

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Many older asthma patients have pathobiological and symptomatic features of the overlap phenotype of asthma and chronic obstructive pulmonary disease (COPD), necessitating a re-evaluation of the concept of both diseases as separate conditions. From a clinical point of view, the overlap phenotype is composed of COPD patients with increased reversibility and/or of asthmatics with fixed or incompletely reversible airflow obstruction. Its prevalence reports recently estimated that about 13-20% of subjects with COPD have the overlap phenotype, with an increasing trend in the elderly population.1,2,3,4 Physiological ageing of the lung is associated with a decrease in the static elastic recoil, a decrease in compliance of the chest wall, and a decrease in the strength of respiratory muscles. This can lead to decrease of lung function. Also senile emphysema can occur, contributing to the decrement in expiratory flow with ageing.5
Elderly asthmatics are known to have higher rates of airway hyperresponsiveness, more severe asthma, and more difficult to control with corticosteroids.6,7 The Dutch Hypothesis quotes that asthma itself and airway hyperresponsiveness (AHR) predispose patients to develop COPD later in life.8
Patients with the overlap phenotype are known to have worse lung function, more respiratory symptoms, and a lower health-related quality of life than either disease alone.9,10 Recently, the diagnostic criteria for the overlap phenotype has been established by the consensus of a group of experts.11 However, this is limited to COPD patients, but not for the asthma with fixed airflow obstruction.
The aim of this study was to analyze clinical characteristics and lung function of the overlap phenotype of asthma with COPD feature, in the perspective of asthma patients. Most of the previous studies were investigated from COPD perspective. The benefit of our study is that we tried to approach overlap in the perspective of asthma as they may have different clinical and functional characteristics to COPD patients with increased reversibility.
MATERIALS AND METHODS
The medical records of all consecutive patients who were diagnosed with asthma at Seoul St. Mary's Hospital, The Catholic University of Korea, South Korea, between September 2007 and March 2012 were retrospectively reviewed. The study was approved by the Institutional Review Board of the Seoul St. Mary's Hospital, to evaluate and publish information from the patients' records. The requirement for informed consent was waived because of the retrospective nature of the study.
Study subjects and baseline data
We identified all out- and inpatients at Seoul St. Mary's Hospital, aged 41-79 years with a diagnosis of asthma in the set period. The identified cases were checked to ascertain whether they met the following criteria of asthma: Physician's diagnosis of asthma by specialists in pulmonary and allergy departments with either 1) positive response to bronchodilator: >200 mL forced expiratory volume in 1 s (FEV1) and >12% baseline and/or 2) positive methacholine or mannitol provocation test. All enrolled patients had at least one chronic persistent respiratory symptom consisting of cough, wheezing, dyspnea and chest tightness worsening at night or in the early morning for more than 3 months. Subjects who did not meet these criteria were excluded. Patients with the following diagnosis, based on history or tests, were excluded: COPD patients (defined by a post-bronchodilator FEV1/forced vital capacity (FVC) ratio of <0.70 due to GOLD criteria12) and with negative bronchodilator and/or bronchoprovocation response, bronchiectasis, tuberculosis destroyed lung, allergic bronchopulmonary aspergillosis, anthracofibrosis, interstitial lung disease, malignancy, and heart failure.
The enrolled study population was divided into two groups according to the presence of airflow obstruction. We defined overlap patients who had incompletely reversible airflow obstruction (postbronchodilator FEV1/FVC <70) at the time of initial admission and continuing airflow obstruction after at least 3 months follow-up regardless of treatment. Asthma only patients were defined as having postbronchodilator FEV1/FVC ≥70. Initial asthma patients with airflow obstruction who recovered from obstruction (FEV1/FVC ≥70) in their follow-up pulmonary function tests (PFTs) were allocated in the asthma only group. Subjects who did not have follow up lung function results were excluded as they did not meet our definition. The baseline clinical data included demographic data, smoking history, body mass index, height, spirometry, lung volumes, diffusing capacity, methacholine and mannitol provocation challenges, bronchodilator responses (BDRs), serum eosinophil percentage, serum eosinophil count, total serum immunoglobulin (Ig) E count and skin test results. All of the tests mentioned above were performed within one week.
