

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
It is not difficult to choose an effective antibiotic for treating community-onset acute pyelonephritis (APN); however, it may not be easy to choose an economical antibiotic with the least amount of ecological adverse effects for the treatment of APN. In addition, there is usually an opportunity to choose and tailor the antimicrobial regimen on the basis of susceptibility results, as uropathogens are commonly isolated in most cases of community-onset APN. Therefore, APN is a disease entity that is very useful for analyzing and elucidating the basic principles underlying the choice of antimicrobial agents.
Cefuroxime, a second-generation cephalosporin, is known to be an effective antibiotic against Enterobacteriaceae species and has been used for the treatment of APN.1234 However, extended-spectrum cephalosporins have been more commonly used for treating APN since the introduction of third-generation cephalosporin in the mid-1980s.56 However, extended-spectrum cephalosporins should be used judiciously due to the selection and spread of extended-spectrum β-lactamase (ESBL)-producing Enterobacteriaceae.7
It is recommended that women with APN who require hospitalization should be treated with an intravenous extended-spectrum cephalosporin, a fluoroquinolone, or an aminoglycoside, with or without ampicillin.6 We believe that cefuroxime may be a suitable alternative to cefotaxime for treating community-onset uncomplicated APN. Few clinical studies, however, have actually compared the efficacy of cefuroxime and cefotaxime in treating community-onset APN. In an attempt to reduce the use of extended-spectrum cephalosporins and prevent the selection and spread of multi-drug-resistant pathogens, such as ESBL-producing Enterobacteriaceae in the Republic of Korea (ROK), where the prevalence of fluoroquinolone resistance is high, we searched for additional options for initial empirical antibiotics that could be used in the treatment of APN in the ROK.
The study therefore compared the therapeutic efficacy of intravenous cefuroxime (750 mg, three times a day) with that of cefotaxime (2000 mg, three times a day), followed by optional oral therapy, in treating women with uncomplicated APN in the ROK.
MATERIALS AND METHODS
Study design
This was a retrospective study of women with community-onset uncomplicated APN due to Escherichia coli (E. coli). It was performed at St. Vincent's Hospital, a university-affiliated hospital in South Korea, from January 2011 to June 2014. All of the study protocols were assessed and sanctioned by the Institutional Review Board (IRB) of Catholic University St. Vincent's Hospital (approval number VC14OISI0152). The requirement for written, informed consent was waived by the IRB.
Patients and setting
The data of hospitalized women of ages ≥18 years old with community-onset APN due to E. coli who received intravenous antibiotic therapy were collected for the study. We retrospectively analyzed clinical symptoms, chronic medical conditions, uropathogens, laboratory values, and treatment regimens of patients with APN indicated in the hospital discharge database between January 2011 and June 2014. APN was defined clinically as a fever of ≥38.0℃ and the presence of at least three of the following conditions: pain in the flanks; costovertebral angle tenderness; symptoms of lower urinary tract infection (UTI) (pain during urination, urgency, increased frequency of urination, pelvic pain); pyuria on urinalysis [≥5-9 white blood cells (WBC)/high-power field]; and leukocytosis (peripheral blood leukocyte count greater than 11600/mm3 or polymorphonuclear cells plus bands greater than 65%).8910 Patients diagnosed with APN after the first 48 hours of hospitalization or patients with a catheter-associated UTI, a complicated case of APN, or azotemia were excluded from this study. We defined complicated APN as APN combined with any of the following comorbid conditions (cerebrovascular disorder, chronic liver disease, chronic renal disease, congestive heart failure, connective tissue disorder, diabetes mellitus, kidney transplantation, malignancy, pregnancy, or immunosuppression) or urinary tract abnormality (neurogenic bladder, polycystic kidney disease, urolithiasis, or vesicoureteral reflux) or APN in women more than 65 years old.8911 Ultimately, only the urine culture-confirmed cases of community-onset uncomplicated APN due to E. coli in women of ages ≥18 years initially treated with parenteral cefuroxime or cefotaxime were enrolled and analyzed.
According to the Catholic University St. Vincent's Hospital Antibiotic Policies, cefuroxime (750 mg, three times a day) or cefotaxime (2000 mg, three times a day) was usually administered intravenously in women with APN before they were switched to oral antimicrobial agents. Ciprofloxacin was preferentially used as an oral antimicrobial agent (500 mg, twice a day). However, oral cephalosporin or amoxicillin/clavulanate was used if the uropathogen was resistant to ciprofloxacin or if the patient could not tolerate ciprofloxacin. The suggested total duration of parenteral plus oral administration of the antimicrobial agent was 14 days.
