

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Whole-spine sagittal alignment, including cervical lordosis, thoracic kyphosis, and lumbar lordosis, is important for maintenance of horizontal gaze and minimization of energy consumption in the normal state, and there is a close relationship between whole-spine sagittal alignment and pelvic alignment in maintaining global sagittal balance.1,2,3,4,5,6 Previous studies have shown that progression of thoracolumbar deformity influences sagittal and cervical alignment.1,7,8,9 Furthermore, surgical correction of sagittal malalignment by techniques such as lumbar pedicle subtraction osteotomy (PSO) has been shown to improve abnormal cervical hyperlordosis to normal lordosis through reciprocal alignment changes.1
The increase in life expectancy and widespread adoption of diagnostic tools such as MRI has increased the incidence of cervical fusion surgery. Among various cervical fusion surgeries, anterior cervical discectomy and fusion (ACDF), introduced by Smith and Robinson,10 is the most common cervical fusion surgery. ACDF is an established procedure for the treatment of cervical radiculopathy and myelopathy secondary to degenerative disc disease, and several studies have reported good fusion success rates and excellent clinical outcomes.11,12,13,14
Whole-spine alignment is known to change after thoracolumbar deformity correction of cervical lordosis.1,7,8,9 Although cervical fusion surgeries, including ACDF, have become common spine procedures, whole spine alignment changes after ACDF have not previously been investigated in detail. We hypothesized that there might be reciprocal changes in whole-spine sagittal alignment, including thoracolumbar angle and pelvic alignment, followed by changes in cervical alignment after ACDF. We therefore designed this study to assess changes in whole-spine sagittal alignment and pelvic alignment after ACDF.
MATERIALS AND METHODS
Subjects and study design
This retrospective, cross-sectional study included patients who were diagnosed with single-level cervical disc herniation. Forty-eight consecutive patients who had undergone single-level ACDF due to cervical disc herniation with only radiculopathy, not myelopathy, from January 2011 to December 2012 were enrolled in this study. We excluded patients treated for non-degenerative purposes such as trauma, tumor, or infection, as well as patients who had undergone multi-level ACDF, lumbar operations, or other spine operations in order to minimize the possible impacts of surgery on segments other than the cervical spine on whole sagittal balance. In addition, we also excluded patients who had thoracic and lumbar spine pathologies on routine whole-spine sagittal MRI images, as other segment pathologies besides cervical disc herniation might affect whole sagittal alignment. This project was approved by the Institutional Review Board of Gangnam Severance Hospital, Yonsei University College of Medicine (No. 3-2013-0296).
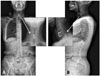
To compare various situation-related operations, patients were divided according to operative method [cage only: Zero-P implant (Synthes GmbH Switzerland, Oberdorf, Switzerland) with autobone; cage & plate: allobone spacer (CG Bio, Seoul, Korea) and Zephir plate (Medtronic Sofamor Danek Inc., Memphis, TN, USA)] (Figs. 1 and 2), operative level (upper level: C3/4, C4/5; lower level: C5/6, C6/7), and preoperative cervical lordosis (high cervical lordosis: preoperative cervical lordosis >12.5°; low cervical lordosis: preoperative cervical lordosis <12.5°).15,16 Preoperative cervical lordosis was classified relative to the mean angle of all patients (12.5°) (Table 1).
Outcome assessment & statistical methods
Arm pain and neck pain were assessed by self-reported measurements using the Visual Analog Scale (VAS) and Neck Disability Index (NDI), respectively. Patients were required to undergo cervical MRI, CT, and whole-spine radiography preoperatively, as well as serial whole-spine radiography at the 1-, 3-, 6-, and 12-month postoperative follow-ups. Cervical lordosis, thoracic kyphosis, lumbar lordosis, sagittal vertical axis (SVA), and pelvic parameters (pelvic incidence, pelvic tilt, and sacral slope) were measured preoperatively and at all follow-ups. Cervical lordosis was measured by determining the Cobb angle between the caudal endplate of C2 and the caudal endplate of C7. Thoracic kyphosis was measured by determining the Cobb angle between the cranial endplate of T4 and the caudal endplate of T12, while lumbar lordosis was measured by determining the Cobb angle between the sacral upper margin and the cranial L1 endplate (Fig. 3).
