

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Achondroplasia is the most common form of rhizomelic dwarfism, with an incidence of approximately 1 in 25000 people.1234 Bilateral lower-limb lengthening has been commonly performed for patients with achondroplasia, as it improves the quality of life (QOL) in selected patients.2 However, only a small number of reports have described bilateral lengthening of both the femur and tibia in these patients.567 Moreover, these and other previous studies analyzed the femur and tibia as a whole, and these bones were not compared with each other in terms of the proportion of each limb segment and the rates of callus formation, consolidation, and complications.2468910
Therefore, we proposed 1) to compare the radiological outcomes of femoral and tibial lengthening and 2) to investigate the differences of complications related with bilateral lower-limb lengthening in patients with achondroplasia.
MATERIALS AND METHODS
After receiving approval from the Institutional Review Board of our hospital, we retrospectively reviewed 142 patients with achondroplasia who underwent lengthening procedures between January 2004 and December 2012. All patients were diagnosed with achondroplasia as proven by genetic evaluation. The clinical features and radiographic findings were examined by pediatric orthopedic surgeons and musculoskeletal radiologists. Any patient with achondroplasia who had joint pain related to abnormal limb alignment and functional deficit (including gait impairment) and who was willing to undergo surgery for limb lengthening for psychological or cosmetic reasons was eligible for the surgery. Patients who had previous injuries or bony surgery involving the lower extremities, medical comorbidities (e.g., heart disease, restrictive or obstructive lung diseases, neurologic issues such as cervicomedullary compression) that could render the patient at high risk for surgery, or other systemic diseases were excluded. Ultimately, 28 patients (112 segments; 56 femora and 56 tibias) who underwent bilateral tibial lengthening with an Ilizarov ring fixator and bilateral femoral lengthening with a monolateral external fixator were included in this study. Our goals of surgery were to realign the mechanical axis and to lengthen of bone segment by more than 30% of its initial length. The average ages of the patients at tibial and femoral lengthening surgeries were 9.2 years (range, 5.5-20.3 years) and 10.8 years (range, 6.8-21.5 years), respectively. The study population consisted of 10 males and 18 females. All patients first underwent bilateral tibial lengthening, and 9-48 months (average, 17.8 months) after this procedure, bilateral femoral lengthening was performed. The minimum follow-up period was 1 year after the femoral lengthening surgery (average, 3.8 years; range, 1.3-6.8 years). All data were obtained from medical records and radiographs.
Operative technique
All surgeries were performed by the senior author (HRS). At the time of the initial visit, all patients showed short stature (<3% of the average age-matched height) with genu varum deformity, ankle varus related to a long fibula, and severe medial deviation of the mechanical axis. Lengthening and angular correction of the tibia was performed first, as there should be no difference between the anatomical axis and the mechanical axis of tibia. We used the Ilizarov ring fixator for tibial lengthening after peroneal nerve release. Three or four rings were used depending on whether unifocal or bifocal osteotomies were performed around the center of rotation of angulation (CORA) for gradual correction of the deformity (if indicated) and lengthening. Paired hinges were aligned with the apex of the deformity, and a single lengthening rod was placed opposite to these hinges. We used two wires each at the proximal and distal rings. The proximal and distal tibiofibular joints were each transfixed with a wire to prevent distal or proximal migration of the fibula, respectively. We inserted two additional half pins at the proximal and middle rings. Osteotomy was performed using the multiple drill hole method around the level of the CORA. A monolateral external fixator (Dynaextor, BK Meditech, Seoul, Korea) was used for femoral lengthening. Two to four Schanz screws were inserted in the proximal and distal ends of the femur perpendicular to the anatomic axis. A transverse osteotomy was performed at the mid-diaphyseal region in all cases after longitudinally incising the periosteum. All procedures were conducted under image intensifier guidance. Postoperatively, full weight bearing was allowed from 3 days after the surgery, and lengthening was started after 7 days at a rate of 1 mm/day (0.25 mm every 6 hours). For tibial bone segments with bifocal osteotomies, lengthening was performed on the proximal metaphyseal area. The rate was adjusted during follow-up according to the morphologic features of the callus as described by Li, et al.11 Rotational deformities were gradually corrected at the end of the lengthening period. We removed the fixator when we observed three continuous cortices on the radiographs, and we also based our decision on the serial pixel value ratios (PVRs) as previously described.12 Patients underwent supervised daily physiotherapy, including active and passive range of motion (ROM) of the knee and ankle, beginning 2 days after surgery. Patients were followed on a weekly basis for the first month, bi-weekly during the lengthening period, and then monthly during the consolidation period.
