POR was 20.5% (36/176), with a sensitivity of 45.0%, specificity of 92.2%, positive predictive value of 75.0%, and negative predictive value of 76.4% (Table 4). Compared with the Bologna criteria, our new definition showed a similar predictive performance.
DISCUSSION
Poor ovarian response limits IVF success, and assessing various interventions is difficult because of wide variations in defining POR. In 2011, the ESHRE working group proposed the Bologna criteria to define POR to ovarian stimulation for IVF. However, as they stated, the aim of the Bologna criteria was to identify POR only for research purposes and that the criteria have no absolute value in predicting prognosis.4 The goal of ORT, especially in POR patients, is to add more prognostic information to the counseling and planning process in order to help couples choose among treatment options and to have a realistic expectations of fecundity. Thus, we attempted to develop a more objective and scientific definition of POR. In doing so, we discerned that POR could be defined as total oocytes ≤2 or mature oocytes ≤1 obtained in a previous cycle or for serum AMH ≤0.76 ng/mL (as an expected POR).
Sallam, et al.11 also attempted to define POR on the basis of IVF prognosis. In their study, CPR started to become significantly lower when fewer than five, six, and eight (maybe total) oocytes were retrieved from patients treated with ICSI, conventional IVF, or TESE/ICSI, respectively. Also, McAvey, et al.12 evaluated the association between the number of mature oocytes per IVF cycle and the likelihood of live birth. In conclusion there was an advantage to obtaining six or more mature oocytes during the fresh oocyte retrieval, compared with five or fewer oocytes. However, the choice of such a high oocyte number as the definition of POR might be impractical, as the incidence of POR would be too high.
In the Bologna criteria, AFC and AMH were used as ORT. However, AFC was not analyzed in the present study because objective reporting by the same observer was not available for all patients. Although the diagnostic performance of AFC in the prediction of poor ovarian response is good, recent literature indicates a new hormonal marker, AMH, as a preferred marker.13,14 The Practice Committee of the American Society for Reproductive Medicine concluded that there is mounting evidence to support the use of AMH as a screening test for POR and insufficient evidence to support the use of AFC as a screening test for failure to conceive.4 Among the numerical and categorical variables analyzed in the present study, only three variables (serum AMH, serum FSH, and age of women) could predict the POR with a statistical significance. Therefore, several risk factors proposed by the Bologna criteria were not included in our new definition. Indeed, 21 women in our series received ovarian surgery; however, ovarian response and IVF outcomes were similar between women with or without previous ovarian surgery.
ROC curves provide a graphic representation of a tradeoff between sensitivity and specificity. One of the commonly used criterion is Youden index that maximizes the sum of sensitivity and specificity. The cut-point leading to the index is the optimal cut-point when equal weight is given to sensitivity and specificity. It both measures the effectiveness of a diagnostic marker and enables the selection of an optimal threshold value (cutoff point) for the marker. The values for AMH, age, and FSH that resulted in maximizing the Youden index were defined as "usual cut-off values." However, in the context of defining POR, disease positive indicates individuals with poor response and disease negative indicates those with a normal or high response. A false positive refers to good responders, although it is wrongfully assigned to poor responders. From a practical viewpoint, false positive rates should be lower than 5%. This is, in general, a prerequisite for proper screening tests. Thus, in our study, "usual cut-off values" were derived from the Youden index, while the maximal deflection points and "extreme cut-off values" were chosen at the point at which the false positive rate was 5%.
In the present study, when POR was defined as total oocytes ≤2 or mature oocyte ≤1, the AUC of serum AMH was highest and combining serum FSH or age did not enhance the predictive performance thereof significantly. Currently, there is mounting evidence of serum AMH as a better predictor of POR, compared to serum FSH or age of a woman.15-24 This finding was subsequently confirmed in an individualized patient data meta-analysis, with no significant improvement in classification of a poor ovarian response, above a basal AMH when age, FSH, or AFC were also taken into account. Considering these findings, serum AMH appears to be an optimal variable for defining POR. Additionally, a previous meta-analysis concluded that basal FSH is not a useful predictor of IVF outcome,25 possibly because of inter-cycle variability.26 Meanwhile, serum AMH exhibits little inter-cycle variability in comparison to serum FSH; it is well-known as a quantitative indicator of oocyte number and as a qualitative indicator of oocyte quality and clinical pregnancy.21,27,28 Although several studies have recently shown that serum AMH is affected by a number of factors, including obesity, serum vitamin D, and serum leptin,29,30,31,32 AMH remains one of the most reliable markers of ovarian reserve. Therefore, we proposed that serum AMH alone is sufficient as a predictor of expected POR. Nevertheless, studies have suggested that AMH <0.1-2.0 ng/mL is a poor predictor of ovarian response and likely CPR in all women with normal ovarian reserve.15,16,17,18,19,20,21,22,23,24 Moreover, an AMH <0.2 ng/mL has been suggested as a poor predictor of CPR in women with POR.33,34 On the other hand, Gleicher, et al.35 showed that AMH ≥1.06 ng/mL is a predictor of good LBR in women with POR.
When we applied the Bologna criteria or our new definition to our data, the predictive performances were similar. The incidence of expected POR was higher when our new definition was applied (27 vs. 36), although the incidences of true POR were the same for both criteria. Applying either the Bologna criteria or our new definition applied, expected POR had a similar ongoing PR: 11.1%/cycle (3/27) and 17.6%/ET (3/17) vs. 13.9%/cycle (5/36), and 20.0%/ET (5/25).
Although limited by the relatively small sample size, we propose a new definition of POR, which is simple and based on statistical and prognosis-based evidence. We adopted serum AMH alone as a predictor for greater simplicity of the prediction model and adopted a lower false positive rate for serum AMH as a prerequisite of an appropriate screening method. Our new definition might be helpful when selecting patients in clinical practice, as well as for research purposes.





 XML Download
XML Download