

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Deep vein thrombosis (DVT) is a major medical problem characterized by thrombi formation in the deep venous system and can result in a fatal pulmonary embolism (PE). DVT occurs most commonly in the legs, although thrombi can also form in the veins of the arms as well.1 In the United States, DVT and PE result in up to 600000 hospitalizations a year, and nearly 50000 individuals die annually as a result of PE.2
Hip arthroplasty, knee arthroplasty, and hip fracture orthopedic surgeries are strongly associated with a risk of developing DVT.2,3,4 The incidence of asymptomatic DVT after a major orthopedic surgery without prophylaxis reportedly ranges from 30% to 80%,2,5,6 whereas the incidence of symptomatic DVT reportedly ranges from 0.5% to 4%.4,7 Although the incidence of asymptomatic DVT is greater than that of symptomatic DVT, the clinical importance of asymptomatic DVT remains unclear.8,9 Indeed, asymptomatic DVT rarely causes symptomatic PE and most asymptomatic DVT cases include isolated DVT of the calf that is usually detected by venography.10 However, estimates indicate that 40-50% of untreated symptomatic DVT patients will develop a PE within 3 months and 10% of symptomatic PE cases will die within 1 hour of onset.10,11 Therefore, as the objective of DVT prevention is to prevent fatal PE, elucidating the incidence of symptomatic DVT, as a surrogate marker for PE, is of critical importance.
Hip and knee arthroplasties rank high among the most successful surgeries performed in the orthopedic field, and approximately 1 million arthroplastic surgeries are performed annually in the United States or Europe.12,13 Although, orthopedic surgeons are encouraged to consider the development of DVT, there are no nationwide reports on the incidence of symptomatic DVT after major orthopedic surgery. In the present study, we aimed to use a national claim registry to evaluate the incidence and risks factor for the development of symptomatic DVT after major lower limb orthopedic surgery. We also attempted to evaluate whether the incidence of postoperative DVT varies among major orthopedic operations.
MATERIALS AND METHODS
The present study was exempt from Institutional Review Board review because it did not involve human subjects.
Data source and study population
We investigated the incidence of DVT from 2007 to 2011 using a nationwide database maintained by the Korean Health Insurance Review and Assessment Service (HIRA). The HIRA is a non-profit agency that is responsible for reviewing medical fees, as well as evaluating the appropriateness of health care services provided to health insurance beneficiaries. Approximately 97% of the Korean population is obliged to enroll in the government-operated National Health Insurance (NHI) program, which is the only public medical insurance system. There are no exceptions for unemployed or part-time workers. Patients typically pay approximately 30% of the medical cost, and hospitals or clinics submit claims, with details on diagnostic codes, demographic and medication data, operation codes, and operative records, to the NHI for the remainder of the medical cost. Importantly, the HIRA database contains claim records from all medical facilities in Korea. The remaining 3% of population not insured by the NHI program are either covered by the Medical Aid Program of Korea or are illegal residents; claims from these patients are also reviewed by the HIRA. Therefore, a nationwide study was possible given that every claim record, along with its diagnostic code, is electronically collected via the HIRA database. According to the HIRA database, 99.9% of Koreans were registered in 2009.
Data collection
We identified DVT cases using the International Classification of Diseases (ICD-10) system. The codes for DVT were I80.2 [DVT, not otherwise specified (NOS)] and I80.3 (embolism or thrombosis of the lower extremity, NOS). Major orthopedic procedures of the lower limbs were identified using the HIRA operation code classification system. Hip arthroplasty, knee arthroplasty, and hip fracture surgeries were considered as major lower limb orthopedic procedures. Hip replacement arthroplasty included total hip replacement arthroplasty, revision total hip replacement arthroplasty, and bipolar hemiarthroplasty. Knee replacement arthroplasty consisted of total knee arthroplasty, revision total knee arthroplasty, unicompartmental knee replacement arthroplasty, and revision for unicompartmental knee replacement arthroplasty. Hip fracture surgery included closed reduction of the femur, open reduction of the femur, and external fixator application for the femur and the pelvic bone. Postoperative DVT was considered in cases where the DVT codes were claimed within 4 weeks postoperatively.