Radiographic evaluation
Standard radiographs of both lower limbs were taken at each follow-up visit and compared with the preoperative and immediate postoperative images. All radiographs were studied by three independent observers (KWP, RNG, CAR) using Star PACS PiView (Star 5.0.6.1 software, Infinitt Co. Ltd., Seoul, Korea). At the time of each visit, we measured the amount of lengthening and the PVR. The serial PVR was measured on the calluses of the regeneration areas using the free-line range of interest method (Fig. 1).1213 A PVR of 1 indicated corticalization of the regenerate in the lengthening area. The radiological features of distraction osteogenesis were classified with regard to shape and type on the basis of the Li, et al.11 classification. The shape was based on the width of the callus compared to the original osteotomy site. The type was based on the callus shape (cylindrical, fusiform, or concave), three patterns of osteogenesis (homogeneous, heterogeneous, and lucent), and three densities (low, intermediate, and normal). The density was judged relative to the adjacent soft tissues and cortex. At the final follow up, we recorded the amount of lengthening, percentage of initial length gained, lengthening index (LI), external fixator index (EFI), and healing index (HI). The LI was calculated by dividing the duration of lengthening in days by the total length of the regenerate in cm. EFI was calculated by dividing the entire duration of external fixator application in days by the total length of the regenerate in cm. The HI was calculated by dividing the duration of consolidation in days (from the time of lengthening cessation to the time of removal of the external fixator) by the total length of the regenerate in cm. We estimated the intraclass correlation coefficient (ICC) values and corresponding 95% confidence intervals (CIs) for the interobserver reliability of all radiographic parameters. The estimated ICC values for interobserver reliabilities of the PVR and the amount of lengthening were 0.85 (95% CI, 0.68-0.94) and 0.94 (95% CI, 0.89-0.98), respectively.
Clinical results and complications
All patients were examined for any signs of pin tract infection, ROM of adjoining joints, angulation or translation of the osteotomy site, and other complications that could occur during lengthening. The complications were recorded according to the classification of Paley (problems, obstacles, sequelae).7 Subsequent treatment and any secondary operations were also documented.
Statistical analysis
Differences in the LI, EFI, HI, and PVR were assessed using a linear mixed-effect model analysis. Statistical differences in callus features were analyzed using a repeated-measures analysis of variance. The data were recorded using Microsoft® Exce® 2010 version (Microsoft Corp, Redmond, WA, USA) and analyzed using SPSS® software (SPSS Inc., Chicago, IL, USA). A p-value <0.05 was considered significant.
RESULTS
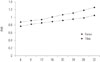
All procedures achieved the planned lengthening. The average gain in length was 9.8 cm (95% CI, 9.2-10.5) in the tibia and 8.4 cm (95% CI, 7.8-9.0) in the femur. The mean values of the LI, EFI, HI, and PVR of the tibia were significantly better than those of the femur (Table 1). The PVR at the regenerate of each bone increased during the distraction period, and a PVR of 1.0 at the regenerate was first achieved in the tibia. The mean PVR in the tibia was significantly higher than that in the femur during the entire distraction period (Fig. 2). In the 56 lengthened tibial segments, there were 54 homogeneous, two lucent, and no heterogenous pathways during the consolidation period, whereas in the 56 femoral segments, there were 37 homogenous, seven lucent, and 12 heterogenous pathways. In the tibia, there were 46 cylindrical, ten fusiform, and no concave shapes, whereas in the femur there were 36 cylindrical, 12 fusiform, five concave, one central, and two lateral shapes. Homogeneous and cylindrical shapes were more prominent in the tibia than in the femur (p<0.05).
