

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Colorectal cancer currently ranks the second most common cancer in males and the third most common in females in Korea. Among colorectal cancers, nearly 40-50% are rectal cancers.1 The goals of surgical treatment for rectal cancer are complete removal of the rectal cancer and preservation of sexual and voiding functions. Preoperative chemoradiation therapy (CRT) has been gaining popularly. According to NCCN guidelines, long-course 5-fluorouracil-based concurrent CRT is recommended in rectal patients with cT3,4 N0/+ disease. However, this recommendation does not include tumors with a threatening circumferential resection margin.
The standard long-course CRT is more common in North America and Korea; short-course radiotherapy is more common in European countries. Preoperative CRT has been demonstrated to be effective in local control of tumors and for anal sphincter preservation in large, prospective, randomized clinical trials.23
A prospective German rectal cancer study compared preoperative and postoperative CRT among patients with locally advanced rectal cancer (LARC) and found a dramatic decrease in rate of local recurrence, although no survival benefits, in a preoperative CRT group. A Dutch rectal cancer study compared preoperative short-course radiotherapy followed by surgery with surgery alone and revealed that preoperative short-course radiotherapy decreased the rate of local recurrence; however, it had no survival benefits.2 In contrast, an NSABP R-03 prospective randomized trial compared preoperative versus postoperative CRT for the treatment of LARC and showed survival benefits in the preoperative CRT arm in terms of five-year disease-free survival and overall survival. Interestingly, the five-year locoregional recurrence rate was the same for each treatment arm.4 It is apparent that preoperative CRT has a definite role in disease control and contributes to improved survival in patients with LARC.
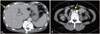
Tumor response to preoperative CRT is evaluated based on tumor (ypT) and nodal (ypN) down staging and tumor regression grade (TRG), which correlate significantly with local recurrence and survival outcomes.56 After preoperative CRT, a wide range of tumor responses has been observed, from complete remission (CR, ypT0N0) to disease progression. If a tumor shows CR after preoperative CRT, we expect an excellent prognosis. According to the literature, 10-30% of patients who receive preoperative CRT show CR, and 60% showed a reduction in tumor size and T and N down staging (Fig. 1A),78 though some patients showed a poor response with little or no tumor reduction (Fig. 1B).56 Furthermore, even though primary rectal cancer showed a dramatic reduction in tumor size and down staging, liver metastasis and systemic lymph node metastasis developed during preoperative CRT (Fig. 2). This discrepancy between tumor responses of the primary tumor and disease progression is sometimes observed.
EVALUATION MODALITIES FOR ASSESSMENT AND PREDICTION OF TUMOR RESPONSE
Various modalities have been studied and proposed to assess and predict responses to CRT. For morphologic assessment of tumor response after preoperative CRT, endoscopic findings and imaging studies, including magnetic resonance imaging (MRI) and positron emission tomography (PET), have been used and demonstrate good results. Clinical factors and serum carcinoembryonic antigen (CEA) have also been investigated and shown to hold some predictive value. Notwithstanding, due to the limitations of these modalities, molecular biomarkers analyzed using immunohistochemistry (IHC) and gene expression profiling have been investigated and may play a possible role as predictive models for tailored treatment of patients undergoing preoperative CRT.
Endoscopic findings
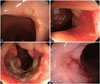
Gross tumor characteristics detected by endoscopy have been suggested for assessment of tumor response after preoperative CRT. Habr-Gama, et al.9 attempted to provide a clear definition of clinical complete response (cCR) after preoperative CRT using endoscopic features. They defined the positive and negative signs for cCR. Positive signs for cCR frequently included whitening of the mucosa, presence of any telangiectasia, subtle loss of pliability of the rectal wall harboring the scar, and no gross evidence of residual tumor. In contrast, positive signs of residual disease included residual deep ulceration, superficial ulcer irregularity, palpable nodule, and significant stenosis (Fig. 3). It was suggested that regularly scheduled reassessments might provide a safe alternative to patients with endoscopic findings of cCR.
Smith, et al.10 conducted a retrospective study of nonoperative management (NOM) of rectal cancer with cCR after neoadjuvant CRT. Thirty-two patients were treated with NOM after cCR. Fifty-seven patients (22%) demonstrated pathologic complete response (pCR) and formed the control group. The NOM group showed six local recurrence cases and concurrent distant recurrences were observed in three cases. Salvage rectal resection controlled all six local failures with no further local recurrence. The pCR group after rectal resection demonstrated no local failures. The two-year distant disease-free survival (88% vs. 98%, p=0.27) and overall survival (96% vs. 100%, p=0.56) were similar between the NOM and pCR after rectal resection groups. Local control without rectal resection was successful in 81% of patients in NOM group. When combined with salvage surgery, NOM achieved similar local and distant disease control compared with pCR after rectal resection.
