

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Atrial fibrillation (AF) is the most common arrhythmia in clinical practice and causes significant morbidity and mortality.1 Although the use of radiofrequency catheter ablation (RFCA) is increasing around the world,2 analysis of pre-procedural characteristics that stratify for procedural efficacy and safety might be helpful, given the cost and potential complication of this procedure.3 Recent studies have demonstrated that early recurrence of AF (ERAF) after catheter ablation might be associated with a worse rhythm outcome during long-term follow-up, although the proportion of clinical recurrence of AF three months after RFCA varies gradually.4 The pathophysiology of ERAF remains unclear; however, pro-inflammatory effects after catheter ablation may play an important role in ERAF.5 Nitric oxide (NO) is one of many essential factors suppressing arrhythmia through a cGMP-mediated modulation of cardiac autonomic nerve activity or atrial electrical remodeling.6 Several studies suggest that NO levels and bioavailability are markedly reduced in the atria during AF.67 One clinically relevant eNOS variant is the missense G894T variant (rs1799983) in exon 7. This mutation corresponds to a GluAsp substitution (Glu298Asp).8 The rs1799983 variant has been reported to be associated with reduced basal NO production9 and ischemic stroke.10 Some of eNOS3 gene polymorphisms were reported to be associated with predisposition to AF,1112 but other single nucleotide polymorphisms (SNPs) of the same gene were not. So, there still remains some controversy regarding this finding.13 The present study explored the relationship between eNOS3 SNPs and the recurrence of AF after catheter ablation.
MATERIALS AND METHODS
Study population
The study protocol was approved by the Institutional Review Board of the Yonsei University Health System and all patients provided written informed consent. Participants included 500 consecutive Korean patients with AF who underwent RFCA and 500 age, gender-matched healthy control provided by National Biobank of Korea (KOBB-2012-00).14 Exclusion criteria were as follows: 1) permanent AF refractory to electrical cardioversion; 2) left atrial (LA) size >55 mm as measured by echocardiogram; 3) AF with valvular disease >grade 2; 4) any structural heart disease other than left ventricular hypertrophy; 5) residual coronary artery stenosis >75%; and 6) prior AF ablation or maze surgery. Three-dimensional (3D) spiral computerized tomography (CT) scans (64 Channel, Light Speed Volume CT, Philips Brilliance 63, Eindhoven, the Netherlands) were performed to visually define the pulmonary vein (PV) anatomy. Using trans-esophageal echocardiography, we ensured that no LA thrombus was present. All antiarrhythmic drugs were discontinued for at least five half-lives of the respective drugs. Amiodarone was discontinued at least four weeks prior to the procedure. Anticoagulation therapy was performed before catheter ablation.
Electrophysiologic mapping and radiofrequency (RF) catheter ablation
Intracardiac electrograms were recorded using the Prucka CardioLab™ electrophysiology system (General Electric Health Care System Inc., Milwaukee, WI, USA), and catheter ablation was performed in all patients using 3D electroanatomical mapping (St. Jude Medical Inc., Minnetonka, MN, USA) merged with 3D spiral CT. If the initial recording identified a sinus rhythm, an LA 3D electroanatomical voltage map was generated during atrial pacing by obtaining contact bipolar electrograms from 350-400 points on the LA endocardium. Color-coded voltage maps were generated by recording bipolar electrograms and measuring peak-to-peak voltage during high right atrial pacing with a cycle length of 500 ms as previously described.151617 We used an open irrigated-tip catheter (Celsius, Johnson & Johnson Inc.; Diamond Bar, CA, USA; irrigation flow rate 20 to 30 mL/min; 30 W; 47℃) to deliver RF energy for ablation (Stockert generator, Biosense Webster Inc.; DiDiamond Bar, CA, USA). We generally performed RFCA in sinus rhythm after electrical cardioversion. However, if sinus rhythm could not be maintained due to immediate recurrence of AF, RFCA was performed while in AF. All patients initially underwent circumferential PV isolation and bi-directional block of the cavo-tricuspid isthmus. For patients with paroxysmal AF, additional linear ablation or complex fractionated atrial electrogram (CFAE) ablation guided by 3D-CFAE-CL map18 was conducted depending on the operator's decision. In patients with persistent AF, circumferential PV isolation, cavo-tricuspid isthmus block, and roof line, posterior inferior line, and anterior line19 were performed as a standard lesion set. If AF persisted, CFAE ablation was done depending on the operator's decision. Most of procedures were conducted during sinus rhythm after cardioversion to generate voltage map. However, if AF persisted despite administration of the aforementioned ablation protocols, procedures were stopped after internal cardioversion. Procedural end-point was defined when there was no immediate recurrence of AF after cardioversion by isoproterenol infusion (5-20 µg/min). If non-PV foci were identified in 10.9% under isoproterenol, they were all ablated.