Data collection
We collected and analyzed demographic characteristics, previous history of hospitalization and antibiotics usage, past history, underlying medical conditions, clinical symptoms, physical signs, laboratory findings, the length of parenteral and oral antibiotic therapy, microbiology results, hours to defervescence, length of hospitalization, and mortality by reviewing the health records for all participants. Clinical manifestations, physical findings, and laboratory results, were gathered and analyzed at admission, after 72 hours of antimicrobial treatment, at the 4-14-day follow-up, and at the 21-35-day follow-up visit after the end of therapy (EOT).
Clinical outcome assessments
We defined early clinical success as defervescence with mitigation of UTI signs or symptoms within the period of 72 hours following the initiation of antimicrobial treatment. Cases that did not fulfill the requirements of early clinical success were considered as early clinical failures.1213 Microbiological success or cure was defined as negative urine culture at the 3-4-day follow-up after the start of initial antibiotics or at the 4-14-day follow-up after the EOT. Clinical cure was defined as defervescence and complete resolution of UTI symptoms or signs at the 4-14-day or the 21-35-day follow-up after the EOT. Clinical failure at the 4-14-day follow-up was defined as the continuation or recurrence of UTI signs and symptoms within 4-14 days of follow-up after the EOT.1415
Treatment outcomes were estimated in terms of time to defervescence after the administration of initial antibiotics, hospitalization days, clinical and microbiological outcomes (cure or failure) at the follow-up visit.
Defervescence or resolution of fever was defined as the afebrile state of body temperature ≤37.0℃ and its continuation for at least 24 hours.8 Time to defervescence was defined as the time from the initiation of cefuroxime or cefotaxime therapy to an afebrile state. The body temperatures of each patient were measured by a tympanic thermometer every 4 hours during the hospitalization period.
Microbiological testing and outcomes
Quantitative urine culture and blood culture were performed at admission. All uropathogens were tested for in vitro susceptibility. Urine specimens and blood samples from women with APN were incubated. Etiological pathogens were determined by identifying ≥105 colony forming unit (CFU)/mL organisms on urine cultures or by isolating urinary pathogens from blood cultures.1016 Uropathogens and their antimicrobial susceptibility were identified by using a semiautomated system (VITEK, bioMerieux, Hazelwood, MO, USA).1718
Statistical methods
The results of this study are described in the form of means ±standard deviations (SD) or medians [interquartile ranges (IQR)], or numbers (percentages). Continuous variables are indicated as means±SD or medians (IQR) and were analyzed by the independent t-test or Mann-Whitney U test. Categorical variables were analyzed and compared using Fisher's exact test or the Pearson chi-square test. Tests with a probability of less than 0.05 were considered as indicating statistical significance. SPSS version 21.0 for Windows (SPSS Inc., Chicago, IL, USA) was used for statistical analyses.
RESULTS
Baseline clinical characteristics of the study population
Nine hundred and twelve women with community-onset APN were screened during the study period. Of these, 255 patients with community-onset uncomplicated APN due to E. coli who received cefuroxime or cefotaxime as the empirical antibiotic therapy were recruited (Fig. 1). Of these patients, 144 (56.5%) received cefuroxime and 111 (43.5%) received cefotaxime. Table 1 is a comparative chart of the baseline clinical characteristics, and treatment durations for the populations of the cefotaxime and cefuroxime groups. The median ages of the cefuroxime and cefotaxime groups were 41 (IQR, 31-51) years and 41 (IQR, 26-52) years, respectively (p=0.605) (Table 1). The patients in the two groups showed no significant differences in initial body temperature, costovertebral angle tenderness, flank pain, lower UTI symptoms, or the proportion of postmenopausal women. There were also no significant differences in previous history of UTI, prior history of hospitalization, or frequency of antibiotic usage within 12 months before the hospitalization between the cefotaxime and cefuroxime groups (Table 1).
In the laboratory findings, no statistically significant differences in leukocyte counts, C-reactive protein (CRP) level, and the proportions of hematuria and bacteremia were observed between the two groups. In addition, the prevalence of cefazolin-resistant E. coli and ESBL-positive E. coli were also not significantly different between the cefotaxime and cefuroxime groups (Table 1).
Microbiological data
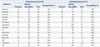
The antimicrobial susceptibility profiles of the 255 E. coli isolates are shown in Table 2. The susceptibilities of E. coli to amikacin, amoxicillin/clavulanate, ampicillin, cefazolin, cefepime, cefotaxime, cefoxitin, ceftazidime, fluoroquinolone, gentamicin, piperacillin/tazobactam, and trimethoprim/sulfamethoxazole were compared using Fisher's exact test or the Pearson chi-square test and were not significantly different between the cefuroxime and cefotaxime groups.