We performed a prospective study to evaluate the prediction of a pCR based on endoscopic findings in 71 rectal cancer patients after preoperative CRT and following surgical resection (unpublished data). We ventured a hypothesis that no visualization of tumor, white scar, or red scar would be associated with "cCR" and ulcerations and remaining masses of any size would be associated with "non-cCR." Twenty-four (33.8%) patients showed pCR. Of the 23 patients that demonstrated endoscopic cCR, 19 (82.6%) showed pCR. Of the 48 patients that demonstrated endoscopic non-cCR, 43 (89.6%) showed non-pCR. For assessment of pCRs, endoscopic findings exhibited 81.8% sensitivity and 91.8% specificity. Endoscopic findings were significantly correlated with tumor response after preoperative CRT for rectal cancer. Notably, endoscopic cCR showed a high specificity for assessment of pCRs and might be valuable as a predictive tool.
Magnetic resonance imaging (MRI)
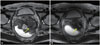
An MRI can be used to indicate tumor response 4-8 weeks after completion of preoperative CRT. MRI has the advantage of detailed and wide view to investigate the pelvic anatomy in advanced rectal cancer patients rather than endorectal ultrasonography.11 Threfore, surgeon can get the more information from MRI after preoperative CRT to decide the resection plan and extent of surgery. Although MRI demonstrate the high accuracy for local staging of rectal cancer without preoperative treatment, the lower accuracy was observed in assessing the ypT stage after preoperative CRT. From the report of pooled data analysis for more than 1500 patients, the disappointing results were observed with a low sensitivity of 50% for assessment of ypT stage, but relatively high specificity of 91%.12 Furthermore, the sensitivity for assessment of ypT0 was only 19%. On the other hand, a higher specificity of 94% was observed.11 The high specificity means that surgeon can select patients who need the radical surgery for remnant tumor even after preoperative CRT. In contrast, patients who have good response can be underestimated and receive more extended surgery without a chance of organ preservation. The findings above suggest that MRI has some limitations to distinguish remnant tumor cells and fibrotic change after preoperative CRT. Small viable tumor cells can be missed or fibrotic tissue can be overestimated to remnant cancer tissue (Fig. 4).
Some reports demonstrated the good performance of MRI volumetric measurements of tumor to assess the tumor shrinkage after preoperative CRT and accuracies was up to 87%.1314 Dresen, et al.13 found that the combination of an initial tumor volume ≤50 cm3 and a ≥75% volume reduction rate on post-CRT MRI predict ypT0-2 with accuracy of 87%. Curvo-Semedo, et al.15 and Ha, et al.16 found areas under the receiver operation characteristic (ROC) curve (AUCs) of 0.70-0.84 for the assessment of pathological complete response with MRI volumetric measurements.
In our previous work, we evaluated the impact of tumor volume changes assessed by three-dimensional (3D) volumetry on tumor response. Eighty-four patients who underwent preoperative CRT followed by radical surgery were prospectively enrolled in the study. The post-treatment tumor volume and tumor volume reduction ratios (% decrease ratio), as shown by 3D MR volumetry, were compared with the histopathologic response. In a multivariate analysis, the tumor volume reduction ratio was not significantly associated with T or N down staging. However, the volume reduction ratio (>75%, p=0.01) was significantly associated with an increased pCR rate.17
To evaluate a good tumor response after preoperative CRT in rectal cancer, some MRI features including invasion depth of tumor, tumor volume, and tumor characteristics were used.131819 No lymph node metastasis, absence of extramural venous invasion, and no evidence of mucinous component, have also been reported to correlate with improved response.1819 Furthermore, MRI features could be a predictive factor of distant metastasis in LARC. Sohn, et al.20 showed that three factors, positive extramural vascular invasion (EMVI), high T stage, and positive regional lymph node metastasis, were significantly associated with synchronous distant metastasis within six months. On their own, these features are insufficient to predict treatment response and plan a tailored treatment strategy individually. However, MRI is definitely meaningful modality for prediction of preoperative CRT as a part of combined model.
Advances in functional magnetic resonance technology combine morphological information with information on the biological microenvironment of the tumor. Functional MRI could provide a more comprehensive picture of tumor heterogeneity and its changes in response to preoperative CRT. Some of these functional technologies have been already used in clinical practice, including perfusion imaging [dynamic contrast-enhanced MRI (DCE-MRI)] and diffusion-weighted MRI (DW-MRI). Other technologies, such as metabolic imaging with MRI (1H, 13C magnetic resonance spectroscopy), are still in the experimental phase.2122
Perfusion MRI and DCE-MRI demonstrate the angiogenic activity of tumor vasculature by measuring the pharmacokinetics of an intravenously administered contrast agent. These perfusion characteristics can be evaluated in a qualitative, quantitative, or semi-quantitative manner.23 The wash-in rate Ktrans is volume transfer content between plasma and extravascular space, and correlated with the permeability of tumor vasculature. Ktrans is the most popular perfusion parameter in quantitative analysis.24 Gollub, et al.25 evaluated the value of Ktrans before and after preoperative chemotherapy for LARC and found a significantly lower post-treatment Ktrans for pCR, compared to that of non-pCR (p=0.04). George, et al.26 and Lim, et al.27 studied the predictive value of pretreatment Ktrans in rectal cancer patients received preoperative CRT and good responder showed a higher Ktrans than poor responder (Fig. 5). Oberholzer, et al.28 also observed same findings that the higher pretreatment Ktrans was correlated with tumor down staging. On the other hand, Devries, et al.29 and Kremser, et al.30 showed that, Ktrans before preoperative CRT was higher in down staging (-) tumors, compared to down staging (+) tumors.
