

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
It is difficult to predict block height in pregnant women after combined spinal-epidural anesthesia (CSE) with a hyperbaric local anesthetic, as many factors influence block height.1234 When the block is performed in the lateral position, an inappropriately high sensory block frequently occurs, which is one cause of hemodynamic instability, and many studies have been conducted with the goal of preventing this side effect.567 One such study involved modified positioning (the Oxford position),5 in which the head and shoulder are supported and raised in a lateral position during the placement of spinal anesthesia; the flexure is raised at the level of the fourth thoracic vertebra, and the spread of local anesthesia in the subarachnoid space toward the cephalic region is prevented. However, a higher block can occur when the patient is changed to the supine position, due to further cephalad spread of the local anesthetic in the subarachnoid space.78910 We aimed to determine whether maintaining head elevation at the level of the fourth thoracic vertebra, even after changing to the supine wedged position for surgery, can prevent occurrence of inappropriate higher sensory block and improve hemodynamic stability. In this randomized controlled trial, we compared the prevalence of hypotension, amount of ephedrine given, and maximal sensory block height between the right lateral (group L) and right lateral and head elevated (group HE) group.
MATERIALS AND METHODS
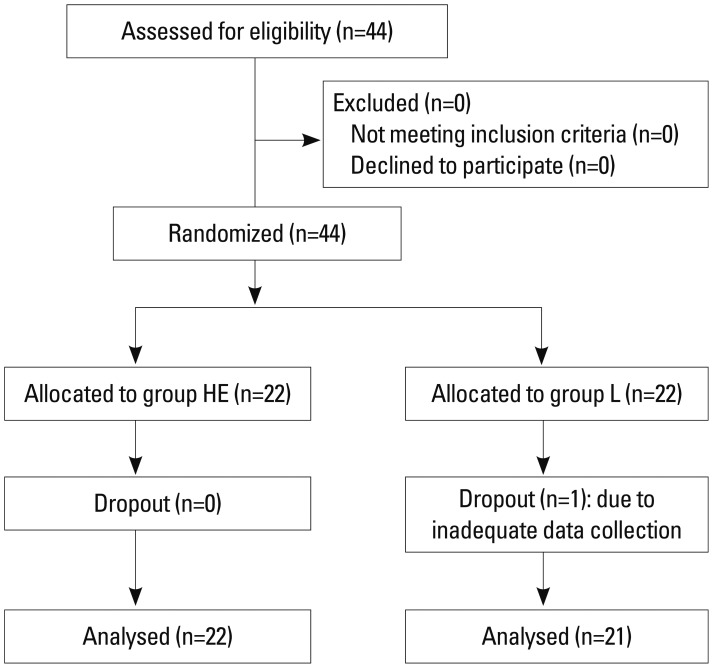
This study was approved by our Institutional Review Board (registered at http://cris.nih.go.kr; Ref: KCT0000583). Written informed consent was obtained from all subjects and data collection was carried out between March and September 2012. Forty-four parous women scheduled for elective Caesarean section under CSE were enrolled and randomly assigned by a computer-generated sequence to the right lateral (group L) or right lateral and head elevated (group HE) group. Women with contraindications to regional anesthesia, including coagulopathy, local skin infection, uncorrected hypovolemia, body weight <50 kg or >100 kg, intrauterine growth restriction, preeclampsia, or multiple gestation were excluded.
None of the patients received premedication. Standard monitoring devices including electrocardiogram, pulse oximeter, and noninvasive blood pressure cuff were applied on arrival in the operating room. Before undergoing CSE, all patients received 10 mL/kg of intravenous crystalloid solution over a period of 10 min. Baseline systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP), and heart rate (HR) were recorded.
Patients were placed on their right side for anesthesia. In group L, women were placed in the right lateral position with one pillow supporting the head. In group HE, women were placed in the right lateral position with three pillows supporting the head and two pillows under the shoulder. After positioning, SBP, DBP, MAP, and HR were recorded from the lower arm. CSE was performed in the midline at the L3-4 interspinous space. When free flow of cerebrospinal fluid (CSF) was confirmed, 10 mg of 0.5% hyperbaric bupivacaine (Marcaine®, Astra Zeneca, Sweden) and 10 ug of fentanyl were injected into the subarachnoid space over 30 s. An epidural catheter was then inserted 5 cm into the epidural space. Following CSE, patients in group L were repositioned supine with a wedge under the right hip. Group HE patients were turned 180° to the left lateral position, with three pillows continuing to support the head and two pillows under the shoulder. When the sensory block height reached T5, group HE subjects were placed in the supine position, maintaining two pillows under the shoulder and three pillows under the head, and a wedge under the right hip, until the end of surgery. In cases in either group when the block failed to reach the T5 segment within 20 min of the intrathecal injection, 6 mL of 2% lidocaine was administered through the epidural catheter. A second investigator who took no part in the CSE assessed the sensory block and hemodynamic values.