SVA was measured as the distance between vertical lines through the center of the C7 vertebral body and the S1 superior posterior corner. Pelvic incidence was measured as the angle between the line joining the center of the femoral head with the midpoint of the sacral endplate and the perpendicular line from the midpoint of the sacral endplate. Pelvic tilt was measured as the angle between the line joining the center of the femoral head with the midpoint of the sacral endplate and the vertical line. Sacral slope was measured as the angle between the line along the sacral endplate and the horizontal line (Fig. 3).17,18,19,20 All radiologic parameters were evaluated using PACS software and a PACS workstation (Centricity 3.0, General Electric Medical System, Milwaukee, WI, USA).
Statistical comparisons were performed based on the measured follow-up radiologic date. SPSS for Windows (version 15.0 K; SPSS Inc., Chicago, IL, USA) was used for statistical analyses. The Wilcoxon signed-rank test was used for intragroup comparisons preoperatively and at postoperative 1, 3, 6, and 12 months. For intergroup comparisons, the Mann-Whitney U test was used, and the Pearson correlation test was used to assess the significance of differences in radiologic parameters among groups. p values less than 0.05 were considered statistically significant.
RESULTS
Among 48 patents, 25 were male, and the mean age was 52.9 years (Table 1). Arm pain and neck pain were assessed using VAS and NDI, respectively. There was a significant, sequential improvement in both VAS scores and NDI values postoperatively, relative to the preoperative state (VAS: 6.9±1.1 preoperatively, 1.6±1.8 at 1 month, 1.1±0.6 at 3 months, 1.5±1.2 at 6 months, and 0.6±0.6 at 12 months postoperatively; NDI: 20.0±6.8 preoperatively, 7.9±6.5 at 1 month, 6.9±5.3 at 3 months, 6.1±4.6 at 6 months, and 3.6±3.4 at 12 months postoperatively). Cervical lordosis, pelvic tilt, and sacral slope changed postoperatively relative to the preoperative state. Cervical lordosis significantly decreased at postoperative 1 and 3 months (preoperatively -12.5° to -10.4° at postoperative 1 month and -10.8° at postoperative 3 months; p<0.05) (Table 2). Pelvic tilt was significantly higher postoperatively than at preoperative 12 months (12.0° to 15.0°; p<0.05) (Table 2). Sacral slope was significantly lower at 12 months postoperatively than preoperatively (36.9° to 34.8°; p<0.05) (Table 2). Other radiologic parameters (SVA, thoracic kyphosis, lumbar lordosis, and pelvic incidence) did not show any significant differences between preoperative and postoperative states (Table 2).
Effect of operative method: cage only versus cage & plate
There were 28 patients in the cage-only group (58%) and 20 patients in the cage-&-plate group (42%). There were no significant differences in mean age (cage only: 51.4 years; cage & plate: 55.0 years) or sex (cage only: 15 men, 13 women; cage & plate: 10 men, 10 women) between these two groups (Table 1). Intergroup comparisons of radiologic parameters revealed that cervical lordosis was the only factor that differed significantly between groups. Cervical lordosis at 3 months was -15.6° in the cage-only group compared to -5.9° in the cage-&-plate group (p<0.05) (Table 2).
Intragroup comparison according to operative method, cervical lordosis, and pelvic tilt revealed that these factors changed significantly postoperatively compared to the preoperative state. Cervical lordosis was significantly lower at postoperative 3 months in the cage-&-plate group than preoperatively (-11.5° to -5.9°; p<0.05) (Table 2). Pelvic tilt was significantly higher at postoperative 6 and 12 months in the cage-&-plate group than preoperatively (preoperatively 12.2° to 15.5° at postoperative 6 months and 17.1° at postoperative 12 months; p<0.05) (Table 2).