DW-MRI provides qualitative and quantitative information about the basic cellular architecture of the tissue based on differences in movement (diffusion) of water protons within the various tissues. Tissues with high cellular density like malignant tumor show restricted proton movement and an enhanced signal on DW-MRI images. Numbers of studies have reported the efficacy of DW-MRI to distinguish the fibrosis from remnant tumor tissue after chemoradiaton in rectal cancer. According to a meta-analysis, DW-MRI can improve the diagnostic value for the assessment of pCR after preoperative CRT in rectal cancer, with an increase in sensitivity from 19% to 84%. Lambregts, et al.31 reported a effectiveness of DW-MRI for identifying residual tumor and distinguishing non-pCR with a NPV of 90%.
The apparent diffusion coefficient (ADC) is the objective value of DW-MRI. ADC values increase during and after CRT in rectal cancer, which indicate cell death and tumor necrosis. The higher ADC is generally shown in good tumor responders, and a potential predictive biomarker of chemoradiation.32333435 Significant differences of mean ADC after preoperative CRT have been observed between good versus poor responders; however, a substantial variation and conflicting results is also found in several studies.333436
Changes in ADC before and after CRT are also different between responders and non-responders. The research of Jung, et al.34 and of Intven, et al.37 found a significantly greater increase in ADC in responders than in non-responders.35
The value of pretreatment ADC has been studied as a predictor of response to CRT. Sun, et al.32 found that pretreatment mean ADC of patients with good response was lower than that of patients with poor response. In contrast, Barbaro, et al.38 reported a high pretreatment ADC for good responders. Lambrecht, et al.35 and Intven, et al.37 found significantly higher pretreatment ADC values in patients resulting pCR than non-pCR.
In summary, the basis of potential predictive imaging biomarker in rectal cancer after preop CRT is more evident for DW-MRI than DCE-MRI; however, for both, results are drawn mainly from small, single-center studies. Further investigation through prospective large-scale studies and combined manner are needed to find a promising imaging biomarkers of treatment response in rectal cancer.
Fluorine-18-fluorodeoxyglucose (18F-FDG) positron emission tomography (PET)
Fluorine-18-fluorodeoxyglucose (18F-FDG) PET is being increasingly used for staging and evaluating treatment response in oncology. Many researchers studied 18F-FDG PET to assess and predict responses to CRT in rectal cancer, and various parameters have been investigated.394041424344454647 Maximum voxel standardized uptake value (SUVmax) is defined as the ratio of radioactivity concentration to the injected activity divided by body weight. ΔSUV was defined as the SUVmax-pre-SUVmax-post difference, and the percentage decrease between the SUVmax-pre and the SUVmax-post is presented as the response index (RI)=[ΔSUV/pre-SUV]×100. The percentage change in total lesion glycolysis (TLG) before and after CRT (ΔTLG%) is another semi-quantitative parameter. One qualitative parameter related to 18F-FDG PET, visual response (VR), was assessed for predicting pathologic response to preoperative CRT (Table 1).394041424344454647
The diagnostic performances of the three parameters (RI, SUVmax-post, and VR) related to 18F-FDG PET were similar in predicting pathological response. The parameter ΔTLG% had higher specificity than the other three parameters in predicting pathological response.42434445
Most studies have used several parameters but find just one or two to be correlated with CRT response.40414243444547 In our previous study,40 a lower SUVmax-post and a higher RI were shown in good tumor response (T-down staging and TRGs 1 and 2). The SUVmax-post and RI were also significantly associated with pathological treatment response, especially in pCR (Fig. 6). Maffione, et al.46 used eight parameters to predict TRG, and found SUVmax, RI, VR, and ΔTLG% to be significantly correlated with pathological treatment response, with SUVmax-post having the highest sensitivity for predicting TRG.
Janssen, et al.48 studied the optimal time point for repeated 18F-FDG PET during preoperative CRT and the best factor for the prediction of pathological treatment response in patients with LARC. Thirty patients were prospectively enrolled and underwent sequential PET-CT imaging at four time points: prior to therapy, at days 8 and 15 during CRT, and shortly before surgery. Based on TRG evaluations, 13 patients were classified as pathological responders (TRG 1-2), while 17 patients were classified as pathological non-responders (TRG 3-5). The RI for SUVmax on day 15 of CRT was found to be the best predictive factor for pathological response.
At present, many parameters are used to assess response to preoperative CRT. Both RI and SUVmax-post showed a similar sensitivity and specificity for predicting TRG, and pCR and could be suitable indicators of tumor response for preoperative CRT in patients with rectal cancer.40414243444547
Even though several 18F-FDG PET parameters have been used to assess CRT response in LARC, it has clinical limitations. First, the results of the predicting value of 18F-FDG PET are so various and not clear. Second, 18F-FDG has weakness in assessing lymph node metastasis. Third, 18F-FDG PET has difficulty distinguishing between residual cancer and physiologic uptake by inflammation or fibrotic change after CRT. Fourth, the specificity of the predictive value is too low to change or modify the treatment strategy with confidence.