Pulmonary function tests
PFTs were performed in all patients by three technicians experienced in lung function testing following American Thoracic Society (ATS)/European Respiratory Society (ERS)guidelines in a licensed laboratory.13,14 Spirometry and body plethysmography were performed according to current recommendations.13,14 The residual volume (RV), functional residual capacity (FRC) and total lung capacity (TLC) were determined by body plethysmograph. Diffusing capacity of the lung for carbon monoxide (DLCO) was measured in duplicate by the single-breath method according to ATS/ERS guidelines.15 Post-bronchodilator (BD) FEV1 (ΔFEV1) was measured 15 min after the administration of 400 mcg salbutamol using a metered dose inhaler and a large volume spacer.
According to ATS guidelines, medications that can decrease airway responsiveness were withheld before the test.16
Bronchoprovocation tests
Non-specific bronchial responsiveness was assessed by bronchial challenge with methacholine chloride and mannitol. Bronchoprovocation tests using methacholine were performed in accordance with ATS guidelines.16 The methacholine challenge schedule started with an inhalation of saline, followed by increasing concentrations of methacholine up to a cumulative dose of 25 mg/mL. The test was stopped when either the maximum cumulative dose had been reached or FEV1 had fallen by 20% or more. Positive methacholine results were defined as provocative concentration of methacholine required to decrease FEV1 (PC20) by 20% less than or equal to 16 mg/mL.16
Dry powder mannitol (Aridol; Pharmaxis, Sydney, Australia) was administered according to the recommendations of the manufacturer, and FEV1 was recorded in line with current guidelines.17 The mannitol challenge schedule started with an inhalation of 0 mg placebo, followed by increasing concentrations of mannitol up to a cumulative dose of 635 mg. The challenge was stopped when FEV1 decreased of 15% or more from baseline values or when the maximum cumulative dose of 635 mg had been administered. Positive mannitol results were defined as PD15 less than or equal to 635 mg.17,18 Patients with severe airflow limitation (FEV1 <50% predicted or <1.0 L) were contraindicated for bronchoprovocation tests. Medications that can decrease airway responsiveness were withheld before the test, according to ATS guidelines.16
Evaluation of allergy and atopy
Atopy was defined as either at least one positive specific IgE or one positive skin prick test to aeroallergens (cat, dog, house dust mite, grasses, and fungi). Skin prick test was considered positive when there was a 3 mm or larger wheal and/or erythema of 10 mm or more, greater than the negative control. All patients were asked to discontinue using antihistamine for 3 days prior to testing.19 Furthermore, the increase of eosinophils, eosinophil count, and total IgE were analyzed between groups.
Data analysis
Continuous variables are presented as mean±standard error of mean and analyzed using two independent sample t-test. Categorical variables are presented as frequency and percentage and analyzed using Pearson's chi-square tests or Fisher's exact tests. All tests were two-sided, and p-value <0.05 was considered statistically significant. All analyses were performed with the SPSS computer package, version 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
During the study period, 1898 patients with a suspected diagnosis of asthma were enrolled. After evaluation, a total of 566 (30%) eligible patients who had asthma according to the definition criteria were included: all relevant clinical data and initial spirometry results were available for these patients. Of these patients, we excluded 310 patients who did not follow up PFTs. Thus, a total of 256 asthma patients (13.4%) were enrolled in the study.
We divided the 256 asthma patients into two groups according to the presence of airflow obstruction. Finally, 159 (62%) patients were enrolled in the asthma only group and 97 (38%) patients in the overlap group.
Clinical characteristics of enrolled patients
The clinical characteristics of 256 asthma patients are shown in Table 1. The overlap group was older (63.0±0.9 vs. 57.6±0.7, p<0.01) and had more males (37.1% vs. 18.2%, p<0.01) than the asthma only group. There was higher percentage of current or ex-smokers (46.2% vs. 14.9%, p<0.01) in the overlap group.