Effect of operative level: upper level (C3/4, C4/5) and lower level (C5/6, C6/7)
There were 13 patients in the upper-level group (27%) and 35 patients in the lower-level group (73%). There were no significant differences in mean age (upper level: 56.2 years; lower level: 51.7 years) or sex (upper level: 7 men, 6 women; lower level: 18 men, 17 women) between groups (Table 1). Intergroup comparisons of radiologic parameters, SVA, and cervical lordosis showed significant differences. SVA preoperatively and at 1, 3, and 12 months postoperatively was significantly different between groups (upper level: 30.7, 29.4, 21.0, and 29.2 mm; lower level: -17.9, -9.0, -10.3, and -18.1 mm, respectively; p<0.01 preoperatively and 1 month; p<0.05 at 3 and 12 months) (Table 2). Cervical lordosis preoperatively and at 1, 3, and 12 months postoperatively was also significantly different between groups (upper level: -20.0°, -18.2°, -20.1°, and -21.8°; lower level: -9.6°, -6.3°, -9.3°, and -10.6°, respectively; p<0.01 at 12 months; p<0.05 preoperatively and at 1, 3, and 12 months postoperatively) (Table 2).
Intragroup comparison according to operative level, cervical lordosis, pelvic tilt, and sacral slope revealed significant changes postoperatively relative to the preoperative state. Cervical lordosis significantly decreased at postoperative 1 month in the lower-level group (-9.6° to -6.3°; p<0.05) (Table 2). Pelvic tilt was significantly higher at postoperative 12 months in the upper-level group (12.7° to 19.4°; p<0.05) (Table 2). Sacral slope was significantly lower at postoperative 12 months than preoperatively in the upper-level group (35.7° to 31.6°; p<0.05) (Table 2).
Effect of cervical lordosis: high lordosis and low lordosis
There were 21 patients in the high-lordosis group (44%) and 27 patients in the low-lordosis group (56%). There were no significant differences in mean age (high lordosis: 51.1 years; low lordosis: 53.8 years) or sex (high lordosis: 12 men, 9 women; low lordosis: 13 men, 14 women) between the two groups (Table 1). Intergroup comparisons of radiologic parameters revealed significant differences in SVA and cervical lordosis. SVA preoperatively and at 1 and 3 months postoperatively was significantly different between groups (high lordosis: 17.5, 16.2, and 11.1 mm; low lordosis: -20.7, -10.5, and -12.8 mm, respectively; p<0.01 preoperatively; p<0.05 at 1 and 3 months) (Table 2). Cervical lordosis preoperatively and at 1, 3, and 6 months postoperatively was significantly different between groups (high lordosis: -25.9°, -17.6°, -17.8°, and -18.4°; low lordosis: -2.5°, -2.8°, -3.8°, and -6.7°, respectively; p<0.01) (Table 2).
Intragroup comparison according to cervical lordosis revealed that only the high-cervical-lordosis group showed significant changes in SVA, cervical lordosis, pelvic tilt, and sacral slope postoperatively compared to the preoperative state. SVA was significantly shorter at 6 and 12 months postoperatively than the mean preoperative value in the high-lordosis group (17.5 to 4.5 and 5.6 mm, respectively; p<0.01) (Table 2). Cervical lordosis was also significantly lower at postoperative 1, 3, 6, and 12 months relative to the mean preoperative value (-25.9° to -17.6°, -17.8°, -18.4°, and -17.9°, respectively; p<0.01 at 1, 3, and 12 months; p<0.05 at 6 months) (Table 2). Pelvic tilt also showed a significant increase at postoperative 12 months relative to the preoperative mean value (12.0° to 16.7°; p<0.05) (Table 2). Sacral slope was significantly lower at postoperative 12 months than preoperatively (36.4° to 33.3°; p<0.05) (Table 2).