Currently, 18F-FDG PET is not widely available for use as a predictor of tumor response to preoperative CRT. For the optimal prediction of tumor response, it is necessary to coordinate decisions with morphological imaging techniques (TRUS, MRI) and functional techniques (18F-FDG PET). Therefore, multi-institutional prospective studies are needed to determine the feasibility of 18F-FDG PET for the tailored treatment of patients who receive preoperative CRT.
Serum carcinoembryonic antigen (CEA)
CEA is the most widely used tumor marker in patients with rectal cancer. Compared with other potential predictive markers, measurement of serum CEA level is inexpensive, standardized, widely used, and easily performed. In recent years, many studies have focused on the predictive value of CEA level in patients with rectal cancer receiving preoperative CRT (Table 2). Most studies have shown low pre-CRT CEA (CEA-pre) levels with different cut-off values to be associated with good tumor response or pCR, although the results of the CEA-pre predictive values are not consistent.495051525354 Our previous study showed that pretreatment CEA (≤3 ng/mL) is significantly associated with an increased rate of pCR.17
On the other hand, some studies have shown the correlation of post-CRT CEA (CEA-post) level with CR. Perez, et al.,49 Yang, et al.51 did not find a correlation between initial CEA-pre level and pCR, but reported that a CEA-post level <5 ng/mL was associated with increased rates of clinical CR and pCR. CEA-post with a cut-off value of 2.7 ng/mL was also shown to be an independent predictor of good tumor regression. In a recent study, CEA-post <2.61 ng/mL also showed a strong predictive value for pCR, with a sensitivity of 76.0% and specificity of 58.4% in patients with low CEA-pre level or high CEA-pre level but normalized CEA-post level.53
In the first retrospective study of CEA-change as a predictor, a lower CEA-pre level or higher CEA-pre level with a CEA reduction ratio ≥70% was found to have a better five-year DFS.50 However, it was unknown whether or not this ratio was related to pCR. To ensure that the CEA ratio (defined as CEA-post divided by CEA-pre) can be used as a predictor for pCR, Yang, et al.51 noted that when CEA-pre level ≥6 ng/mL, the CEA ratio was a significant predictor of pCR, and the optimal cutoff value of CEA ratio was 0.22 with a sensitivity of 87.5% and specificity of 76.7%.
Compared with other potential prognostic and predictive markers, measurement of serum CEA level is inexpensive, widely used, and easily performed; however, different studies have used different cut-off values, and most studies did not provide the sensitivity or specificity of CEA-post as a predictor of CRT response.
Molecular biomarkers
Many molecular markers have been assessed for evaluation and prediction of tumor response to preoperative CRT in patients with rectal cancer according to IHC or direct gene sequencing analysis. More than 40 different biomarkers have been explored in the literature, with conflicting results in predicting the outcomes of CRT (Table 3). Some of the more promising markers are discussed below.
One of the most extensively studied markers is the tumor suppressor p53. It plays a vital role in the regulation of the cell cycle and is important for genetic stability, cell proliferation, apoptosis, and inhibition of angiogenesis. Previous studies have shown that nuclear expression of p53 in rectal cancers is predictive of treatment failure and that detection of nuclear p53 using IHC is correlated with resistance to pre-operative CRT. 5556 Of 21 studies examined, 17 found no correlation between p53 expression and any survival or outcome measure. Chen, et al.57 (n=130) and Bertolini, et al.58 (n=91) published studies of large sample sizes and revealed no correlation between mutant p53 expression and treatment outcomes. However, other studies did find a correlation between p53 and treatment outcome. Lin, et al.59 (n=70) determined that pre-treatment tumor biopsies negative for p53 are predictive of complete tumor regression or only tumor in situ in surgical specimens (p=0.006). Spitz, et al.60 (n=42) found a relationship between samples lacking p53 staining and improved histopathologic response to preoperative CRT (p=0.02) and a direct relationship between p53 positive-staining samples and residual disease detected within lymph nodes (p=0.02). In contrast, Esposito, et al.61 (n=38) found that pre-treatment biopsies (PTB) showing strong expression of p53 were associated with better responses to preoperative CRT. Our results are consistent with studies showing an association between strong p53 positivity and tumor resistance to CRT, and our multivariate analysis identified p53 as an independent predictor of pCR.62
Wild-type p53 protein induces the expression of p21, a product of the WAF1/CIP1 gene. Charara, et al.63 (n=57) and Rau, et al.64 (n=66) both found that p21 expression is associated with a good/complete response. On the other hand, Reerink, et al.65 (n=34) found higher p21 expression to be associated with poorer survival, while Bertolini, et al.58 (n=91) found no correlation between p21 expression and pathological response, though they did find a reduction in disease-free survival with high p21 expression. In our cohort, strong expression of p21 was observed significantly more often among good responders and was significantly associated with pCR.62
Ki-67 has been used to assess cell proliferation and activity and can be detected in all active stages of the cell cycle; two previous studies showed an association between Ki-67 and treatment response. Our earlier study66 (n=23) showed that good treatment responders have a higher Ki-67 index (number of Ki-67 staining tumor cells per 1000 cells), whereas Jakob, et al.67 (n=22) showed the opposite. In our cohort, Ki-67 index was significantly higher in good responders, as determined based on ypTNM, T-down staging, N-down staging, TRG, and pCR. Furthermore, Ki-67 was an independent predictor of pCR. Other studies have found no association between Ki-67 expression in PTB and any measure of outcomes.6268
