

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The process of metastasis involves the migration of tumor cells from the primary site to other parts of the body via the blood stream or lymphatic channels. Metastatic tumor cells are able to proliferate and grow in secondary sites by escaping from immune surveillance. Bone tissue is one of the three sites, most preferred for solid tumor metastasis,1 indicating that the bone microenvironment is compatible with secondary tumor growth. Furthermore, common types of cancer, such as breast, lung and prostate cancers, are more likely to result in bone metastasis than other types of cancer.1 It is estimated that when breast cancer metastasizes to bone, the relative five-year survival rate falls from 90% to less than 10%, indicating a greater need for further investigations into its mechanisms and treatments.2
Bone metastasis affects normal bone remodeling, leading to discrete osteolysis, diffuse osteopenia and osteoblastic lesion.1 Osteolytic tumors have a detrimental effect on the geometry of the bone and its biomechanical properties, since cancer cells enhance bone resorption.3 The factors released from bone subsequent to resorption (e.g., TGF-β1) provide positive feedback to the tumor cells, creating a cycle of decay.45
There are two main categories of drugs for the treatment of tumor osteolysis, namely anti-cancer and anti-resorptive drugs. Paclitaxel, a taxane, is the most commonly used anti-cancer drug to treat breast cancer.678 Paclitaxel, also known as taxol, acts mainly by stabilizing microtubule assembly through non-covalent interactions with tubulin, resulting in blockage of cell replication in the late G2 mitotic phase of the cell cycle, inhibiting proliferation.9 Bisphosphonates, on the other hand, are a class of anti-resorptive drugs that reduce bone resorption by inhibiting osteoclast activity. Traditionally, bisphosphonates were used in the treatment of osteoporosis, Paget's disease, and other bone metabolic diseases.101112 More recently, researchers have established the efficacy of bisphosphonates in the treatment of bone metastases.513141516 In particular, ibandronate, a third generation nitrogen-containing bisphosphonate, has been shown to have the capability to prevent tumor-induced osteolysis and hypercalcemia of malignancy101718 by inhibiting osteoclast activity. In spite of zoledronic acid being a prominent choice in recent studies as a more potent source of bisphosphonate, ibandronate was chosen for this study, because zoledronic acid is much more likely to cause renal tubule injury, leaving ibandronate an attractive viable option for patients.1920
Most animal models, which have been developed to study bone metastasis are that of immuno-compromised animals,21222324 which might not adequately represent events in bone metastasis, since the interactions between the immune system, tumor cells and the bone environment are not entirely preserved. Moreover, the treatment response of chemotherapeutic (paclitaxel) and anti-resorptive (ibandronate) drugs on bones affected by osteolytic tumors has not yet been thoroughly studied with the use of an immunocompetent animal model. Therefore, the objective of this study is to investigate the micro-architectural and mechanical effects of chemotherapeutic (paclitaxel) and anti-resorptive (ibandronate) treatments, together with an analysis of bone resorption markers [deoxypyridinoline (Dpd)] in a tumor metastatic immunocompetent animal model. It is hypothesized that anti-resorptive drugs (ibandronate) are as effective as high doses of chemotherapeutic (paclitaxel) drug in preserving bone micro-architectural and mechanical properties.
MATERIALS AND METHODS
Cell culture
Walker carcinoma 256 (W256) malignant rat breast cancer cells (ATCC, CCL-38 LLC-WRC 256 cells, Manassas, VA, USA) were cultured in M199 culture media (Sigma-Aldrich, St. Louis, MO, USA) with 5% horse serum (Sigma-Aldrich, St. Louis, MO, USA). The cells were maintained in a 5% carbon dioxide incubator at 37℃. On the day of surgery, cells were harvested and counted using a hemocytometer. Approximately 2.5×106 cells were suspended in 0.5 mL of saline in every surgery and used to develop the osteolytic tumor rat model.
Animals
Seventy female Sprague-Dawley (SD) rats, aged 10-12 weeks, were housed at the Laboratory Animal Centre in a light-controlled environment (12 h light-dark cycle) under standard temperature (23±1℃). They were fed with standard rodent chow and water ad libitum. The rats were randomly divided into four groups (SHAM, CANC, IBAN, and PAC). SHAM (n=16) was the control group while CANC (n=18) was used to observe the effect and progression of tumor growth. IBAN (n=18) and PAC (n=18) were administered with ibandronate and paclitaxel, respectively. All rats from the CANC, IBAN, and PAC groups had Walker Carcinoma 256 cells injected into their right femoral medullary canal via a drill hole made through the intercondylar notch to develop the osteolytic tumor.18 Rats from the SHAM group (n=16) also underwent similar surgical procedure, but saline was injected instead of cancer cells.