Post-ablation follow-up
All patients were followed in the absence of anti-arrhythmic medications after RFCA. Patients were asked to visit an outpatient clinic at 1, 3, 6, and 12 months after RFCA and then every 6 months thereafter for follow-up. Electrocardiography (ECG) was performed at each visit and whenever the patient reported palpitations. A Holter ECG (24- or 48-hour) and/or event recorder was performed on patient at every six-month follow-up and whenever the patient complained of symptoms for at least two years according to 2012 ACC/AHA/ESC expert consensus guideline for AF management.20 We defined recurrence of AF as any episode of AF or atrial tachycardia of at least 30 sec in duration.21 We did not use routine anti-inflammatory drug after procedure. If the patient complained symptomatic arrhythmia within 3rd month of procedure, we tried to document it by Holter ECG or event recorder depending on the frequency and duration of symptom. If AF was found on ECG within the three-month blanking period during follow-up, the patient was diagnosed with ERAF, and any AF recurrence thereafter was diagnosed as clinical recurrence.21 For the patients with symptomatic ERAF, we prescribed anti-arrhythmic drug. However, we stopped antiarrhythmic drug in these patients, if there was no AF in 3rd month Holter ECG.
Off-line analyses of color-coded 3D maps and CT images
We analyzed color-coded voltage maps of both anterior-posterior and posterior-anterior views. Percent of each color area was calculated by customized software (Image Pro) and referenced with color scale bars. PVs were not included in the analysis. Low voltage areas, defined as LA voltage <0.2 mV, were colored gray, and high voltage areas (>5.0 mV) were colored purple.
Biochemical analyses
Plasma levels of high sensitivity C-reactive protein (hsCRP) was quantified with a commercially available enzyme-linked immunosorbent assay (R&D Systems, Minneapolis, MN, USA) method in peripheral blood samples taken just before the procedure.
Genotyping of rs1799983 in whole blood
eNOS is an enzyme that catalyzes the formation of NO from Larginine. Several polymorphisms have been described. rs1799983 G894T is evaluated in the present study.22 Genotyping of rs1799983 was performed using a validated TaqMan assay (Applied Biosystems, Life Technologies, Carlsbad, CA, USA). Polymerase chain reaction (PCR) was performed using 0.9 µm of forward and reverse primers, 0.2 µm of fluorescein amidite and VIC minor groove binding sequence-specific probes. PCR constituents were as follows: 3 ng of DNA, 5.0 mM MgCl2, and 1x TaqMan Universal PCR Master Mix containing AmpliTaq Gold DNA polymerase in a 5.5-µL reaction volume. Both the SNPs had a call rate of >99%.
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Sciences software for Windows version 18.0 (SPSS Inc., Chicago, IL, USA). A chi-square test was used to test the deviation of genotype distribution from Hardy-Weinberg equilibrium. Genotype distribution and allelic frequencies in patients with and without AF recurrence were compared using a chi-square test. The strength of the association between gene trait and ERAF was determined by calculating an odds ratio and 95% confidence interval. p<0.05 was considered significant.