The bax and bcl-2 proteins belong to the bcl-2 subset of oncogenes involved in the apoptosis pathway. One of the three studies examining bax expression and outcome in preoperative CRT treatment have revealed a significant correlation.69 Chang, et al.70 (n=130) found that the complete-response group had 54% bax-positive pretreatment tumor biopsies, compared with 29% bax-positive biopsies in the partial-response group (p=0.017). More studies evaluating bax as a predictive biomarker are needed to remedy the limited data available. Of 12 total studies that evaluated bcl-2's potential as a predictive biomarker of treatment response, only one revealed a correlation. Kudrimoti, et al.71 (n=17) found that 60% of the complete responders were bcl-2 positive on pretreatment biopsy staining, compared with 16% bcl-2 positive in the partial responders group (p=0.04). Survivin is another antiapoptotic molecule that inhibits members of the caspase family of enzymes. Sarela, et al.72 (n=49) showed a correlation between survivin expression and decreased survival.
Angiogenesis is essential for tumor growth and survival. Therefore, vascular endothelial growth factor (VEGF) is a subject of investigation in cancer biology. Tumor hypoxia can induce resistance to radiation and chemotherapy by depriving cells of oxygen essential for the cytotoxic activities of these agents. Only one marker for hypoxia, VEGF, has been assessed as a response predictor in rectal cancer.73 Qui, et al.74 examined VEGF expression in PTB from 72 patients undergoing longcourse preoperative radiotherapy; they found that the histological response was unrelated to pre-treatment VEGF status. In contrast, we observed that VEGF expression levels were predictive of pCR; that is, tumors strongly expressing VEGF on tissue microarray (TMA) responded significantly better to CRT than did those with weak expression.
COX 2 is an important mediator of tumor invasiveness and metastasis. Smith, et al.75 assessed endogenous COX 2 expression in PTB of 49 patients undergoing preoperative CRT for rectal cancer. Patients with COX 2 overexpression in PTB were more likely to demonstrate poor response to RCT (TRG 3 and 4) than were those with normal COX 2 expression (p=0.026). Our study also demonstrated that patients with COX 2 overexpression were more likely to show a poor TRG and were less likely to achieve histopathologic nodal down staging (p=0.03) than those with normal COX 2 expression.76
Epidermal growth factor receptor (EGFR) is expressed in 50 to 70% of cancers, and therapies targeting this and related pathways are increasingly being developed for translational trials. Giralt, et al.77 (n=87) found that a significantly higher number of EGFR-negative patients achieved pCR, compared with EGFR-positive patients. Using multivariate analysis, Kim, et al.78 (n=183) found that low EGFR expression significantly predicts increased tumor down staging with therapy. Spindler, et al.79 (n=60) found that tumors involving replacement of G with a T nucleotide at position 216 of the EGFR promoter (GT or TT genotypes) demonstrated improved response, compared with tumors with a GG genotype.
Thymidylate synthase (TS), located on chromosome 18p11.32, is an essential enzyme for cell proliferation and deoxyribonucleic acid (DNA) synthesis. Several studies have evaluated the efficacy of TS as a predictor of treatment response after CRT in rectal cancer. Okonkwo, et al.80 (n=25) and Saw, et al.69 (n=60) determined that PTB negative for TS were predictive of tumor down staging in the CRT group (n=35). In contrast, Negri, et al.81 demonstrated that PTB demonstrating high TS staining intensity had significantly more complete and partial responders than those exhibiting low TS staining intensity (88% vs. 12%) in the CRT group (n=19). We investigated the correlation of TS gene expression and polymorphisms with tumor response to preoperative CRT in 44 patients with LARC. Patients exhibited 2R/3R and 3R/3R tandem repeat polymorphisms in the TS gene. In regard to TS expression in these genotypes, 2R/3RC and 3RC/3RC were defined as the low expression group and 2R/3RG, 3RC/3RG, and 3RG/3RG as the high expression group. Patients in the low expression group with a G>C single-nucleotide polymorphism (SNP) (2R/3RC, 3RC/3RC) exhibited a significantly greater tumor down staging rate, compared with patients in the high expression group without the SNP (2R/3RG, 3RC/3RG, 3RG/3RG) (p=0.001). The nodal down staging rate was also significantly greater in this low expression group, compared with that of the high expression group.82
Cancer stem cell markers
CD133, CD44, and CD24 have been widely known as colorectal cancer stem cell markers. Cancer stem cell has the characteristics of resistance to chemotherapy and radiotherapy. Therefore, there have been some efforts to investigate the correlation of cancer stem cell markers with the treatment response to CRT. CD133 expression means the existence of cancer stem cell and high level is correlated with resistance to CRT in LARC.83 The level of CD24 was also found to be significantly associated with CRT response in some reports. Huh, et al.84 revealed that, among 13 molecular markers, only elevated CD44 mRNA level in PTB was predictive of poor tumor regression, and CD133 level had no significant correlation with CRT response. Until now, there is no confirmative result that cancer stem cell marker is predictive of CRT response and useful in clinical field. More investigation is needed to develop predictive model using cancer stem cell markers.