The endpoint of the study was reached when the sensory block fell below T10 in the recovery room, at which point patients were transported to their rooms. Sensory block level was assessed through testing loss of light touch with an alcohol swab.
For statistical analyses, each dermatome level was scored in sequence (L3=1 and T6=10). The intervention blood pressure level was calculated as 80% of the baseline blood pressure. If MAP fell below the intervention level or if SBP fell to 90 mm Hg, 4 mg of ephedrine was injected intravenously. If the blood pressure continued to drop, the same dose of ephedrine was injected repeatedly. Oxygen was supplied at a rate of 5 L/min via facemask during surgery.
We recorded SBP, DBP, MAP, HR, dosage of ephedrine, and sensory block height every 3 min before delivery and every 5 min after delivery. We also recorded time from spinal injection to T5 sensory block, incision, delivery, and completion of surgery. In addition, the maximal sensory block level (MSBL), the time at which MSBL was achieved, and the time to two-segment regression (TSR) of the sensory level were also recorded.
Statistical analysis was performed with SAS statistical software (version 9.2, SAS Inc., Cary, NC, USA). Data were expressed as mean±SD, median (range), or number of patients. Sample sizes were calculated assuming that the difference in the amount of ephedrine required to treat hypotension would be over 10 mg, with an alpha error of 0.05 and a power of 80%. A total of 18 patients per group was necessary to demonstrate statistical significance; therefore, we assigned 22 patients to each group to allow for possible protocol violations during the study period.
For comparison of variables between groups, the Kolmogorov-Smirnov test was used to identify variables with a normal distribution. Variables with a normal distribution were compared using the independent t-test, and those without a normal distribution were compared using the Mann-Whitney U test. The numbers of patients between groups were compared using the chi-squared or Fisher's exact tests. Value comparisons for each measurement were also conducted using repeated measures analysis of variance (ANOVA). All significant results were further analyzed with the Bon-ferroni post hoc test to determine whether the time points at which we recorded data produced values significantly different from baseline values. A p value of less than 0.05 was considered statistically significant.
RESULTS
Forty-four parous women were enrolled in this study; one was excluded due to inadequate data collection (Fig. 1). Demographic data are presented in Table 1 and did not differ significantly between the two groups.
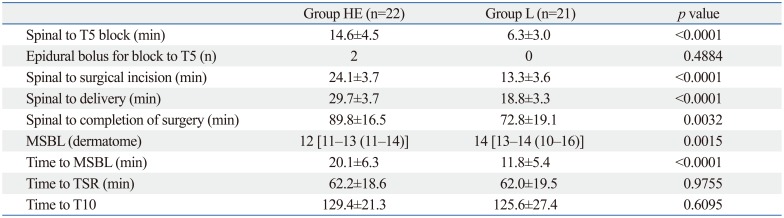
The characteristics of the sensory blocks are presented in Table 2. The lengths of time from spinal injection to T5 sensory block and achievement of MSBL were shorter in group L than in group HE. Correspondingly, the lengths of time from spinal injection to surgical incision, delivery, and completion of surgery were longer in group HE than in group L due to the longer interval required to reach T5 sensory block in group HE. MSBL was also higher in group L than in group HE [14 (T2) versus 12 (T4), p=0.0015]. However, the length of time to TSR of the sensory level and T10 did not significantly differ between the two groups.
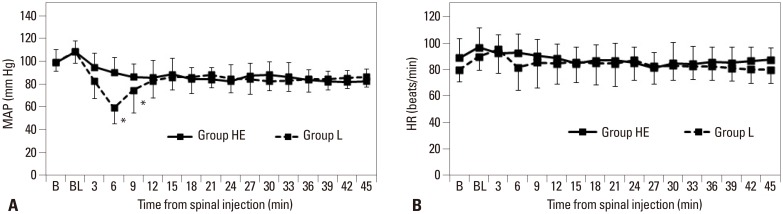
The incidence of hypotension was significantly higher in group L than group HE. The amount of ephedrine administered before and after achieving sensory block to T5 was also significantly higher in group L than in group HE (Table 3).
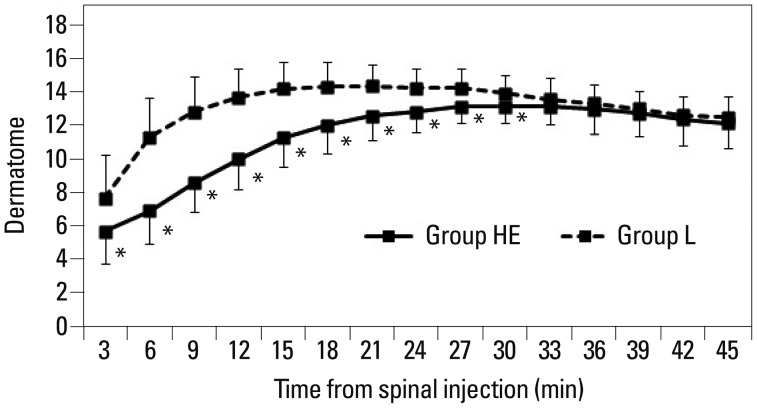
Fig. 2 shows the number of dermatomes blocked at each time point. The number of dermatomes blocked was greater in group L than in group HE during the 30 min following spinal injection.