The IBAN group rats were given a subcutaneous administration of ibandronate (Bondronat®, Roche Diagnostics GmbH, Mannheim, Germany) at a dosage of 250 µg/kg of rat,18 once every ten days, starting from the day of the surgery. The increased inhibition of osteoclast resorption, coupled with ongoing bone formation, results in preservation of bone mass and architecture. However, exceeding a certain threshold of drug dosage (in this case 10 µg P/kg) results in decreased bone formation.25 This is why the mid value of the prescribed range (0.1<1<10 µg P/kg/day) was chosen. Paclitaxel (Anzatax®, Mayne Pharma Pte Ltd., Salisbury South, Australia) was administered intravenously at a dosage of 10 mg/kg of rat via the lateral tail vein of the PAC group rats, once every 10 days from the day of surgery.7 The CANC and SHAM group rats were given placebo treatment. Six (IBAN, PAC, and CANC) and four (SHAM) rats from each group were euthanized at intervals of 10 days and the femoral bones were harvested. The excised femurs were cleaned such that soft tissue was removed, wrapped in 0.9% saline-soaked gauze and stored in -20℃ freezer.
X-ray
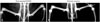
X-ray scanning of all rats was performed 10 days after the tumor inoculations by using Kodak DXS 4000 system at 35 kV for 2 minutes. X-ray analysis was performed with radiological scores given as follows: Grade 0 for no radiolucent lesion observed, Grade 1 for minimal but detectable lysis within the canal, Grade 2 for moderate lysis limited to the canal, and Grade 3 for extensive lesions extending into soft tissues.226 In this study, rats with detectable osteolysis were chosen for CANC and treatment (IBAN, PAC) groups. Only rats with osteolytic response (Grade 3 as in Fig. 1B) were utilized since sclerosis (tissue hardening) develops in slow growing or benign osteolytic lesions, in which it appears to limit lesion growth indicating regression of osteolysis.26
Micro-computed tomography
Prior to micro-computed tomography (µCT) scanning, the femurs were thawed to room temperature (25℃). The right distal femoral metaphysis was scanned using the SkyScan µCT machine (SkyScan 1172, Konitch, Belgium). The volume of interest (VOI), containing 152 CT slices, was located 6 mm away from the distal intercondylar notch and covered a region of 2 mm of the distal femur metaphysis as shown in Fig. 2A. Resolution of the scans was set at 13.148 µm. An average pixel size of 6 µm was used for scanning. These images were then analyzed, and four morphological indices, namely bone volume faction (BV/TV), trabecular number (Tb.N), trabecular separation (Tb.Sp) and trabecular thickness (Tb.Th), were obtained for micro-architectural analysis.3
Mechanical testing
The failure load (Fx) and stiffness (S) of femur specimens were obtained using the three-point bending test (Instron 5848 micro-testing machine, Norwood, MA, USA). Prior to testing, the femurs were thawed in 0.9% saline for about two hours until they reached room temperature (-25℃). Femurs were placed posterior side up on supports spanning 15 mm and a stabilizing preload of 10 N was applied at the center of the femur. The specimen was loaded till fracture at a deformation rate of 0.1 mm/s. The data acquisition interval was set to 5 ms. Testing conditions were determined through preliminary experiments.2728 The maximum force observed in the load-deformation plot was taken as Fx and the slope of the linear portion of the plot as the S.
Bone turnover marker
Approximately 1 mL of blood was collected from the central tail artery of each rat at 0, 10, 20, and 30 days. After standing for an hour, the blood was centrifuged at 4600 rpm for 20 minutes. The serum was then separated and stored at -20℃. The Metra® Total DPD EIA Kit (Mountain View, CA, USA) was used to determine the level of Dpd in serum to assess bone resorption activity.29
Statistical analysis
The SPSS 16.0 software (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Mean and standard deviation of all the variables were reported. One-way ANOVA was performed by time to determine significant differences between different groups at each time point. Similarly, one-way ANOVA test was also performed by respective groups to determine the significant differences of each group over the time period. Bonferroni corrections were used for all the comparisons and the results were considered to be statistically significant when p<0.05.
RESULTS
Morphological analysis
X-ray images of the SHAM and CANC groups are shown in Fig. 1. The cancer induced right femur (Fig. 1B) shows obvious osteolytic, radiolucent lesions (white arrows) unlike the sham operated right femur (Fig. 1A).
µCT images (1.5 mm by 1.5 mm) of distal rat femurs of all the four groups are shown in Fig. 2B. The CANC group exhibited reduced bone mass compared to the SHAM group. On the other hand, the IBAN and PAC groups displayed increased bone mass compared to the CANC group, indicating their efficacy in preventing bone loss.
