

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Stenotrophomonas maltophilia (S. maltophilia) is an emergent pathogen in healthcare facilities worldwide, causing mainly pneumonia or septicemia related or unrelated to catheter use. Patients with immunodeficiency are especially at risk.1,2,3 Serious infection attributed to S. maltophilia is a significant cause of mortality in patients with hematologic malignancies,4 with mortality rates up to 37.5%.5
S. maltophilia is intrinsically resistant to antibiotics that could be excluded by multidrug efflux pumps and/or inactivated by β-lactamase and aminoglycoside-modifying enzymes.6 Trimethoprim-sulfamethoxazole (TMP-SMX), historically the first line of defense in S. maltophilia infection,7 may induce resistance related to class 1 integrons containing the sul1 sulfonamide resistance gene and insertion element common region elements containing the sul2 resistance gene.6,8,9 However, rates reported for resistance to TMP-SMX in S. maltophilia are generally less than 10%.10,11,12
Clinically, the use of TMP-SMX in S. maltophilia infection is limited by adverse effects of the drug, including skin eruptions, hepato- and renal toxicity, and bone marrow suppression.7,13 Additionally, resistance to TMP-SMX in S. maltophilia is increasing at certain centers.8,13
Fluoroquinolones, including levofloxacin and moxifloxacin, are an attractive alternative for treating S. maltophilia infection, because they are well-tolerated and effective, compared to TMP-SMX, and because of their low rates of microbial resistance.7,11,13,14,15,16 However, S. maltophilia can rapidly acquire resistance to fluoroquinolones, especially in monotherapy, and this may limit their use in combination therapy.17 In this study, we investigated the poorly understood relationships between clinical factors and the acquisition of levofloxacin resistance in S. maltophilia.
MATERIALS AND METHODS
Subjects and study design
This retrospective cohort study was conducted at Severance Hospital, a 2000-bed university-affiliated teaching hospital and tertiary care referral center in Seoul, South Korea, based on data collected from January 2008 to June 2010. Patients who met all of the following conditions were eligible for this study: 1) age 18 years old or older; 2) ≥3 serial isolations of S. maltophilia by culture, accompanied by in vitro antimicrobial susceptibility testing (AST) in any clinical specimen; and 3) results for three or more consecutive ASTs of S. maltophilia for levofloxacin in clinical specimens from the same system (e.g., the respiratory, urinary or biliary tract, peritoneal or pleural fluid, or an external wound) at intervals from 3 days to 3 months.
We screened the data for 3029 S. maltophilia isolates from 1275 patients, and identified 528 isolates with data for serial isolation and all AST results from 122 patients (Fig. 1). We stratified these 122 patients into either the SS group (n=54) whose records showed maintenance of levofloxacin susceptibility from the first S. maltophilia isolate to the last isolate recorded or the SR group (n=31) with data confirming transition from levofloxacin susceptibility to resistance in serial S. maltophilia isolates. However, we excluded an RR group (85 isolates from 21 patients) whose records revealed the maintenance of levofloxacin resistance from the first S. maltophilia isolate to the last isolate recorded from our study analysis. Additionally, patients (12 isolates from 4 patients) with data confirming transition from levofloxacin resistance to susceptibility and patients (86 isolates from 12 patients) with inconstant AST results for levofloxacin were excluded from the analysis (Fig. 1).
In vitro antimicrobial susceptibility testing
All bacterial species were identified using conventional methods and/or the ATB 32GN system (bioMerieux, Marcy l'Etoile, France). Antimicrobial susceptibility was tested by the Clinical and Laboratory Standards Institute (CLSI) agar dilution method.18 The antimicrobial agents used for AST were TMP-SMX (Dong Wha Pharmaceutical Co. Ltd., Seoul, Korea); levofloxacin (Daiichi Sankyo Co. Ltd., Tokyo, Japan); minocycline (SK Chemicals Co. Ltd., Life Sciences, Seoul, Korea); ceftazidime, amikacin, and gentamicin (Sigma Chemical Co., St. Louis, MO, USA); tigecycline (Wyeth Research, Pearl River, NY, USA); imipenem (Choongwae Pharma Corp., Seoul, Korea); and piperacillin/tazobactam (Yuhan Co. Ltd., Seoul, Korea).