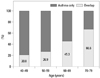
Percentage of patients with the overlap phenotype in different age groups are shown in Fig. 1. Among subjects with asthma, the percentage of overlap was 20.8%, 26.9%, 45.3%, and 66.6% in the 40-49, 50-59, 60-69, and 70-79 years age groups, respectively (Fig. 1). The highest percentage was shown in the 70 s.
Allergic test findings
Allergic test results are shown in Table 1. Significantly lower serum eosinophil count (267.8±32.7 vs. 477.5±68.9, p=0.02) and higher IgE (332.1±74.0 vs. 199.8±33.4, p=0.03) were seen in the overlap group. However, there was no significant difference in positive allergic skin test results in either group.
Pulmonary function test findings
Pulmonary function test findings at the time of presentation are shown in Table 2. The overlap group had lower FEV1 (58.0±1.2% vs. 69.4±1.2%, p<0.01), and higher TLC (111.1±2.2% vs. 101.6±1.6%, p<0.01), FRC (125.2±4.0% vs. 101.9±2.3%, p<0.01), and RV (125.6±6.0% vs. 99.0± 3.9%, p<0.01). There was no significant difference in DLCO values in both groups.
There was no significant difference in AHR with either methacholine or mannitol and BDR in the two groups. However, the mean PC20 (3.9 vs. 6.4, p<0.01), and PD15 (63.2 vs. 236.0, p<0.01) values were significantly lower in the overlap group, as shown in Table 2.
DISCUSSION
It is often difficult to clinically distinguish overlapping COPD and asthma, and there have been many studies to investigate the characteristics of such phenotype.1,2,3,4,6,20 Diagnostic criteria for this overlap phenotype in COPD have been proposed, including positive BDR, eosinophilia in sputum, personal history of asthma before age 40 years, high total IgE level, and a personal history of atopy.11 However, this was investigated from COPD perspective. From the perspective of asthma, overlap phenotype can be defined as asthmatics with fixed airflow obstruction.2 To investigate the overlap phenotype from the perspective of asthma, we excluded COPD patients without asthmatic components.
Previous studies showed that asthma is a risk factor for the development of fixed airflow obstruction,8,21 while cigarette smoking is the main risk factor for the development of persistent airflow obstruction in asthmatics.22 Asthmatics with a history of smoking, exhibit higher numbers of neutrophils in bronchoalveolar lavage fluid and biopsies.23,24 In our present study, we defined the overlap group within our enrolled asthma patients, which is different from other studies. In the diagnosis of asthma, we excluded physician's diagnosis of asthma without either positive BD or provocation results because of the potential inaccuracy. To try and differentiate overlap, which shows persistent irreversible obstruction, from severe asthma with reversible airflow obstruction, patients who recovered airflow obstruction at follow up PFTs (at least 3 months interval) were designated in the asthma group. Patients who did not have follow-up PFTs were excluded. Of the initial 566 asthma patients, we only enrolled 256 patients with follow up PFTs.
In our asthma clinic cohort, the prevalence of overlap was approximately half of that of asthma only (37.9% vs. 62.1%). This finding is consistent with a previous study that the prevalence of overlap is nearly half of that of asthma (24.3% vs. 52.9%), representing a significant proportion of patients with both phenotypes.6 In our cohort, the highest percentage was observed in patients in their 70 s, and large population studies found that the prevalence of this overlap phenotype increases with age.4,6 In our study, the age distribution also followed this trend. Age is a very important variable when assessing obstructive lung diseases, due to the known changes in lung function that occur with increased age.5 A combination of exercise intolerance, static or dynamic hyperinflation and senile emphysema in the elderly patient can lead to a decrease in lung function.5 The annual decrease in FEV1 is approximately 20 mL/year in subjects up to age 40 years and is approximately double that number when an individual's age is greater than 65 years. The decrease in FEV1 is slightly greater than that in FVC, particularly from 50 to 60 years of age, resulting in a decrease in the FEV1/FVC ratio in older individuals.5,25
Furthermore, there was significant increase of ex-smokers in the overlap group. It is known that asthmatics who smoke have more neutrophils in their airways, leading to steroid resistance.19,20 This in turn can lead to more severe symptoms and an accelerated decline in lung function.21,22
Total IgE was significantly increased in the overlap group compared to the asthma only group. Atopic persons often have increased plasma total IgE concentrations, and quantitative IgE antibodies may serve as a marker of asthma severity.26,27 It has been reported that AHR to methacholine is correlated with the level of total IgE in the serum, which has been observed not only in subjects with asthma and rhinitis, but also in asymptomatic subjects.28 Based on these findings, we conclude that more severe degree of atopy in asthma patients may lead to the development of mixed phenotype.
