

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
For pediatric patients with end stage renal disease (ESRD), the ultimate goal of treatment is successful kidney transplantation. Until a donor kidney is provided, most patients require a period of dialysis before renal transplantation.1
Peritoneal dialysis (PD) has been performed without major complications in children who need renal replacement therapy. However, several infectious or noninfectious complications may occur in continuous ambulatory peritoneal dialysis (CAPD). Although infectious complications of PD have been frequently reported, the data for noninfectious complications of PD have not been sufficiently reported in children.2345678910 The management of noninfectious complications of PD is highly dependent on the nephrologist's experience, but it is important to establish proper treatment for noninfectious complications of PD. Early detection and intervention will play an important role in decreasing the mechanical failure and patient morbidity associated with PD.2 Globally, there have been few studies on the mechanical complications of PD,6789 and there was no report regarding comprehensive metabolic complications in Korea and other Asian countries. Therefore, we aimed to investigate noninfectious complications of PD, including both mechanical and metabolic complications, in Korean children at a single center.
MATERIALS AND METHODS
Data from all children who had received PD at Severance Hospital between June 1, 1986 (when detailed medical data were available) and December 31, 2012 were reviewed retrospectively. Sixty patients (40 male and 20 female) who had initiated PD before or at the age of 18 years were selected for this study. Fifty-seven patients who received PD before December 2011 were analyzed in our another study on peritonitis.5 The follow-up duration was defined as the period from the initiation of PD to the date of switching to hemodialysis (HD), renal transplantation, or death. The collected data included gender, age at the start of PD, underlying causes of PD, noninfectious complications, duration of CAPD, treatments for complications, and change of modality.
Laboratory data before the year 2000 were not available for metabolic complications; thus, we obtained the serum glucose, sodium, potassium, and calcium levels of 21 patients (from 2000 to 2012). We excluded five patients who received HD and continuous renal replacement therapy. Hyperglycemia was defined as a fasting serum glucose level above 126 mg/dL. Hyponatremia was defined as a serum sodium concentration <135 mmol/L, and hypernatremia was defined as >145 mmol/L. Hypokalemia was defined as a serum potassium level <3.5 mmol/L, and hyperkalemia was defined as >5.5 mmol/L. Hypocalcemia was defined as a serum calcium level <2.13 mmol/L, and hypercalcemia was defined as >2.63 mmol/L.
Among 60 patients treated by CAPD at our center during the period, a total of 70 catheters were used for treatment. Possible causes for switching to HD or catheter reinsertion were recorded. Two-cuffed straight Tenckhoff catheters were placed in all patients by using the downward-facing tunnel method. CAPD was initiated two weeks postoperatively in elective situations. Dialysate was composed of 1.5%, 2.5%, and 4.25% dextrose PD fluid and was selected according to the volume status of each patient.
Continuous variables were expressed as the mean±standard deviation or medians with ranges and were analyzed by the Mann-Whitney U test. Categorical variables were expressed as frequencies and percentages and were analyzed by chi-square test and Fisher's exact test. SPSS software (version 22.0 for Windows, SPSS Inc., Chicago, IL, USA) was used for the statistical analysis. A p value less than 0.05 was considered statistically significant.
This study was approved by the Institutional Review Board of Yonsei University Severance Hospital. The board exempted written informed consent from all study participants.
RESULTS
Incidence of noninfectious complications of PD
The mean duration of PD therapy was 28.7±42.1 months (range 1-240 months). The common causes that led to ESRD were glomerular diseases (43.3%), followed by congenital anomalies of kidney and urinary tract (CAKUT) (20%) (Table 1).
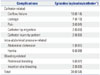
We divided the PD patients into those with and without mechanical complications, and there were no statistically significant differences between the groups in gender, age at PD start, and total duration of PD (Table 2). Thirty-eight episodes of mechanical complications, not including metabolic complications, occurred in 26 individuals (16 boys, 10 girls). The incidences of complications per catheter were as follows: outflow failure (14.3%), leakage (10.0%), hernia (8.6%), peritoneal bleeding (7.1%), inflow or outflow pain (4.3%), catheter tip migration (2.9%), catheter injury by patient or care-giver (2.9%), and abdominal distension (1.4%) (Table 3).