Definitions
The index isolate was defined as the last levofloxacin-susceptible isolate cultured from a patient in the SS group and as the first levofloxacin-resistant isolate from one patient in the SR group.
Data collection
The clinical data at the time of identification of the index isolate were collected through review of electronic medical records. Coexisting conditions of interest included length of hospital stay, intensive care unit admission, use of mechanical ventilation, current tracheostomy status, acute renal failure (ARF) with renal replacement therapy (RRT), neutropenia, and steroid or immunosuppressant use, as well as the Charlson's comorbidity index score. We recorded the history and total duration of all systemic antibiotic exposures within 3 months from identification of the index isolate. To evaluate the effect of co-infection or co-colonization with other bacteria on the acquisition of resistance to levofloxacin in S. maltophilia, the data for co-infection or co-colonization were evaluated in parallel with results of AST for fluoroquinolones.
Statistical analysis
Categorical data are expressed as a number (percent). If the continuous variables had normal distribution, these were expressed as mean±standard deviation. Continuous variables without normal distribution were expressed as median (interquartile range). We used Student's t-test or Mann-Whitney U test and the χ2 test or Fisher's exact test to compare continuous and categorical variables, respectively, in a univariate analysis of clinical characteristics in the SR and SS groups. Variables with p-values less than 0.10 in univariate analysis were included in a multivariate logistic regression analysis to identify clinical factors associated with acquisition of levofloxacin resistance in S. maltophilia. Results from the multivariate analysis are expressed as an odds ratio (OR) and 95% confidence intervals (CIs). A two-tailed p-values <0.05 was taken to indicate significance. All statistical analyses were performed using SPSS 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
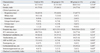
The SS and SR groups were similar in age and gender (Table 1). A significantly higher proportion of patients in the SR group than in the SS group were in ARF requiring RRT (25.8% vs. 7.4%, p=0.026). Other coexisting conditions did not differ significantly between the two groups (Table 1).
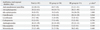
The total duration of exposure to levofloxacin within 3 months from identification of the index isolate was significantly longer in the SR group [33 (9-42) days] than the SS group [11 (4-64) days, p=0.044] (Table 2). However, the total duration of exposure to anti-pseudomonal penicillins, 3rd cephalosporins, 4th cephalosporins, ciprofloxacin, carbapenems, aminoglycosides, glycopeptides, and metronidazole did not show significant differences between the SS and SR groups (Table 2). Co-infection or co-colonization with ciprofloxacin-resistant Staphylococcus aureus was significantly more common in the SS group than in the SR group (31.5% vs. 9.7%, p=0.032). The SR group had significantly higher percentages of co-infection or co-colonization with any gram-negative bacteria and with Klebsiella pneumonia resistant to levofloxacin (58.1% vs. 35.2%, p=0.041; 32.3% vs. 9.3%, p=0.007, respectively) (Table 3).
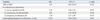
In the final multivariate logistic regression analysis, exposure to levofloxacin for more than 3 weeks (OR 15.39, 95% CI 3.08-76.93, p=0.001) and co-infection or co-colonization with K. pneumoniae resistant to levofloxacin (OR 4.85, 95% CI 1.16-20.24, p=0.030) were clinical factors independently associated with the acquisition of resistance to levofloxacin in S. maltophilia (Table 4).