In the cefuroxime and cefotaxime groups, the susceptibilities of E. coli were 82.6% versus 83.8% to cefazolin and 93.1% versus 91.0% to cefotaxime, respectively. In addition, there was no statistical significance of the proportion of ESBL-producing E. coli between the two groups.
Comparative analysis of the clinical outcomes in the cefuroxime and cefotaxime groups
Clinical outcomes were compared between the cefotaxime and cefuroxime groups (Table 3). A cefuroxime dose of 2250 mg/day was administered intravenously three times a day in the cefuroxime group. The dose of cefotaxime was 6000 mg/day, and it was administered intravenously three times a day in the cefotaxime group. The durations of the cefuroxime and cefotaxime therapies were 5 (IQR, 4-6) days and 5 (IQR, 4-6) days, respectively (p=0.516). The durations of total antimicrobial therapy were 14 (IQR, 14-14) days in the cefuroxime group and 14 (IQR, 14-14) days in the cefotaxime group (p=0.306). Of all 255 enrolled patients, 238 (93.3%) and 137 (53.7%) had a follow-up at 4-14 days and at 21-35 days, respectively, after the EOT.
Six (4.2%) of 144 patients in the cefuroxime group and six (5.4%) of 111 patients in the cefotaxime group were converted to an alternative intravenous therapy. The clinical success rates were 13.9% (20 of 144) versus 12.6% (14 of 111) at 24 hours, 52.8% (76 of 144) versus 54.1% (60 of 111) at 48 hours, 88.2% (127 of 144) versus 90.1% (100 of 111) at 72 hours, 93.1% (134 of 144) versus 97.3% (108 of 111) at 96 hours, and 97.9% (141 of 144) versus 100% (111 of 111) at 120 hours in the cefuroxime and cefotaxime groups, respectively, and these differences were not statistically significant between the two groups (Table 3). The median times to defervescence were 46 (IQR, 32-67) hours and 45 (IQR, 30-61) hours in the cefuroxime and cefotaxime groups, respectively (p=0.482). The median durations of hospital stay in the cefuroxime and cefotaxime groups were 7 (IQR, 6-8) days and 7 (IQR, 6-8) days, respectively (p=0.157).
The clinical cure rates at 4-14 days after the EOT were 94.9% (129 of 136) and 98.0% (100 of 102) in the cefuroxime and cefotaxime groups, respectively (p=0.307). No complications associated with APN, such as renal failure, renal abscess or septic shock, occurred in either the cefuroxime or cefotaxime group. The clinical cure rates at 21-35 days after the EOT were 97.4% (75 of 77) and 100% (60 of 60) in the cefuroxime and cefotaxime groups, respectively (p=0.504).
Microbiological outcomes were available for 183 of 255 women at the 4-14-day follow-up and for 57 of 255 women at the 21-35-day follow-up after the EOT. Microbiological cure rates were 88.3% (91 of 103) versus 95.0% (76 of 80) at 4-14 days after the EOT and 85.2% (23 of 27) versus 96.7% (29 of 30) at 21-35 days in the cefuroxime and cefotaxime groups (p=0.186 and p=0.179), respectively.
Of 255 women, 20 had APN due to ESBL-positive E. coli, and 235 had APN due to ESBL-negative E. coli. The time to defervescence was not statistically different between the ESBL-positive and ESBL-negative groups [38.0 (IQR, 27.3-69.8) hours versus 46.0 (IQR, 32.0-65.0) hours, respectively; p=0.714]. Therefore, the early clinical success rates at 72 hours in the ESBL-positive and ESBL-negative groups were 85.0% (17 of 20) versus 89.4% (210 of 235), respectively, which was not significantly different (p=0.469). However, the cure rates at 4-14 days after the EOT in the ESBL-positive group were significantly lower (clinical: 75.0% versus 98.2%, p<0.001; microbiological: 63.2% versus 94.5%, p<0.001) than those in the ESBL-negative group.
Comparison of laboratory findings and microbiological outcomes after 72-96 hours of cefuroxime or cefotaxime treatment
The median CRP levels after 72-96 hours of antimicrobial therapy were 4.21 (IQR, 2.27-6.78) mg/dL and 3.54 (IQR, 1.92-5.72) mg/dL, respectively, in the cefuroxime and cefotaxime groups and were not significantly different (p=0.135). The median WBC counts after 72-96 hours of antimicrobial therapy were 5390 (IQR, 4290-6368) and 5060 (IQR, 4210-6130), respectively, in the cefuroxime and cefotaxime groups (p=0.344) (Table 4).