Incidence of DVT and the rates of major orthopedic surgeries
Demographic data (e.g., gender and age) were obtained from the HIRA database. We divided the subjects into 10-year age groups. The crude annual incidence of DVT was calculated using the number of patients with DVT and the total Korean population for the respective year. The annual incidence of DVT according to age was also calculated. As there were differences in the population size for each year with regard to age and gender, the age- and gender-adjusted annual incidence of DVT was also calculated, after adjusting with the 2009 population.
The age- and gender-adjusted rates of major orthopedic surgeries in the South Korean population from 2007 to 2011 were calculated. The data for knee replacement arthroplasty was evaluated from 2008 to 2011. The postoperative incidence of DVT according to the surgical procedure was also assessed.
Statistical analysis
The surgery rate per 100000 persons/year and the 95% confidence intervals were calculated on the basis of the Poisson distribution for the observed number of DVT cases. The relative risk of DVT between genders for the different surgeries was assessed using the ratio of these rates, along with 95% confidence intervals. Data were analyzed using SPSS Statistics, version 20.0, for Windows (IBM Co., Chicago, IL, USA). All statistics were two-tailed and all p-values less than 0.05 were considered statistically significant.
RESULTS
The population of South Korea in 2007 was approximately 50,000,000 and increased annually until 2011. The population comprised a greater number of males than females (Table 1).
When adjusted for age and gender, the overall annual incidence of DVT was 70.67 per 100000 persons/year, and this value annually increased during the 5-year period of the study. DVT incidence also increased with age (Fig. 1). Indeed, when compared to patients aged <49 years, the relative risk of DVT was five times higher in patients aged 50-69 years and 10 times higher in patients aged >70 years (p<0.001). Interestingly, females showed a greater relative risk for DVT than males (p<0.001) (Table 2).
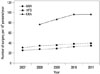
From 2007 to 2011, 89710 hip replacement arthroplasties and 75328 hip fracture surgeries were performed, whereas 180611 knee replacement arthroplasties were performed from 2008 to 2011. The annual number of the major orthopedic surgeries increased over the 5 years of evaluation (Fig. 2). The relative risk for major lower limb orthopedic surgery was higher in females than in males. The relative risk for hip replacement arthroplasty and hip fracture surgery in females was 1.54 [95% confidence interval (CI), 1.38-1.70] and 1.66 (95% CI, 1.47-1.85), respectively. Females were also more likely to require knee replacement arthroplasty than males (relative risk, 7.45; 95% CI, 6.90-8.00) (Fig. 3).
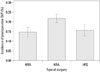
The overall incidences of DVT in patients undergoing hip replacement arthroplasty, knee replacement arthroplasty, and hip fracture surgery were 0.15%, 0.22%, and 0.16%, respectively. Furthermore, the relative risk of DVT after a major lower limb orthopedic surgery increased with age. Compared with the patients aged 20-49 years, the relative risk in the older age groups increased from 1.2- to 2.8-fold. The incidence of postoperative DVT according to the type of surgery was significantly higher for knee replacement arthroplasty, compared to those for hip replacement arthroplasty and hip fracture surgery (p<0.002) (Table 3, Fig. 4). The relative risk for DVT was higher in females than in males for knee replacement arthroplasty (relative risk, 1.47) and hip fracture surgery (relative risk, 2.25) groups. However, for hip replacement arthroplasty, the relative risk in females (relative risk, 0.97) was similar to that in males.
DISCUSSION
This study is the first nationwide investigation of DVT after major lower limb orthopedic surgery. The age- and gender-adjusted annual incidence of DVT was 70.67 per 100000 persons/year, and this value showed an annual increase over the 5-year period examined. Additionally, the incidences of postoperative DVT for hip replacement arthroplasty, knee replacement arthroplasty, and hip fracture surgeries were 0.15%, 0.22%, and 0.16%, respectively.
The definition of postoperative DVT varies among studies in the literature. DVT has been reported to occur up to 3 months postoperatively.14,15 However, most thromboembolic events after elective orthopedic surgery are reported to develop during the first postoperative week.16,17 In patients who develop DVT after 4 weeks postoperatively, the causal relationship between surgery and DVT is not clear. Therefore, we defined postoperative DVT as DVT that developed within 4 weeks postoperatively.