RESULTS
Frequency of rs1799983 variant allele in patients with AF vs. controls
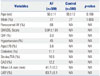
The baseline characteristics of study population are shown in Table 1. Participants included 500 consecutive Korean patients with AF (77% males, 56±11 years old) who underwent RFCA and 500 age, gender-matched healthy control without ECG documented AF, provided by National Biobank of Korea (KOBB-2012-00). Among the AF patients, 68% had paroxysmal and 32% had persistent AF. A mean of 1.9±1.3 antiarrhythmic drugs had been used to treat the AF patients prior to RFCA. Table 2 shows the genotype distribution and allele frequencies of the eNOS polymorphisms. Variant frequency did not deviate significantly from Hardy-Weinberg equilibrium. There were no significant differences in the genotype and alallele frequencies between the patient and control group.
Characteristics of eNOS3 gene (rs1799983) variants and AF recurrence
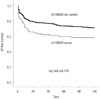
Table 3 summarizes the differences between AF patients with rs1799983 variants and those without variants. There were no significant differences in general clinical features and the degree of LA electro-anatomical remodeling between patients with and without the rs1799983 variant (T). In addition, serum hsCRP levels were not significantly higher in patients with the rs1799983 variant. Interestingly, the frequency of associated stroke/transient ischemic attack and coronary artery disease was significantly higher in patients with the rs1799983 variant (p=0.004). Statin utilization was also significantly higher in patients with the rs1799983 variant (p=0.010). ERAF (within 3 months post-RFCA) was observed in 31.8%, whereas clinical recurrence of AF (after 3 months post-RFCA) occurred in 24.8% of the patients during mean follow-up of 17±8 months. The clinical recurrence rate after 3 month post-RFCA was not different in patients with rs1799983 variant and in those without (p=0.907). However, ERAF was more frequent in patients with the variant allele of the rs1799983 than in those without (42.2% vs. 29.8%, p=0.027). In addition, ERAF occurred significantly earlier in the carriers of the variant allele (mean early recurrence days, 11±16 days vs. 20±25 days, p=0.016) (Fig. 1).
In the sub-analysis for Persistent AF, early and clinical recurrence rates were 59.3% and 26.9% in the rs1799983 variants, and 40.0% and 45.1% in non-variant group, respectively. However, early (p=0.066) and clinical recurrence rates (p=0.087) did not reach to the statistical difference. Among 124 patients with clinical recurrence, we tried anti-arrhythmic medication first. If recurred AF was not controlled by antiarrhythmic drug, we conducted redo-ablation in 46 patients (4.8% in rs1799983 variant group vs. 10.1% in non-variant group, p=0.084). Early recurrences were observed in 1 out of 4 patients in variant group and 14 out of 42 patients in non-variant group after redo-procedure. None of 4 patients in variant group and 15 out of 42 patients in non-variant group recurred after 3rd month of redo-ablation.
Characteristics and predictors of ERAF after RFCA
Table 4 compares characteristics of AF patients with and without early recurrence. Patients with early recurrence were more likely to have persistent AF (44.4% vs. 27.1%, p<0.001) and had larger left atria (p=0.011) compared to those without early recurrence. LA endocardial voltages were significantly lower in patients with early recurrence than in those without (p=0.025). Patients with early recurrence were more likely to be taking an angiotensin converting enzyme inhibitor or an angiotensin II receptor blocker than those without (p=0.020). In contrast, procedure time (p<0.001) and ablation time (p<0.001) were significantly longer in patients with early recurrence.
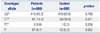
In a univariate analysis, persistent AF, larger LA size, and presence of the rs1799983 variant were associated with ERAF after RFCA. Multivariate analysis showed that the rs1799983 variant (OR 1.75, 95% CI 1.07-2.86, p=0.026) and persistent AF (OR 1.91, 95% CI 1.27-2.94, p=0.003) were independent predictors of ERAF (Table 5).
