

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Esophageal cancer (EC) is a highly lethal and aggressive tumor worldwide. Around the world, there were 482300 new cases of EC and 406800 deaths in 2008.12 According to 2013 Annual Report of Cancer Registration in China, it is the fourth leading cause of cancer-related death among male, and sixth among female. EC can be divided into two types according to histology: esophageal adenocarcinoma (EADC) and esophageal squamous cell carcinoma (ESCC). In China, ESCC accounts for most esophageal malignant tumors (about 87%). Although screening and multimodality therapy technology has greatly improved,34 the outcome for EC remains very poor; the 5-year overall survival rate is below 15%,56 emphasizing the need for early detection and prognostic markers. Over the past decade, scientific research have worked on revealing the molecular and biological mechanism that lead to carcinoma, leading to extensive search for prognostic markers in EC. For example, the expression of epidermal growth factor receptor (EGFR), Her-2, heat shock proteins (HSPs), and P53 has been found to be associated with the prognosis of EC.78910
The HSPs family is molecular chaperone and biochemical regulator, which functions to mediate cell growth, apoptosis, protein homeostasis, and cellular targets of peptides.11 It is a highly conserved cellular proteins group which is upregulated under stress conditions, including thermal, oxyradical, and inflammatory stress.1112 They are classified into six major family members based on their molecular size: HSP100, HSP90, HSP70, HSP60, HSP40, and small HSPs.131415 Excessive expression of HSPs in a wide range of human tumors have been reported, including breast, endometrial, ovarian, colon, lung, and prostate.16 Expression levels of HSPs are also reportedly altered, either increasing or decreasing, during malignant transformation.17 Studies have also shown that HSPs expressions are closely related with prognosis of carcinoma.1618
A question arises whether these findings justify the use of HSPs detection, in a routine clinical setting, as a prognostic indicator in patients with EC. In our study, we conducted a systematic review on HSP27, HSP70, and HSP90, which are three main members of HSPs family, and meta-analysis to estimate the prognostic importance of HSPs expression for survival among patients with EC.
MATERIALS AND METHODS
Search strategy
Two authors (Wang and Shi) conducted a systematic literature search independently in PubMed, Web of Science and Medline. Searches were applied from the day of establishment of the database to May 31, 2014. The following MeSH headings, keywords, and text words were used: 1) esophageal cancer OR esophageal neoplasms OR oesophageal neoplasms OR oesophageal cancer; 2) heat shock protein OR HSPs. We also used the references cited in the identified studies to complete the search.
Inclusion and exclusion criteria
Studies enrolled in this meta-analysis should meet the following criteria: 1) diagnosis of EC in humans was proven; 2) the expression of HSPs in the primary EC tissue was measured by any methods available; 3) data reported were related to the prognostic value; 4) survival rate, survival curve or sufficient data were provided for estimating an hazard ratio (HR) with 95% confidence interval (CI); 5) the follow-up time should be more than 5 years; 6) the study was published in English. The major exclusion criteria were: 1) study without extractable data, 2) case reports, editorials, commentaries, reviews or abstracts only, and 3) for duplicate publications and the smaller dataset.
Data extraction
Two investigators (Wang and Shi) reviewed all eligible studies and extracted data independently and resolved controversies by discussion. The name of the first author, year of publication, origin of country, histology, disease stage, number of eligible patients, gender, median age, test method, cutoff value, HSPs negativity, and survival results from each study were recorded (Table 1). Differences in the extraction of data were checked together by the two authors. If data from any of the above categories were not reported in the primary article, items were treated as "not reported." We did not contact the author to request the information.
Statistical analysis
For appropriate HSPs evaluation in a single study, the summary HR and their 95% CIs were combined to present the value reported in the study using methods described by Parmar, et al.19 We used HR calculations spreadsheet provided by Tierney, et al.20 were to calculate the estimation of HR from published summary statistics or data extracted from Kaplan-Meier curves.
Cochran's test (I2 statistics) was used to assess the heterogeneity of included studies. When heterogeneity was detected, a random effect model was applied; otherwise, a fixed effect model was used.21
The combined HRs were estimated using forest plots graphically. An observed HR of more than 1 implied a worse survival for the HSPs-negative, low HSPs expression group relative to the HSPs-positive, or high expression group, and if the 95% CI line of a study across the invalid line, it means that the study was not statistically significant. The study was considered statistically significant if the 95% CI did not overlap 1 (p≤0.05). Horizontal lines represent 95% CIs. Boxes represent the HR point estimate, and its area is proportional to the weight of the study. The diamond represents overall summary estimate, with the CI represented by its width. The unbroken vertical line was set at the null value (HR, 1.0). Assessment of publication bias was conducted using Funnel plot asymmetry.22 All the statistical analyses were conducted using Review Manager 5.2 (The Nordic Cochrane Centre, The Cochrane Collaboration, 2012).