Gene expression profiling
To overcome the limitation of single specific markers for predictability, DNA microarray-based gene expression profiling technology have been used to analyze a large number of genes simultaneously and to search systematically for molecular markers to predict CRT responses and outcomes (Table 4).8586 Ghadimi, et al.87 used two different microarray platforms to analyze PTB, and identified 54 genes that were significantly differentially expressed between responders and non-responders based on T down staging. The genes were able to correctly predict tumor behavior in 83% of patients.
Watanabe, et al.88 studied gene expression profiles, and identified 33 novel discriminating genes whose expression differed significantly between responders and non-responders among 52 rectal cancer patients who underwent preoperative CRT. Using that gene set, they established a new model to predict responses to CRT in rectal cancer with an accuracy of 82.4%. The list of discriminating genes included those related to growth factors, apoptosis, cell proliferation, signal transduction, and cell adhesion. Among the 33 discriminating genes, apoptosis inducers (lumican, thrombospondin 2, and galectin-1) showed higher expression in responders, whereas apoptosis inhibitors (cyclophilin 40 and glutathione peroxidase) showed higher expression in non-responders. In a subsequent study, Watanabe, et al.89 initially identified differently expressed genes between responders and non-responders using microarray analysis. Quantitative reverse transcriptase polymerase chain reaction was performed to validate the microarray expression levels of the discriminating genes, and the 16 genes showed a difference in expression between responders and non-responders after preoperative CRT. They constructed a predictive model using different sets of these 16 genes, and the highest accuracy rate (89.1%) was obtained using LRRIQ3, FRMD3, SAMD5, and TMC7. The predictive accuracy rate of this fourgene signature in an independent set of 16 patients was 81.3%.
Kim, et al.90 also investigated whether microarray gene expression analysis predicted complete response to preoperative CRT in patients with rectal cancer. The reported an accuracy of greater than 80%.
Microarray gene profiling seems to be ideal for identifying overall molecular markers that predict response to CRT. However, although each study has shown the promising results with predictive genes for CRT response, there are several limitations for the use of microarray in clinical practice. Most important aspect is the absence of uniformity of reported gene signatures among studies. The reproducibility is essential for use in clinical practice and simplicity is also needed. Microarray is still insufficient for these practical aspects. The difficulty of fresh tissue handling and high cost is also limitation. However, considering the promising data and usefulness of gene profiling in breast and lung cancer, gene expression profiling holds considerable promise to identify the underlying complex genetics of responses to CRT of rectal cancer if candidate genes are carefully validated.
Single-nucleotide polymorphism (SNP) markers
Genome-wide association studies (GWA) are theoretically capable of identifying predictive markers of CRT response despite of discordance among studies. SNP analysis has been used to investigate special gene sites in order to predict responses to CRT. Furthermore, thousands of SNPs can be identified by GWA studies. A recent study proposed a novel threestep approach to the identification of CRT-responsive patients based on genome-wide screening, clinical association, and biological validation of SNP markers.90 Of 691.162 SNPs analyzed in the first step using 43 patients, 9 candidate CRT-responsive SNPs, including USP20 rs227450, FAM101A rs7955740, ZNF281 rs424414, OR2T4 rs153870, SLC10A7 rs41398848, CORO2A rs1985859, ASZ1 rs7808424 MED4 rs157125, and CDC42BPA rs192986 were selected. In the second step, the above nine candidate SNPs were genotyped by pyrosequencing using genomic DNA samples from the 43 initial screening patients and 70 additional patiens for clinical validation and two candidate markers were identified. Positive response (TRG 1-3) were obtained more likely in patients carrying the reference allele (C) of the SNP CORO2A rs1985859 than in those with the substitution allele (T).90 Flow cytometry determined the significant association between downregulation of CORO2A and reduced early apoptosis in colorectal cancer cells. Reduced radiosensitivity was also confirmed by colony-forming assays in the same cells in the third step. Otherwise, any genotype or allelotype of SNP FAM101A rs7955740 was not associated with radiosensitivity in the clinical association analysis. However, downregulation of FAM101A significantly reduced early apoptosis and enhanced colony formation in colorectal cancer cells.
Despite the controversial findings in the study and poor concordance between GWA studies, the finding is novel, and SNPs are worth further validation in large cohorts.