We also divided the patients into 0-5-years and ≥6-years age groups (Table 4). Despite a relatively small number of patients, leakage was significantly more frequent in the 0-5-years age group than in the ≥6-years age group (Table 4).
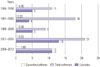
After dividing the data into 5-year intervals, the incidence (episodes/catheter) of noninfectious complications of PD was highest during the years 2006-2012 (p=0.001) (Fig. 1). The high incidence of years 2006-2012 was thought to be attributable to the higher proportion of young patients, as young age was an important risk factor for noninfectious complications of PD. The numbers of catheters used for 0-5-year-old patients were one (9.1%) in years 1986-1990, zero (0%) in years 1990-1995, five (55.6%) in years 1996-2000, seven (33.3%) in years 2001-2006, and seven (64.6%) in years 2006-2012.
Metabolic complications, including hyperglycemia, hypernatremia or hyponatremia, hyperkalemia or hypokalemia, and hypercalcemia or hypocalcemia within 1 month from starting PD, were observed in three (18.8%) of 16 patients: two patients (12.5%) had hyperglycemia, and one patient had hypokalemia (6.3%). However, the two patients with hyperglycemia at PD commencement showed no hyperglycemia after 1 month. Hypernatremia was not observed during the first month, although one patient showed mild hypernatremia (146 mmol/L) at the second month of PD. One patient had hyponatremia before PD which persisted after PD, but no patient had newly developed hyponatremia. Only one patient developed hypokalemia, which is believed to be associated with potassium-free solution and high peritoneal permeability at the beginning of PD. The patients with such complications received conservative care or were merely observed.
Patient outcomes
Three patients on PD were switched to HD. In the first patient, CAPD was started, but the PD catheter function was not adequate. Ultimately, he was treated with HD until kidney transplantation. In the second case, the patient's cardiomegaly worsened, and the treatment was changed to HD. In the third case, the patient's treatment was changed to HD due to catheter malfunction.
Another five patients required catheter reinsertion. Two patients experienced catheter malfunction, one of whom also had catheter malposition. After reinsertion, the catheter function was restored in these patients. Two cases of catheter injury were caused by the patient or care-giver. In the fifth patient, the catheter was reinserted due to oozing at catheter-insertion site.
Comparison of noninfectious complications of PD in different countries
The previous studies for noninfectious complications of PD in different countries are summarized in Table 5.4678910 Catheter-related complications, such as catheter malfunction, leakage, and dislocation, were notable causes of technique failure. Although technique failure was not related to an increase in patient mortality, it resulted in an early switch to HD. A recent study in Iran showed a high rate (24.5%) of hernias in children with PD,6 while our study showed a relatively lower rate (8.7%), suggesting that hernias can also frequently occur in children with PD.
DISCUSSION
The main goal of this study was to investigate noninfectious complications of PD at Severance Hospital in Korea. Our study revealed that noninfectious complications were relatively common in children on PD. Noninfectious complications of PD can largely be divided into mechanical and metabolic complications. Mechanical complications include flow obstruction, leakage, catheter disposition, and hernia. Common metabolic complications are hyperglycemia, hypertriglyceridemia, and hyperinsulinemia. Recent studies have reported varying incidences of these complications.678910 Although mechanical complications are mainly caused by catheter-related problems and increased intra-abdominal pressure, appropriate catheter selection, adequate surgical technique, and proper postoperative care can prevent early catheter malfunction.211 Additionally, close collaboration between nephrologists, surgeons, and radiologists will improve catheter function.