Correlation test
Correlation test results are summarized in Fig. 4 and Table 3. As we found statistically significant changes in SVA, cervical lordosis, pelvic tilt, and sacral slope after ACDF, we performed a Pearson correlation test for SVA, cervical lordosis, pelvic tilt, and sacral slope. SVA was negatively correlated with cervical lordosis and sacral slope and positively correlated with pelvic tilt (Table 3, Fig. 4). Cervical lordosis only showed a negative correlation with SVA (Table 3, Fig. 4). Pelvic tilt was positively correlated with SVA yet negatively correlated with sacral slope (Table 3, Fig. 4). Sacral slope was negatively correlated with SVA and pelvic tilt (Table 3, Fig. 4).
DISCUSSION
Over the last decade, appreciation of the critical role of normal whole-spine sagittal alignment and sagittal pelvic alignment in the maintenance of an economic posture and minimal energy consumption has been increasing.1,2,3,4,5,6 Whole-spine sagittal alignment and pelvic alignment are closely related and can change simultaneously, and sagittal spinopelvic alignment is a complex chain of correlation from the pelvis to the occiput such that changes in one region of the spine can result in reciprocal changes in other spinopelvic regions.1,2,3,4,5,6 Previous studies have tended to focus on the effects of changes in the lower spine (pelvis, lumbar, and thoracic spine) on the upper part (cervical spine).1,8 These studies reported that changes in the balance of the thoracolumbar spine caused reciprocal changes in the whole sagittal spine and cervical spine alignment.1,8,9 Development of spinal instrumentation and osteotomy techniques, such as PSO, has enabled surgical correction of thoracolumbar deformity and positive sagittal malalignment.8 Lumbar PSO to correct sagittal malalignment has been shown to improve abnormal cervical hyperlordosis to normal lordosis through reciprocal change.1,8 In contrast, however, it is not known whether cervical lordosis changes after cervical spine surgery, or how this may affect whole spine sagittal alignment and pelvic alignment.
We investigated 48 patients who underwent single-level ACDF for cervical disc herniation. Cervical deformity is not a common disease, in contrast to thoracolumbar deformity; thus, it is challenging to determine whole-spine sagittal alignment changes after cervical deformity correction. ACDF is the most common cervical fusion procedure; therefore, our goal was to assess whether there were whole-spine sagittal alignment changes after ACDF and to find significant factors that influenced such changes. We did not observe any change in SVA after ACDF; however, cervical lordosis, pelvic tilt, and sacral slope did change after ACDF in the overall group of patients (Table 2). As SVA did not change after ACDF, we could not distinguish whether the change in pelvic alignment (pelvic tilt and sacral slope) was associated with ACDF or whether it occurred independently of ACDF. To determine the relationships among radiologic parameters, we performed correlation tests of significant variables. We found that the correlation between cervical lordosis and SVA and the changes in SVA resulted in changes to pelvic tilt and sacral slope angles (Table 3, Fig. 4).
To find operation-related or patient factors that influenced SVA and pelvic alignment, we compared operative methods (cage only versus cage & plate), operative level (upper level versus lower level), and preoperative cervical lordosis (high cervical lordosis versus low cervical lordosis).15,16 When we performed intragroup comparisons between preoperative status and postoperative 1-, 3-, 6-, and 12-month statuses according to operative method and operative level, we did not observe any changes in SVA after ACDF. This means that the operative methods and levels were not associated with SVA changes after ACDF. We also grouped patients according to preoperative cervical lordosis, as previous studies have reported that correction of thoracolumbar deformity by PSO significantly decreases cervical lordosis and that this results in a reciprocal change to correct cervical hyperlordosis.8 Patients with positive sagittal malalignment could compensate with abnormally-increased cervical lordosis to maintain horizontal gaze; this correction of sagittal malalignment would result in correction of cervical hyperlordosis through reciprocal changes.8