RESULTS
Characteristics of the studies
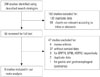
As the search flow diagram shows (Fig. 1), we identified the abstracts and titles of 248 primary studies for initial review using the search strategies as described. After exclusion of articles that were duplicate or not clearly relevant to our meta-analysis, we identified 56 candidate studies for full-text review. Upon further review, 4 review articles and 37 articles were eliminated because of having no survival data for meta-analysis. In the remaining 15 articles, 3 were not focused on the HSP members which we cared, 2 duplicate data and 1 was about gastric esophageal. Finally, 9 articles were selected.
These studies included three HSP members; 510232425 studies for HSP27, 617242526 for HSP70, and 3272829 for HSP90. The histopathology in most of the included studies was ESCC, while 1 study showed EADC and 2 studies showed EC (both ESCC and EADC). The studies were conducted in different countries; 5 of 9 studies were conducted in Japan, 2 in Germany, 1 in China, and 1 study in Sweden. The total number of patients was 801 and ranged from 62 to 125 patients per study (median, 89). The characteristics of the eligible studies are summarized in Table 1.
Meta-analysis results
The results of the meta-analysis are represented in Table 2 and 3, Figs. 2, 3, and 4. For studies evaluating HSP27 levels in EC (Fig. 2), the combined HRs were 2.93 (95% CI, 1.12-7.62). The results were significantly heterogeneous across these studies (p=0.01), and therefore, a random effect model was used in meta-analysis. For studies in ESCCs subgroup, the combined HRs were 3.90 (95% CI, 2.35-6.49) using a random-effect model. The results demonstrate that the reduced HSP27 expression was a significant prognostic factor in ESCC patients. For studies evaluating HSP70 levels in EC (Fig. 3), the test of heterogeneity was not significant, and a fixed-effect model was used in metaanalysis. The pooled HRs estimate for survival in these studies evaluating HSP70 levels in EC were 2.83 (95% CI, 1.90-4.23). However, when we limited the analysis to the 3 studies with ESCC, the combined HR was 3.21 (95% CI, 1.94-5.30), indicating that HSP70-positive patients had a more favorable prognosis than HSP70-negative patients. The combined HRs of HSP90 showed that the expression of HSP90 could not act as an effective prognostic marker in EC (HR: 0.99, 95% CI: 0.69-1.41, Z=0.07, p=0.95).
DISCUSSION
HSPs are highly conserved molecular chaperones, which are also referred to as stress proteins. It has been suggested that 'oncogenic stress' such as acidosis, hypoxia or hypothermia induces up-regulated expression of HSPs that assist in the recovery from stress by either repairing damaged proteins or by degrading them, which evokes a DNA damage response network that delays or prevents cancer at the beginning of tumorigenesis, thereby restoring protein homoeostasis and promoting cell survival.3031 Furthermore, molecular chaperones have been shown to influence tumour growth, differentiation and resistance to radio- and chemotherapy treatment, and they may have a significant impact on the survival of patients with cancer.3233
Many studies have shown that HSPs were related to cell proliferation and apoptosis. In the process of tumor formation, some tumors with expression of HSP27 and/or HSP70 appeared loss of differentiation ability, metastasis, and poor prognosis. In esophageal carcinoma patients, however, down-regulated expression of HSPs was associated with poor prognosis. In order to find an explanation for the observation, we summarized as follows: 1) it may be secondary to fundamental histologic differences between squamous cell carcinoma and adenocarcinoma, such as rectal or gastric cancer; 2) HSPs may be expressed continually because normal esophageal squamous epithelia are frequently exposed to agents such as heat or chemicals, so that HSPs can play roles in protecting cells; 3) HSPs expression is known to be correlated negatively with lymph node metastasis and depth of invasion. This may indicate that reduction of HSPs expression causes the tumor cells to proliferate; 4) There was a significant correlation between HSPs expression and lymphocyte infiltration, and this may indicate that HSPs expression promotes host immunity.1723242526 Thus, the patients with HSPs positive tumors tend to have a better prognosis than those with HSPs negative tumors.
This meta-analysis has some limitations. First, there may be some reports with negative or controversial results that have not been published, which leading to unavoidable publication bias. Second, this meta-analysis was limited to English articles, which leading to potential language bias. Third, studies enrolled in our meta-analysis used IHC to detect HSP level, which represent potential selection bias. Cutoff values for HSP expression differed in the percentage cell staining. Fourth, the estimated data that we obtained were not adjusted for other variables such as age, gender, histologic grade, and tumor stage. This may cause variability in assessing these variables between studies. Finally, there still might be a little error when the approximate calculation method was used to estimate the HR values, although 2 investigators calculated them separately.
In conclusion, our results suggest that reduced HSP27 and HSP70 expressions may be associated with a poor prognosis in patients with EC, thus warranting further definitive investigations into the potential clinical usefulness of HSP expression in ECs. It also appears worthwhile to prospectively validate if HSP27 and HSP70 expression used as prognostic markers could improve the outcomes of patients with EC, especially those with ESCC when integrated into clinical decision making.







 XML Download
XML Download