A total of 61 complications were encountered in the 64 segments (23 during tibial lengthening and 38 during femoral lengthening) (Table 2 and 3). In tibial lengthening, there were 17 segments (30.4%) with joint complications and four segments (7.1%) with bony complications. Most problems in the tibial segments were due to the development of equinus deformities during lengthening (17 segments, 30.4%); however, these were all successfully managed by intramuscular gastrocnemius-soleus recession and the application of an Ilizarov foot frame for gradual correction. Relatively more complications occurred during femoral lengthening. Joint complications occurred in 18 segments (32.1%), and bony complications occurred in 18 segments (32.1%). A flexion contracture >30° with or without adductor tightness, which occurred in 16 (28.5%) patients, was the most frequent joint complication. Refracture was the most common bony complication during femoral lengthening (15 instances, 26.8%), followed by varus angular deformity (three instances, 5.4%). All of these complications were managed operatively (Fig. 3).
DISCUSSION
Limb lengthening surgeries have widely been used for patients with achondroplasia, which is known as the most common form of disproportionate dwarfism. However, limb lengthening is a complex procedure that has a high complication rate; hence, the limb must be lengthened safely without causing deterioration in function.14 In this study, we proposed 1) to compare the radiological outcomes of femoral and tibial lengthening in patients with achondroplasia and 2) to investigate the differences of complications related with lengthening.
Our study had several limitations. First, the number of patients studied was relatively small and only represented the patients who underwent the lengthening procedures. However, achondroplasia is uncommon, as previously mentioned;1234 hence, the number of patients was relatively large enough to investigate the effects of bilateral tibial and subsequent femoral lengthening. Second, the rate of distraction varied according to the morphology of the callus, and this may have had an effect on the PVR. However, we feel that this may not be significant, as it was validated in the senior author's previous study.1516 Third, the order of lengthening might have influenced the radiographic and clinical results. Most of our patients showed severe genu varum deformities and ankle varus deformities at the time of the initial visit. Therefore, we always corrected those deformities first, and lengthened the tibia simultaneously. Moreover, the anatomical axis of the tibia segment should be aligned along the mechanical axis of the lower extremity; therefore, correction and lengthening of the tibial segment first and then lengthening of femoral segment could be a practically reasonable option for this particular patient group. Fourth, the different types of external devices that were used in the two groups might have influenced the radiographic and clinical results. Ilizarov believed that the biomechanical environment provided by a fine-wire circular frame combined with a corticotomy produced the most favorable conditions for distraction osteogenesis,17 providing significantly better results for tibial lengthening. Moreover, the distance between bone and external fixators is shorter in the tibia, thus increasing stability and decreasing the risk of axial deviations.
The ability of the Ilizarov technique to lengthen both lower limbs in patients with achondroplasia and other causes of short stature has been confirmed in several studies;8910 however, our reason for using the monolateral fixator for the femur instead of the Ilizarov ring fixator was that the former provides greater comfort for patients without compromising stability.2 Lastly, we did not consider the preoperative and postoperative QOL assessment or correlate the findings with the complications that developed during lengthening. Hence, such an evaluation is recommended, as Kim, et al.18 mentioned that even with numerous complications, serial lower-limb lengthening is a good option for patients with achondroplasia, resulting in good QOL scores.
We found that the regenerate zone of the tibia had a significantly higher mean PVR than that of the femur, and all other parameters including the LI, EFI, and HI showed significantly higher values for tibial lengthening (Table 1), as callus formation in the tibia during distraction proceeds at a higher rate than that in the femur. Considering that the PVR method has been validated as an objective evaluation of mineralization in the lengthening zone,121519 we were able to determine the rate of callus formation by measuring the serial PVR until 32 weeks instead of a single estimate of bone-mineral apparent density (Fig. 2). The difference in the rate of callus formation is likely associated with the complications of femoral lengthening, such as refracture, callus subsidence, and angulation of the osteotomy site during weight-bearing.