We divided patients into two groups based on mean preoperative cervical lordotic angle: those with an angle >12.5° were assigned to the high-cervical-lordosis group, and those with an angle <12.5° were assigned to the low-cervical-lordosis group. We found that in the high-cervical-lordosis group, cervical lordosis decreased significantly from postoperative 1 month to 12 months, and SVA decreased significantly from 6 months to 12 months; additionally, pelvic tilt increased and sacral slope decreased at postoperative 12 months (Table 2, Fig. 5). Cervical lordosis changed immediately after ACDF and resulted in a change in SVA at postoperative 6 months. The change in SVA resulted in a change in pelvic tilt and sacral slope at postoperative 12 months. This result is the converse of that observed after correction of thoracolumbar deformity by PSO, which changed the pelvic tilt and sacral slope and subsequently decreased the C2-7 plumb line, resulting in reciprocal changes to correct cervical hyperlordosis to neutralization in the cervical-hyperlordosis group.8 Intragroup comparison of the upper-cervical group (C3/4 and C4/5) revealed significant pelvic tilt and sacral slope changes at postoperative 12 months (Table 2). In this group, preoperative cervical lordosis was hyperlordosis (20.0°), which means that the change in pelvic tilt and sacral slope after ACDF in the upper-cervical group was not at the operative level but was instead due to high cervical lordosis preoperatively. In conclusion, ACDF affects whole-spine sagittal balance including SVA, sacral slope, and pelvic tilt between 6 and 12 months postoperatively by changing cervical high lordosis to neutralization. With the swings of SVA, sacral slope, and pelvic tilt in the high-cervical-lordosis group all falling with the normal range, there were no differences in clinical results between the high- and low-cervical-lordosis groups postoperatively in this study.
A reciprocal relationship also exists between lumbar lordosis and thoracic kyphosis, and the sagittal thoracic compensatory curve and pelvic retroversion can normalize after restoration of lumbar lordosis in adolescent idiopathic scoliosis (AIS).1,21,22,23,24,25 In previous studies, cervical kyphosis in AIS with thoracic hypokyphosis was reported. We did not have any cases with thoracic kyphosis or lumbar lordosis changes after ACDF. We only included single-level ACDF and patients with cervical lordosis; therefore, we did not observe any reciprocal changes in the thoracic and lumbar spine. Blondel, et al.21 recently reported normal cervical lordosis from 6.6° to 22.2° for individuals between the ages of 20 and 60 years. The mean cervical lordosis angle in the current study was 12.5°, which is within the range of normal values.8,26 The authors defined high and low cervical lordosis according to the mean preoperative cervical lordosis of all patients (12.5°) (Table 1). This subjective classification of cervical lordosis is a limitation of this study, and our results may have been different had we included cervical kyphosis patients or other cervical deformities.
This study had several limitations: a short follow-up period of one year, a small number of patients, no cervical deformity cases, and no clinical differences according to SVA and cervical lordosis change. In addition, we did not determine the cervical fusion rate. However, several studies have shown that almost all cervical fusion procedures are successful after single-level ACDF; in our study, none of the patients required revision surgery. Nevertheless, long-term follow-up in a larger number of patients, including those with cervical kyphosis and deformities, is required to determine the fusion rate. Radiologic change including cervical lordosis and SVA before and after surgery did not show any clinical relevance or significance. As all preoperative and postoperative radiologic parameters were within the normal range, there was no clinical difference according to changes in radiologic parameters. In addition, from this study it is impossible to know the exact reasons as to why only high cervical lordosis patients had an altered sagittal alignment and not those in the low-cervical-lordosis group, as this study only included the one-segment ACDF and the range of high cervical lordosis was within the normal range. From the previous studies on thoracolumbar deformity, PSO was reported to have changed the pelvic tilt and sacral slope, which changed SVA and resulted in reciprocal changes to correct cervical hyperlordosis to neutralization in the cervical-hyperlordosis group.8 However, this study did not include abnormal cervical hyperlordosis and kyphosis cases. Further studies that include various cervical deformities with abnormal high cervical lordosis and kyphosis are required.
Despite these limitations, ACDF was found to affect whole-spine sagittal alignment and pelvic alignment, especially in patients with high cervical lordosis. After ACDF, cervical lordosis decreased in the high-cervical-lordosis group, SVA decreased, pelvic tilt increased, and sacral slope decreased in sequential order. Cervical lordosis and whole-spine sagittal alignment were strongly correlated after ACDF.







 XML Download
XML Download