FURTHER INVESTIGATIONS AND ONGOING STUDIES
Dynamic analysis using sequential evaluation
Dynamic change of molecular marker value was studied to be correlated with the response to CRT by sequential biopsies of rectal cancer. In one study, biopsies were taken before treatment, after 2, 4, and 6 weeks of CRT and in specimens from the operation. Decreasing expressions of hypoxia-inducible factor 1α, bcl-2, and Ki-67 were observed during CRT, whereas glucose transporter-1 overall was unchanged. No significant changes of the markers were observed in the interval between CRT and surgery. A significant association was observed between the presence of residual carcinoma after 6 weeks of treatment and pathological response to CRT, but no association was seen between the fluctuations of any of the markers and response to CRT.91 In another study immunohistochemical expressions of p21 and apoptosis together with histologic changes on H&E stained biopsy specimens obtained 7 days after starting CRT are strong predictors of response to CRT.72 Microrray analysis of tumor biopsies after a dose of 7.2 Gy at a median time of 1 hour following irradiation efficiently assessed early transcriptomic changes during preop CRT. Up-regulation of 31 genes and down-regulation of six genes was shown.92 These studies demonstrate that early or serial evaluation of treatment response is more accurate and promising rather than only before or after CRT. However, biopsy procedure is invasive may be harmful to be performed serially. Therefore, non-invasive tools like MRI, PET-CT, and CEA can safely evaluate dynamic changes of response in rectal cancer during CRT.93 However, PET-CT is too expensive to be performed repeatedly, and numbers of patients show the normal CEA value before CRT and the significant change would not be expected. A study including 20 patients who underwent MRI including DWI before CRT, after 10-15 fractions and 1 to 2 weeks before surgery demonstrated that ΔADC-during and after CRT was significantly higher in patients with pCR, compared to patients without.35 Above findings indicate that sequential evaluation modalities may be more useful for prediction and early assessment of treatment response to preop CRT of rectal cancer than only one-time evaluation.
Multidirectional evaluation model
Each predictive marker has its own strength and weakness, therefore, a combination of two or more predictive models may improve its predictability of treatment response after preop CRT in rectal cancer. In one prospective study, the combination of PET-CT and DW-MRI was investigated for the prediction of pCR after CRT in rectal cancer.94 Twenty-two patients underwent PET/CT prior to the start of CRT, after 10 to 12 fractions of CRT and five weeks after the end of CRT. A DW-MRI was performed before start of CRT. ΔSUVmax during and after CRT significantly correlated with pCR after CRT. The initial ADC value was also significantly correlated with pCR. ROC curve analysis revealed an optimal threshold for ΔSUVmax of 40% during CRT and 76% after CRT, as well as for ADC value of 1.06×103 mm2/s. Combining the provided ΔSUVmax thresholds during and after CRT increased specificity of the prediction (sensitivity 100% and specificity 94%). The combination of the thresholds for the initial ADC value and the ΔSUVmax during CRT increased specificity of the prediction to a similar level (sensitivity of 100% and specifi city of 94%).
Maas, et al.95 evaluated the feasibility and safety of a waitand-see policy among patients without residual tumor on imaging or endoscopy (cCR) after preoperative CRT for rectal cancer.95 The definition of cCR is 1) substantial downsizing with no residual tumor or only residual fibrosis (with low signal on high b-value DWI, if available). Residual wall thickening due to edema was also an indication for possible cCR, as were 2) no suspicious lymph nodes on MRI; 3) no residual tumor at endoscopy or only a small residual erythematous ulcer or scar; 4) negative biopsies from the scar, ulcer, or former tumor location; and 5) no palpable tumor, when initially palpable with digital rectal examination. If patients did not meet all of these criteria, they were regarded as non-complete responders. Twenty-one patients with cCR were included in the wait-and-see policy group. Mean follow-up was 25±19 months. One patient developed a local recurrence and underwent surgery as salvage treatment. The other 20 patients are alive without disease. The control group consisted of 20 patients with pCR after surgery with a mean follow-up of 35±23 months. For these patients, the cumulative probabilities of two-year disease-free survival and overall survival were 93% and 91%, respectively. The authors concluded that a wait-and-see policy with strict selection criteria, up-to-date imaging techniques, and follow-up is feasible, and results are promising with outcomes at least as good as those of patients with pCR after surgery.
The availability of simple, financially feasible, and high-throughput technology such as TMA-based IHC provides an opportunity to develop a panel of biomarkers. To this end, we evaluated the differential expressions of molecular markers in TMA constructs from stage II/III rectal tumors (n=81) in patients treated with preoperative CRT.62 Using TMAs and IHC, expression levels of 12 candidate biomarkers (p53, p21, bcl-2, Bax, EGFR, COX 2, MLH-1, MSH-2, Ku70, VEGF, TS, Ki-67) were evaluated in paraffin-embedded tumor samples collected before preoperative CRT. The correlations between biomarker expression level and pathologic response to preoperative CRT were assessed based on histopathological staging (pTNM) and TRG. Expression levels of four biomarkers (p53, VEGF, p21, Ki-67) were correlated with pCR. Patients showing low expression of p53 and/or high expressions of VEGF, p21, or Ki-67 exhibited a significantly greater pCR rate. A scoring system devised so that one point was assigned for each biomarker whose expression level was correlated with pCR (score range: 0-4) showed that 1 of 26 patients with scores of 0-1 achieved pCR, whereas 26 of 55 patients with scores of 2-4 achieved pCR (3.8% vs. 47.3%, p<0.001). For prediction of pCR, the scoring system showed 96.3% sensitivity, 46.3% specificity, a 47.3% positive predictive value, and a 96.2% negative predictive value.