DISCUSSION
This study confirmed the acquisition of levofloxacin resistance in S. maltophilia during clinical application of the drug. S. maltophilia may potentially develop resistance to fluoroquinolones through various mechanisms, including 1) efflux pump systems, such as SmeABC and SmeDEF,19,20 or 2) mutations in outer-membrane porin proteins.21 A previous study suggested that spontaneous mutations conferring resistance to fluoroquinolones occur at frequencies between 10-5 to 10-752 after quinolones therapy in S. maltophilia.22 In a clinical study at the MD. Anderson Cancer Center, use of fluoroquinolones in the previous 90 days was independently associated with emergence of multidrug resistant S. maltophilia infection in cancer patients.23 In a case-control study, Spanik, et al.24 found a positive association of prophylactic fluoroquinolones use with bacteremia by MDR gram-negative bacilli including S. maltophilia in neutropenic cancer patients. Thus experimental and clinical data from multiple studies, including this one, associate fluoroquinolones exposure with acquired resistance to fluoroquinolones in S. maltophilia.
Co-infection or co-colonization with levofloxacin-resistant K. pneumoniae presented another independent clinical factor in acquisition of levofloxacin resistance in S. maltophilia. Co-infection and co-colonization with other bacterial species, especially those with resistance to fluoroquinolones, are clinically relevant because the species may actively exchange drug resistance genes by means of plasmids and transposons.25 Clinical co-infection of S. maltophilia with other pathogens (e.g., other glucose-non-fermenting gram-negative bacteria including Pseudomonas aeruginosa, Burkholderia species and Acinetobacter baumannii; Enterobacteriaceae including Escherichia coli, Klebsiella species and Enterobacter species; Staphylococcus aureus including methicillin-resistant S. aureus; Enterococcus species; Bacteroides species; and Candida albicans) is confirmed through recovery of multiple species from patient samples.26,27,28,29 S. maltophilia can also exchange antibiotic-resistance genes with gram-positive and other gram-negative bacteria.30 The Smqnr gene present in the bacterial chromosome contributes to intrinsic quinolones resistance in S. maltophilia.31 Although S. maltophilia isolates harboring Smqnr genes could serve as a reservoir for horizontal transfer of these genes into Enterobacteriaceae, this event is unlikely to occur because plasmids containing Smqnr are unstable.21,32 As the possibility and mechanism for the transfer of levofloxacin resistance gene from other gram-negative bacteria to S. maltophilia have not been fully evaluated, further in vitro study is warranted to verify the association of S. maltophilia with K. pneumoniae with levofloxacin resistance.
To our knowledge, no study has systematically evaluated clinical factors that influence acquisition of levofloxacin resistance in S. maltophilia. To identify such factors, we followed levofloxacin susceptibility in serial isolates of S. maltophilia from 122 individual patients (i.e., longitudinally) and compared characteristics of patient subgroups in which susceptibility was maintained (the SS group) and not maintained (the SR group). Although patients with cystic fibrosis usually suffer the respiratory tract infection with S. maltophilia, there were not any patients with cystic fibrosis in this study because of the extremely low prevalence of cystic fibrosis in South Korea.33
The limitations of our study include the retrospective design with data from a single center only and the non-standardization of protocols for antimicrobial sensitivity testing in S. maltophilia. The results of an AST performed by disc diffusion, an E-test, and agar dilution may vary and may not correlate with in vivo effectiveness.34 The British Society for Antimicrobial Chemotherapy (BSAC) recommends only disk diffusion and agar dilution testing for TMP-SMX, while the CLSI generally recommends only disk diffusion testing and agar dilution testing for TMP-SMX, levofloxacin, and minocycline.18 We performed AST using the most recent revision of CLSI recommendations, the guideline that is most widely available. We further assumed that transitions between CLSI and BSAC recommendations for the AST would not affect the results of our regression analysis.
In conclusion, appropriate restrictions on the use of levofloxacin, currently among the commonly used antibiotics for S. maltophilia infection, may be necessary to prevent the emergence of levofloxacin resistance in S. maltophilia. Further study of this resistance through molecular epidemiologic analysis may clarify these clinical findings.


 XML Download
XML Download