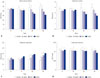
The changes in BV/TV, Tb.N, Tb.Sp, and Tb.Th of different groups with respect to time are indicated in Fig. 3, respectively. Analysis of the four groups indicated that there were no significant differences in Tb.Th across groups or time. As expected, the SHAM group revealed no significant variation in morphological indices across the entire duration of the experiment.
However, 20 days post-surgery, CANC group showed a significant decrease in the BV/TV and Tb.N, while the Tb.Sp showed a significant increase as compared to the SHAM group. By the 30th day post-surgery, BV/TV and Tb.N of the CANC group were lower than those of the SHAM group by 36% (p<0.001) and 38% (p=0.007), respectively. Furthermore, Tb.Sp of the CANC group was 92% higher than that of the SHAM group (p<0.001). These results confirm the successful induction of osteolytic tumors in the CANC group rats.
Starting from 20 days post-surgery, IBAN group rats showed significant variation in the morphological indices, i.e., the IBAN group was 40% (p=0.04) higher than CANC in BV/TV and 32% lower in Tb.Sp (p<0.001). However, Tb.N did not vary significantly between the two groups. Also, bone morphological indices of the IBAN group were not significantly different from those of the SHAM group.
The PAC group did not show significant differences in the BV/TV or Tb.N as compared to the CANC group at any point in the experiment. However, at the 30th day post-surgery, Tb.Sp of the PAC group was 22% lower than that of the CANC group (p=0.036). Unlike the IBAN group, the PAC group also showed significant differences in the BV/TV, Tb.N, and Tb.Sp, compared to the SHAM group.
Mechanical testing
Fx and S of different groups of rats with respect to time are shown in Fig. 4, respectively. The SHAM group showed no significant differences in the Fx and S of the bone over time. However, the CANC group showed significant decrease in both Fx and S. The decrease in Fx gained significance by the 30th day post-surgery (13.3%, p<0.03) and the decrease in S gained significance by the 20th day post-surgery (12.5%, p<0.001) as compared to SHAM.
The Fx values for both PAC and IBAN groups were similar and significantly higher than those of CANC group. Thirty days after surgery, the IBAN group had a 7.7% higher S value than CANC group (p=0.036) and 6.9% lower than SHAM group (p=0.041). There was no significant difference in the S values between the PAC and IBAN groups.
Bone turnover marker
The serum Dpd concentration for each rat was normalized against the reading on day zero, as shown in Table 1. The Dpd concentration of the CANC group increased by 31% after 10 days, 27% after 20 days, and 11.8% after 30 days, while Dpd concentrations in the SHAM group showed no significant variation.
The Dpd concentration of the IBAN group decreased by 37.9% after 10 days, 48.2% after 20 days, and 38.9% after 30 days, indicating that ibandronate treatment is effective in decreasing bone resorption. The PAC group did not show a clear trend in serum Dpd levels. This implies that there was no decrease in bone resorption activity for paclitaxel treated bones.
DISCUSSION
This study investigated the effects of tumor-induced osteolysis in an immunocompetent rodent model involving the inoculation of W256 carcinoma cells in SD rat femur. The efficacy of chemotherapeutic (paclitaxel) and anti-resorptive (ibandronate) treatment in overcoming the effects of metastasis was analyzed in terms of bone structural properties, biomechanical properties and biochemical marker analysis.
It has been reported that granulocytes can play an important role in immune response against initial stages of Walker 256 carcinoma development in SD rats, potentially affecting the characteristics of the tumor and are subsequently established in the host environment.30 The varied tumor responses observed in different host bodies subsequent to the inoculation of tumor cells could be a consequence of host body immune response. Four responses were noted; osteolytic, mixed (osteolytic with osteosclerotic signs), osteosclerotic healing flare and no response. Only rats with osteolytic responses were utilized for the cancer (CANC) and treatment (IBAN, PAC) groups in this study. It is an observation, although not unexpected, which was not widely reported in earlier studies of immunocompetent models31 including the study conducted by Kurth and Müller3 It could be due to a pre-selection of cell types prior to surgery i.e., induction of ascites in host bodies23 or soft agar growth of tumor cells before surgery.3 Nonetheless, successful adoption of an immunocompetent model imitates the actual environment in tumor osteolysis and helps clarify the effects of drugs on bone metastasis in a clinical setting.