To date, there have been several attempts to develop models or nomograms to predict the outcomes of cancer treatment. Keam, et al.96 suggested nomograms predicting clinical outcomes in breast cancer patients treated with neoadjuvant chemotherapy. They developed the nomograms using a logistic regression model for pCR and a Cox proportional hazard regression model for relapse-free survival. The nomogram for pCR based on initial tumor size, estrogen receptor (ER), human EGFR 2, and Ki-67 had good discrimination performance. A multivariate Cox model identified age less than 35 years, initial clinical stage, pathologic stage, ER, and Ki-67 as prognostic factors, and the nomogram for RFS showed good performance.
Jwa, et al.97 assessed a nomogram to predict ypN status after preoperative CRT in rectal cancer. The nomogram was developed in a training cohort (n=891) using logistic regression analyses and was validated in a separate cohort (n=258). Patient age, preoperative CRT tumor differentiation, cN stage, ypT stage, lymphovascular invasion, and perineural invasion were reliable predictors of lymph node metastasis after preoperative CRT and were used for the construction of the nomogram.
As shown in above published studies, a combination of two or more modalities provided complementary information about treatment response and yielded higher accuracy and specificity than the individual investigations. The combination of morphological and functional imaging with the numerous potential molecular markers and identified genes will provide comprehensive information on each individual patient and make possible individualized treatment therapy. Combined models may be the future trend for predicting treatment responses.
CLINICAL APPLICATION OF A PREDICTIVE MODEL FOR PATIENTS WHO RECEIVED PREOPERATIVE CRT
Currently, there is no definite method to predict a tumor response to CRT; however, the ability to do so would be of significant clinical advantage for several reasons. First, CRT is time-consuming, expensive, and increases perioperative morbidity. The ability to predict a response, either before treatment or during its early stages, could exclude patients who might show poor response and disease progression without benefit. Instead, these patients would be candidates for alternative or more intensive treatment strategies. Recently, systemic chemotherapy was offered as initial treatment for patients with high-risk LARC in order to target micrometastasis and improve tumor response before conventional CRT. Additional chemotherapy before CRT and total mesorectal excision resulted in substantial tumor regression, rapid symptomatic response, and achievement of R0 resection.9899100 Second, prediction of complete tumor remission has been regarded as important, because it impacts clinical decisions for treatment strategy. In cases of cT4 middle or lower rectal cancer that represent invasion of an adjacent pelvic organ, such as the seminal vesicles, prostate, vagina, or anal sphincter complex, if CR of rectal cancer after preoperative CRT can be predicted, en bloc resection of the adjacent pelvic organ or anal sphincter, which results in increasing postoperative morbidity and poor quality of life with stoma, can be avoided. In addition, local excision or wait-and-see treatment strategies can be recommended if the tumor shows an excellent tumor response to preoperative CRT for rectal cancer. According to a retrospective analysis of patients who had received preoperative CRT, ypT0 only has a 5% rate of regional lymph node metastasis. However, patients who demonstrate adjacent organ involvement and circumferential margin threatening could be considered for extended surgery or additional radiation therapy for curative resection (Fig. 7).
The above-mentioned modalities can guide clinicians in choosing the best possible treatment for each individual patients. Nevertheless, there are still controversies regarding outcomes of each study; in the future, combined models might better predict response. The ability to predict pathological tumor response before treatment will significantly impact patient selection for preoperative CRT and can potentially modify treatment strategies.
SUMMARY AND CONCLUSION
The wide range of responses to CRT and its potential toxicity generated the investigations to find predictive markers and develop an individually treatment model for better outcomes in rectal cancer. To use predictive tools for treatment plan and clinical practice, the accuracy and effectiveness of markers should be proved. However, the clinical application of these potential predictive markers is still far and the evidence is insufficient.
In this review, we provided an overview of different predictive methods. The MRI, 18F-FDG PET, CEA, and molecular biomarkers each have potential for predicting responses to CRT. However, several methods for prediction of tumor responses after CRT have shown some limitations in accuracy. Therefore, a nomogram for prediction of tumor response with high accuracy is needed using multiple evaluation tools, including relevant molecular markers.
In the future, when highly accurate predictive tools for good tumor response are developed, patients who will benefit from preoperative CRT can be identified and treated with individualized methods. Furthermore, if ypT0 can be predicted in lower rectal cancer, the extent of surgery can be determined with great confidence.








 XML Download
XML Download