In our series, there were more instances of cylindrical shapes and homogeneous pathways in the tibia than in the femur during lengthening. These findings might be related to the significantly lower mean LI, EFI, and HI during tibial lengthening than during femoral lengthening. In our study, both the tibial and femoral EFIs appeared to be comparable to the values reported in the literature for lengthening in healthy bone.72021 Previously, Singh, et al.13 reported that homogeneous pathways exhibited the most favorable outcomes during lengthening. Additionally, the callus pattern is known to be associated with a larger HI.22 We removed the external fixators only when a PVR of at least 1.0 was achieved, as we could safely rely on this variable to define the timing of fixator removal, given that it correlates well in patients with a cylindrical callus pattern regardless of whether the pathway is homogeneous or heterogeneous.162324
The risk of complications from lengthening increases with length.25 Moreover, the regenerate bone is 40-60% weaker than normal bone from 6 weeks to 6 months, and normal strength is not regained until 2 years later.26 In the lower limbs, the number of complications appears to increase when the extent of lengthening exceeds 20%.25 In our study, we were able to lengthen the tibia and femur by 9.8 cm (54.7%) and 8.4 cm (37.0%), respectively. Paley7 mentioned that lengthening is limited by the soft tissues; hence, lengthening to 5-8 cm carries medium risk, and exceeding 8 cm carries high risk. However, we were able to perform extensive lengthening, as bone healing is known to be good in achondroplastic and hypochondroplastic patients.27 These patients tolerate lengthening well due to ligament and soft-tissue laxity, and their muscle length exceeds their bone length before lengthening.28
We encountered many complications related to lengthening, and those difficulties were subclassified into categories defined by Paley7 as problems, obstacles, and complications. In this series, superficial pin-tract infection was the only problem identified in both tibial (two cases) and femoral (one case) lengthening. It required no operative intervention to resolve. Three obstacles in the series were encountered that required operative intervention to resolve. These included equinus deformity (n=17), genu valgum deformity (n=2), and premature fibular consolidation (n=1) in the tibia. Hip flexion contracture (n=16), knee flexion contracture (n=2), and deep surgical-site infection (n=1) were the obstacles encountered in femoral lengthening. A total of 21 (18.8%) true complications were recognized, 16 of which were refractures at the osteotomy sites (one tibial and 15 femoral refractures), and the three remaining complications were varus angular deformities in the femur. Fewer complications were found during the lengthening of the tibia than during the lengthening of the femur.
Muscle contractures are common in limb lengthening;7 particularly equinus deformity is known to develop at a high rate during tibial lengthening,29 and hip-and-knee flexion contracture is common in femoral lengthening.214 Although the exact etiology of equinus deformity remains unknown,29 it has been hypothesized that the shortened soleus-gastrocnemius-Achilles tendon complex is the cause of this deformity.30 Hip-and-knee joint contracture is common particularly during the lengthening of a congenitally short femur and has been associated with the tremendous forces exerted across the joints, which can result in hip or knee instability.5
In our study, there was one incidence of distal fibular migration due to premature fibular consolidation, which may be an indication of a high rate of bone formation during the lengthening process.31 Refracture, callus subsidence, and angulation of the osteotomy site during weight-bearing are known complications of femoral lengthening714 as manifested by bony complications in this series. Despite these problems, obstacles, and complications, the original goals of surgery were achieved in all treated segments, and our true complication rate was lower than the rates of previous studies, which ranged from 46% to 72%.73233
In addition, we believe that refractures and angulation deformities are more frequent in femoral lengthening than in tibial lengthening, as patella tendon bearing casts were applied after tibial fixator removal. Hence, tibial protection was added for 6 more weeks prior to full weight-bearing, whereas initially, weight-bearing with crutches was immediately started after femoral fixator removal. We suggest that the risk of refracture can be minimized by careful analysis of the regenerate during the consolidation period. It has been previously recommended to temporary cease distraction and apply gradual compression when concave, lateral, or central callus shapes appear in the regenerate bone until satisfactory regenerate with fusiform or cylindrical callus develops.14
In conclusion, tibial lengthening may be a more reliable procedure with a relatively lower complication rate compared with the findings for the femur. Callus formation in the tibia during the distraction period proceeds at a significantly higher rate than that in the femur. Our study suggests that bilateral limb lengthening of the tibia followed by femoral lengthening might be a reasonable option for patients with achondroplasia, provided that the patients are carefully monitored for complications and that these complications are promptly addressed whenever they occur.





 XML Download
XML Download