The most common mechanical complication in our center was outflow failure (14.3%). Some case series reported from different countries delineated the rate of outflow obstruction between 4.8% and 24.5%.68 Outflow failure, the incomplete drainage of instilled dialysate, can be caused by constipation, catheter migration, intraluminal or extraluminal catheter occlusion, and catheter kinking.21213 However, there are few data on the effect of catheter design and placement technique on long-term catheter survival and function.1415 In our study, 10 patients had a variable degree of catheter malfunction; however, only one patient required a change to HD, and two patients needed catheter reinsertion. Seven of these patients experienced restored catheter performance through conservative therapy, such as catheter irrigation, abdominal massage, and position change.
Pericatheter leaks are frequently observed within 30 days of catheter insertion. The spectrum of dialysate leaks includes any dialysate loss from the peritoneal cavity, ranging from pericatheter leakage to subcutaneous swelling and edema. A study by Hooman, et al.6 from Iran reported leakage rates as high as 17.6%, whereas the rate from an Italian group was 5.2%.8 Our study exhibited seven episodes (10.0%) of leakage, which was determined to be the second most common noninfectious complication of PD. One patient had a subcutaneous leak and required PD catheter reinsertion due to a hydrocele. However, the remaining six patients with pericatheter leaks were treated with compression and by decreasing the dialysate volume.
Various study groups reported great variation in hernia rates (between 0% and 24.5%).67 Although there were one episode of ventral hernia and 5 episodes of inguinal hernia, two of whom developed twice. All of these patients underwent herniorrhaphy.
Bloody PD effluent is called hemoperitoneum, and it has a good prognosis.211 We had five episodes of hemoperitoneum, and all of the patients recovered within several days. Heparin-mixed dialysate flushing was performed in all cases. Infusing cool dialysate may also be helpful.
Migration of the catheter tip could be the cause of poor drainage or inflow and pain during infusion or drainage. In our study, two patients had catheter tip migration, which lead to catheter malfunction. Kim, et al.10 suggested that laparoscopic PD catheter insertion would be better than classic open surgery, as laparoscopic surgery could fixate the catheter tip in the peritoneal cavity. Advanced laparoscopic technique facilitates rectus sheath tunneling and omentopexy and allows the catheter to be placed in the proper position under direct vision for lysis of adhesions.161718 Thus, laparoscopic catheter insertion could be a good choice.
Disequilibrium syndrome is a well-known complication of HD, but it is rare in patients on PD. However, one patient in our study experienced disequilibrium syndrome. Decreasing the volume of dialysate and widening the interval of dialysate exchange was beneficial in this case. Hyperglycemia and lipid metabolism abnormality are common complications of traditional PD solutions and may persist or deteriorate during renal replacement therapy.1920 The incidence of metabolic abnormalities associated with PD was not high in our small number of patients, but long-term serial evaluation may be necessary in a large number of cohort. Glucose-sparing solutions such as icodextrin could be an option for avoiding the metabolic effects of glucose and its byproducts.21
Although Rinaldi, et al.8 reported that there was no difference in catheter survival between younger children (<2 years) and other age groups of PD patients, age may be an important factor for the outcome of PD. Hooman, et al.6 showed that young age (<24 months) was the only independent factor that predicted mortality of PD patients. In our study, young children (≤5 years) had more noninfectious complications than older children. Young children had a higher risk of injury than older children in catheter-related damage due to increased mucosal fragility and soft-tissue lesions. More important concerns are higher levels of physical activity and irritability after catheter insertion.
In conclusion, PD is the preferred dialysis modality for children requiring renal replacement therapy due to less interruption of daily life and growth. Recently, treatment of peritonitis has been very successful, and noninfectious complications of PD have become relatively more important. The results of our study demonstrated that PD can be performed safely without severe complications, and noninfectious complications of PD rarely lead to catheter removal or HD in pediatric patients. The frequency of noninfectious complications of PD in our study was comparable with those of other pediatric studies.347891022 A reduction in noninfectious complications of PD can be achieved by optimal practices.23 Further randomized prospective studies are necessary to determine a universal recommendation as to the insertion method of PD catheters and glucose-sparing strategies.




 XML Download
XML Download