Microbiological outcomes were available for 221 of 255 women after 72-96 hours of antimicrobial therapy. Microbiological success rates after 72-96 hours of cefuroxime or cefotaxime therapy were 89.4% (110 of 123) versus 94.9% (93 of 98) in the cefuroxime and cefotaxime groups, respectively (p=0.140) (Table 4).
DISCUSSION
Antibiotic resistance is a major clinical and public health problem that must be managed. The use of narrow-spectrum antibiotics in the treatment of infectious diseases is one of many methods that can be used in the battle against infectious diseases.19202122 Although the use of narrow-spectrum antibiotics is one of most important principles in the choice of antimicrobial agents and appreciated by most physicians, broad-spectrum antibiotics can be recommended in guidelines due to lack of clinical evidence or for the concerns about patient safety. Cefotaxime has been recommended as an empirical antibiotic for the treatment of community-onset APN in women according to therapeutic effects in many clinical studies.6 However, cefuroxime is not recommended for similar use in the treatment guidelines for APN, as there is a lack of clinical trials and studies concerning the use of cefuroxime for the treatment of APN. Few clinical trials have demonstrated that cefuroxime is inferior or superior to extended-spectrum cephalosporins.
In this study, the clinical cure rate, microbiological cure rate, mortality rate, hospitalization period, and duration of total antimicrobial therapy were not significantly different between the cefuroxime and cefotaxime groups. In this study, we excluded patients with complicated APN and compared cefotaxime with cefuroxime, which are relatively old antibiotics, rather than the newly-developed carbapenem or β-lactam/β-lactamase inhibitor. These results in our study offer support for reviving an old antibiotic, cefuroxime, which can be used effectively in the treatment of uncomplicated APN.
Resistant uropathogens are known to be associated with treatment failure in APN; however, in several studies, discordant use of initial empirical antibiotics was not found to be a factor related to clinical failure in patients with APN, as this therapy was followed by the use of other antimicrobial agents in sequence after obtaining uropathogen susceptibility test results.131720 Although the prevalence of uropathogen resistance to cefuroxime or cefotaxime might influence the clinical outcomes, the susceptibilities of E. coli in the cefuroxime and cefotaxime groups were 93.1% versus 91.0% to cefotaxime and 82.6% versus 83.8% to cefazolin, respectively (Table 2). In this study, susceptibility testing of uropathogens to cefuroxime was not performed, as a susceptibility test to cefuroxime was not available in our microbiological evaluation system. However, susceptibility of uropathogens to cefuroxime in the cefuroxime group were presumed to be between 82.6% (susceptibility to cefazolin) and 93.1% (susceptibility to cefotaxime). One of our purposes in this study was to emphasize that the susceptibility test to cefuroxime should certainly be available in routine microbiological evaluation systems.
In this study, we also compared the early microbiological outcomes and laboratory findings after the initial 3-4 days of cefotaxime or cefuroxime therapy for the purpose of excluding the effects of other alternative or oral antibiotics. Thus, we found that the early microbiological success rates after the initial 72-96 hours of cefotaxime or cefuroxime therapy in the two groups indicated no significant difference.
These results suggest that intravenous cefuroxime, as well as cefotaxime, can be used as the initial empirical antimicrobial agent in hospitalized women with uncomplicated APN, provided that there is a later change to other antimicrobial regimens concordant with microbiological susceptibility data.
This study had several limitations. First, it was not a randomized, controlled trial but a retrospective study. Therefore, we investigated clinical and microbiological data within a group of women with uncomplicated APN who received only intravenous cefotaxime or cefuroxime as an initial empirical antimicrobial agent. In addition, we planned to compare the cefotaxime and cefuroxime groups after adjusting for propensity score. However, the baseline demographics, clinical characteristics, and laboratory findings of the cefotaxime and cefuroxime groups indicated no significant differences. These similarities between the two groups are presumed to be caused by excluding women with complicated APN or other underlying disorders. Second, the microbiological cure rate might not have been accurately determined, as the microbiological data were available in only 183 of the 255 enrolled patients at the follow-up visit.
In conclusion, intravenous cefuroxime, a second-generation cephalosporin, is a viable alternative for treating community-onset APN in this era of increasing antimicrobial resistance, especially in the regions that need to reduce third-generation cephalosporin use or where the prevalence of uropathogens with ESBL is low. The use of cefuroxime may contribute to broad-spectrum cephalosporin-sparing in the treatment of APN. Adequately powered and well designed comparative trials comparing the efficacy of cefuroxime and cefotaxime are required for the treatment of uncomplicated APN.




 XML Download
XML Download