DISCUSSION
We found that the eNOS SNP rs1799983 is associated with ERAF after catheter ablation. Although the frequency of the rs1799983 risk allele (T) is similar among cases and controls, risk allele carriers were more likely to have coronary artery disease, stroke and ERAF within 3 month post-RFCA.
eNOS, cardiovascular disease/stroke, and AF
The eNOS gene SNPs, rs1799983 has been reported to be associated with hypertension23 and ischemic stroke.24 In addition, Park, et al.25 reported the association of the rs1799983 gene polymorphism with acute coronary syndrome in Korean patients. In the present study, patients with the rs1799983 variant were found to be more likely to have coronary artery disease or stroke which is consistent with previous studies.
AF has been associated with a marked decrease in NOS expression and NO bioavailability in the LA.7 These data indicate that laminar blood flow in sinus rhythm and the cyclic stretch of atrial endocardial cells may act as a stimulus for maintaining normal endocardial expression and function of NOS. It is likely that loss of this important antithrombotic enzyme contributes to the thromboembolic phenomena commonly observed in AF. The association of eNOS3 gene polymorphism, rs1799983, with AF has been investigated by several studies. Bedi, et al.11 reported that rs1799983 TT genotype was associated with AF in patients with congestive heart failure. In contrast, Fatini, et al.1112 and Gensini, et al.13 did not find relationship between rs1799983 polymorphism and AF, which is consistent with the current study. Although we did not find a difference in the frequency of the rs1799983 variant between the AF and control groups, carriers of the rs1799983 variant allele appeared to show a different clinical course after catheter ablation of AF due to decreased NO activity.
ERAF and rs1799983 variant
Although the mechanism of ERAF after RFCA remains unclear, there are potential explanations. First, post-RFCA inflammation is related to electrical instability. An acute inflammatory response is associated with extensive tissue damage involved in extensive AF catheter ablation, and the time course of the presumed resolution of this inflammation correlates well with spontaneous arrhythmia resolution.26 This inflammation is sufficient to facilitate the initiation of atrial arrhythmias.27 In this study, ERAF was higher in patients with the rs1799983 variant allele, and reduced NO availability in genetic variants may contribute to impaired resolution of inflammation after extensive RFCA. However, we did not find a relationship between rs1799983 variants and plasma levels of hsCRP in this study. This may be because plasma levels of hsCRP are influenced by multiple factors including the degree of electroanatomical remodeling of the atrium28 as well as persistence of AF.29
Alternative explanation for ERAF is the recovery of electrical conduction at the ablation sites. This mechanism may explain the fact that 40% of patients with ERAF extend to clinical recurrence of AF 3 months after RFCA. ERAF has been known to be an independent predictor for clinical recurrence after RFCA.4 Remaining 60% of patients with ERAF had no clinical recurrence after 3 months. Therefore, the mechanism of ERAF in patients with the rs1799983 variant allele is more likely to be an acute inflammatory response rather than the conduction recovery, because of an earlier timing of ERAF and no increase of clinical recurrence after 3 months with the rs1799983 variant allele. The eNOS3 gene variants may have a potential role for determination of post-ablation management such as anti-inflammatory drug (e.g., steroid)30 or prediction of clinical outcomes.
Study limitations
We analyzed the SNPs in the eNOS gene in a Korean population undergoing catheter ablation. Therefore, our findings cannot be generalized to all types of AF. When applying SNPs as predictors and targets of therapy for AF, possible racial differences in the association between SNPs and AF should be considered. Although replication study is needed to validate genetic role, we could not conduct it because of different ablation strategies of catheter ablation in the independent cohort.
Conclusion
This study shows that the eNOS3 gene variant, rs1799983, is associated with ERAF after catheter ablation, especially at an earlier stage within 3 months post-RFCA, but not associated with clinical recurrence. Even though we did not find any correlation between eNOS3 gene polymorphism and inflammatory marker, the mechanism of ERAF in patients with the rs1799983 variant allele might be associated with an acute inflammatory response, and the role of anti-inflammatory medication should be studied to prevent ERAF in eNOS3 gene variants at the immediate post-ablation period.



 XML Download
XML Download