The age- and gender-adjusted nationwide annual incidences of DVT in the present study are comparable, or slightly lower, than those of previous reports from Western populations.18,19 Interracial differences,20 genetic factors, and a Western lifestyle may affect the incidence of DVT. Indeed, the adoption of a Westernized lifestyle, the aging population of South Korea, and the development of new diagnostic tools may have contributed to the annual increases in the incidence of DVT in the current study. However, research is lacking on these issues and future investigations regarding ethnic, genetic, and lifestyle factors are required.
Old age is a well-known risk factor for DVT, which was also confirmed in our study.18,21,22 Moreover, elderly individuals are more likely to require a major operation or may be immobilized due to medical problems. Our current findings also showed that females are at a greater risk for DVT and postoperative DVT; no consensus has been reached regarding differences in the incidence of DVT according to gender in previous studies.19,23,24
Orthopedic surgery is a well-known risk factor for DVT. The release of thromboplastin from the dissected soft tissue and reamed bone, as well as venous stasis during surgery and postoperative immobility, are responsible for high rates of DVT.13 The rate of all of the major lower limb orthopedic surgeries that were evaluated in this study increased annually, and this trend is similar to those reported in previous studies.12,25 As mentioned above, an aging population and economic growth may have contributed to increases in the rate of major orthopedic surgeries. Furthermore, both kneeling and squatting are strong risk factors for degenerative arthritis of the knee. Koreans commonly kneel or squat throughout their daily activities. This cultural characteristic greatly increases the likelihood of needing a surgery, and therefore, maintaining knee flexion (which enables kneeling and squatting) may be an important factor when deciding to undergo surgery in Koreans.12
Interestingly, we found that knee replacement arthroplasty cases showed the highest incidence of postoperative DVT. Previous Asian studies of major orthopedic surgeries, followed by venography, have shown similar results.6,26 Although these previous investigations focused on the incidence of postoperative asymptomatic DVT, whereas we evaluated symptomatic DVT, it is important to note that the highest rate of proximal DVT was also observed in knee replacement arthroplasty patients.6 Given that proximal DVT is associated with a higher risk of embolization, compared to distal DVT,27 the incidence of DVT after knee replacement surgery should be considered very carefully. Overall, as the rate of major orthopedic surgeries increases, the incidence of postoperative DVT will also likely increase.
Several limitations of the current study should be considered. First, the data were retrieved according to diagnostic codes and not on an individual patient basis. Therefore, we could not evaluate whether the DVT cases were recurrent in the same patient and year. The cause of arthroplasty, which varies between patients and might affect the incidence of DVT, could also not be evaluated. In addition, cases of bilateral surgery could not be examined. However, we believe that the current diagnosis-based results, compared to those obtained on per patient basis, allow for better assessment of the actual incidence of postoperative DVT because this information contains every case of DVT, regardless of the number of times the patient had presented. Second, the DVT prophylaxis regimen and prevention programs may have affected the outcomes of our study, and given the nature of the study of an entire nation, we cannot assure the homogeneity of the prophylaxis protocol. The current data do not represent the actual incidence of postoperative DVT without prophylaxis, which is reported to be in the range of 30% to 80%.2,5 Third, in current practice, DVT can be diagnosed using ultrasonography, venography, or CT angiography. As the sensitivity of venography is substantially higher than that of ultrasonography, the diagnostic method could affect the incidence of DVT.28 Unfortunately, our data do not include information regarding the diagnostic method.
Our results showed that the incidence of DVT and postoperative DVT after major lower limb orthopedic surgeries have increased annually. Old age, female gender (except after hip replacement arthroplasty), and knee replacement arthroplastic surgery (0.22%) were associated with a higher risk of developing postoperative DVT. Therefore, orthopedic surgeons should carefully consider the risk factors of DVT before performing major orthopedic surgeries and should remain aware of the possibility of the development of DVT after surgery in high-risk patients.





 XML Download
XML Download