Successful osteolytic tumor induction in this model had a harmful effect on bone architecture, as seen from the significant drop in BV/TV and Tb.N and rise in Tb.Sp in the CANC group in 20 days after surgery. This deterioration in bone architecture323334 was reflected in the biomechanical properties of bone, as evidenced from the decreased Fx and S of the bone on the 30th day post-surgery. The total serum Dpd concentration also showed an increase after tumor induction. Based on these results and µCT images, it is reasonable to conclude that tumor growth had been induced in the femoral bone in the osteolytic tumor rat models, causing accelerated bone resorption and micro-architectural deterioration, further leading to the loss of biomechanical competence in bone.
Previous studies showed that Tb.Th varied significantly after tumor induction.318 However, we did not observe statistically significant differences in Tb.Th between different groups or at different time periods. It is possible that Tb.Th is decreasing and the trend is masked by the disconnection of thinner trabeculae.
Morphological indices showed that ibandronate (anti-resorptive drug) had a better effect in treating tumor-induced architectural changes in bone than paclitaxel (chemotherapeutic drug). On the 30th day post-surgery, the BV/TV of IBAN was 40% higher than that of the CANC group, whereas a significant difference was not observed in the PAC group. This concurs with the study conducted by Strube, et al.,35 where MDA-MB-231 (SA) breast cancer to bone metastasis mouse model treated with paclitaxel (9 mg/kg i.p. once daily, 13-17 days) failed to show any significant change in BV/TV, compared to the vehicle-treated group. Similarly, Tb.Sp of the IBAN group was found to be 32% lower than that of the CANC group as compared to 22% of the PAC group. This trend indicates that ibandronate is more effective than paclitaxel in maintaining the structural properties of bone and preventing tumor-induced bone architectural changes. These experimental observations can be related to the mechanism of action of individual drugs, i.e., ibandronate directly inhibits osteoclast resorption and promotes osteoclast apoptosis at a later time1636 while paclitaxel stabilizes microtubule formation, arresting tumor cell division at the mitotic boundary,37 thereby indirectly affecting the degree of bone destruction induced by tumor cells.
Also, Dpd concentrations were significantly lower in the IBAN group, indicating successful inhibition of bone resorption and destruction. However, paclitaxel appeared to have no effect on Dpd concentration, and consequently, minimal effect on osteoclast resorption. Earlier in vitro studies have shown dose-related inhibition effects of paclitaxel on osteoclastic resorption.3538 However, paclitaxel is now shown to have negligible in-vivo effect on bone resorption even at 10 mg/kg, which is the maximum dosage that could be safely administered to rodent models.7373940
Apart from inhibiting osteoclast resorption, ibandronate treatment may allow more time for secondary mineralization,41 which aids in increasing bone mineral density,1042 thus preserving bone S. There are also reports of in vitro and in vivo evidence of bisphosphonates having anti-tumor effects254142434445464748 which might aid further preservation of bone strength and integrity. Therefore, the finding that ibandronate (250 µg/kg) has similar efficacy in maintaining bone mechanical properties to high doses of paclitaxel (10 mg/kg) is surprising since efficacy of ibandronate in bone preservation is well-established. Paclitaxel, on the other hand, is shown to have negligible effect on in vivo bone resorption, nevertheless, it preserves bone mechanical properties, comparable to ibandronate.
Before postulating that paclitaxel may have a direct effect on bone through other mechanisms that do not involve inhibition of bone resorption, bone biopsy and subsequent histomorphometric analysis are required to derive explicit conclusions on the effect of paclitaxel on bone remodeling.3538 Histomorphometric analysis will also be useful in determining the extent to which ibandronate affects tumor proliferation and growth in the intramedullary space. Halvorson, et al.36 reported that ibandronate induced extensive tumor cell necrosis in C3H/HeJ mice bearing osteolytic 2472 sarcoma cells. Earlier in vitro studies have also suggested that bisphosphonates have an influence on neovascularization.36 The specific mechanisms by which bisphosphonates can influence the growth of tumor metastasis and its viability are currently unclear and developing an understanding is an important objective of future research in the field of drug therapeutics.
In summary, an immunocompetent model was adopted where Walker 256 carcinoma cells provoked a localized increase in bone resorption, resulting in bone loss. Ibandronate was found to be as effective as high doses of paclitaxel in maintaining S of bone. Paclitaxel treatment did not appear to inhibit osteoclast resorption, which is contrary to earlier in vitro literature. The immune system also plays a plausible role in the selection of tumor cells as seen from the varied responses of the heterogeneous W256 carcinoma cells in the different host bodies. Emphasis should be placed on the use of immunocompetent models for examining drug efficacy for bone metastasis since it adequately reflects bone metastasis in clinical scenarios.



 XML Download
XML Download