DISCUSSION
We found that head elevation during CSE and surgery for Caesarean section resulted in appropriate MSBLs and a more gradual onset of anesthesia than that achieved with lateral to supine wedged positioning. In addition, maintaining head elevation resulted in a stable MAP after CSE, with a lower requirement for ephedrine.
In obstetrical anesthesia, neuraxial analgesia has to be considered as the gold standard in maternal pain relief during labour or Caesarean section. However, the side effects of neuraxial analgesia, including maternal hypotension or nausea, cannot be underestimated.11 Many studies have been conducted with the goal of preventing these side effects.56711
The spread of a local anesthetic within the CSF is influenced by positioning during and after intrathecal injection. When performing CSE using the lateral to supine wedged position, the curvature of the upper thoracic vertebrae may not be sufficient to prevent significant cephalad spread. In the Oxford position, the patient is placed in the lateral position with an inflation bag under the shoulder and three pillows supporting the head. Viewed from the lateral side, an upward slope is formed in the mid-thoracic region above T3-4. This position was designed to prevent the spread of local anesthetic above T3-4 and to minimize aortocaval compression. Previous studies comparing the Oxford position and other positions for Caesarean section have generated conflicting results in regard to block height and hemodynamic stability.789 Stoneham, et al.7 and Russell, et al.8 demonstrated that elevation of the thoracic vertebrae in the Oxford position slowed the onset of the sensory block and reduced the risk of a dangerously high block. In addition, a longer period of time in the Oxford position prevented anesthesia from ascending further cephalad. However, the majority of patients required ephedrine shortly after repositioning, when returning to the supine wedged position for surgery. In contrast to the findings of Stoneham, et al. and Russell, et al., Rucklidge, et al.9 reported that the Oxford position offered no advantage over sitting or lateral positioning for CSE. Nonetheless, there are several important differences between these reports and our study. First, in the report by Rucklidge, et al., the lateral group underwent CSE in the lateral position and maintained the contralateral position until just prior to operation. This approach differs from previous studies that examined the lateral to supine wedged position. In addition, different doses of spinal agents were administered, and, according to the study design, all groups received 6 mg of prophylactic ephedrine intravenously after intrathecal injection. It was also difficult to carry out an accurate comparison, as they did not measure the degree of block and MSBL according to time; the lateral group reached T5 sensory block and MSBL the fastest. After CSE, there was a reduction in blood pressure in the lateral group; the lack of a significant difference in blood pressure among the groups appears to be the result of appropriate ephedrine use. However, there was a trend toward reduced total ephedrine requirement in the sitting group compared with the lateral and Oxford groups. We consider the conflicting results described above to have resulted from the occurrence of a higher block when changing from the Oxford position to supine for surgery. Hence, in our study, we maintained head elevation during surgery after a T5 block was achieved from CSE performed in the Oxford position. Specifically, the Oxford position is a position for induction of spinal anesthesia or CSE, not for surgery.
Head elevation creates an upward slope in the thoracic region; this position was maintained until the end of surgery to prevent cephalad migration of anesthesia to the upper thoracic nerve roots. In our study, the maximal median segmental block height was T2 (T6-C8) in group L and T4 (T5-2) in group HE (p=0.0015). Relative to group L, group HE required a longer time to reach T5 sensory block, and the MSBL was not as high. There was less increase in block height in the supine position while retaining the pillow under the shoulder. Gradual onset of the block also minimizes the effect of aortocaval compression at the same time that compensatory mechanisms to spinal-induced sympathectomy develop. In addition, we observed after intrathecal injection that the MAP was maintained to within 20% of baseline in group HE. However, group L reached T5 6.3 min after spinal injection; block height increased to T2 15 min thereafter. This was consistent with the decrease in MAP that we observed at that time. In our study, ephedrine requirements both before and after achieving sensory block to T5 were significantly greater in group L than with group HE.
Anesthesiologists might express concern about the slow onset time and the necessity for a smooth, cautious shift from one lateral position to another.12 Considering the advantages of hemodynamic stability and the lower risk of a high block, however, maintaining the head elevated position may be valuable when performing CSE and Caesarean section.
One limitation of the current study is the fact that it was not possible for the anesthesiologist to assess block height and hemodynamic data, as patients in the HE group remained in that position until the end of surgery. In an attempt to limit bias, a second investigator who took no part in the performance of CSE assessed the sensory block and hemodynamic values.
In this study, we demonstrated that maintaining the head elevated position is superior to the lateral to supine position for Caesarean section, as it is associated with a more gradual onset, appropriate sensory block height, and improved hemodynamic stability. Further research will address whether the benefits of the head elevated position are also conferred to the sitting position or other positions.


 XML Download
XML Download