In the present study, we compared pulmonary function between the two groups, and observed a lower FEV1 in the overlap group. This could be explained by the fact that the overlap group had more smokers than the asthma only group. Moreover, asthma itself is significantly associated with an increased risk for chronic bronchitis, emphysema and COPD compared to nonasthmatic subjects, and smoking significantly accelerates the decline in lung function in subjects with or without asthma.21,29 It is well known that cigarette smoking accelerates the loss of lung function by up to 50 mL per year.30 Its effect may be greater in asthmatic smokers, since they have more severe asthma symptoms, accelerated decline in FEV1, reduced response to corticosteroids and increased neutrophilic airway inflammation.31,32,33,34
Previous studies have suggested that factors associated with accelerated lung function decline in asthma also include more severe AHR, adult-onset asthma, frequent severe exacerbations, persistent symptoms, baseline airflow obstruction and persistent elevation of exhaled nitric oxide (NO).35,36,37 In the present study, we found more severe AHR in the overlap group which could be an another contributing factor of lower pulmonary function and irreversible airway obstruction.
We evaluated lung volume in both groups (asthma only; n=66, overlap; n=39). In the overlap group, TLC, FRC, and RV were significantly increased compared to the asthma only group, indicating that air trapping was more severe in the overlap group, in good agreement with a previous study that the overlap group had more gas trapping on expiratory chest CT scans compared to subjects with COPD alone.3 Unfortunately, we were not able to evaluate CT imaging studies since this was a retrospective study. More imaging studies are needed to differentiate the two groups in the future.
The findings in the present study led us to suggest that the mechanisms behind the differences between the two groups involve the combination of aging, cigarette smoking and airway remodeling. First, aging has an effect on decreased lung function, as seen previously.5,25 Second, cigarette smoking in asthmatic patients can significantly accelerate the decline in lung function and increase the risk of COPD.21,29 Third, asthmatic patients can develop airway remodeling as a consequence of persistent airway inflammation which can lead to fixed airflow obstruction. Therefore, these three factors may contribute to the manifestation of overlap syndrome. To what extent they individually contribute to the disease remains unclear and needs to be studied further.
One limitation of this study is the possibility that selection bias might have influenced the significance of our findings, given its retrospective nature. However, a strict diagnostic criteria for asthma was applied to the patients during the enrolling process. As a result, only 13.4% (256 cases) of patients out of 1898 cases of suspected asthma, were enrolled in the study. Thus, we are quite certain that our diagnosis of asthma was reliable, as patients with only the physician's diagnosis of asthma have potential inaccuracy and they were excluded. In our study, we evaluated the differences in lung functions and airway hyperresponsiveness in both groups, and therefore, initial and follow up PFTs were essential to our study. The patients without follow up PFT results were also excluded. Another limitation is the lack of evaluation in inflammatory markers, such as sputum eosinophil and neutrophil counts or exhaled NO. Comparison of these markers would have assisted in comparing the pathologic differences in these two groups.
In conclusion, the overlap phenotype was found to be older, male asthmatic patients who had a higher lifetime smoking intensity and an increased total serum IgE. Lung functions in this group showed lower FEV1 and higher TLC, FRC and RV which suggests more air trapping. The causes of differences between the two groups may be due to the combination of aging, smoking and airway remodeling. Further studies on this overlap phenotype are needed to establish definite diagnostic criteria in asthmatic patients.


 XML Download
XML Download