

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Methicillin-resistant Staphylococcus aureus (MRSA) is a well-known cause of hospital-acquired pneumonia (HAP) or ventilator-associated pneumonia, representing 20-40% of infections.1,2 Unlike the previous confinement of MRSA to healthcare settings, MRSA has also emerged as an important pathogen in non-nosocomial pneumonia, comprising up to 20% of healthcare-associated pneumonia (HCAP) cases and up to 10% of community-acquired pneumonia (CAP) cases.3,4,5,6,7
MRSA pneumonia is likely to be severe and life-threatening, with high mortality, compared with non-MRSA pneumonia.8,9,10 Rapidly progressive necrotizing pneumonia, due to community-associated MRSA, is notable for its high morbidity and mortality, even in relatively young and previously healthy patients.11 Although treatment of MRSA pneumonia is typically universal, starting with glycopeptide antimicrobial therapy, regardless of the source of infection (i.e., hospital- or community-acquired) different risk factors, transmission, clinical courses, and antibiotic resistance patterns have been reported between hospital-acquired (HA-) and community-acquired MRSA (CA-MRSA) pneumonia.12,13
Recently, HCAP and CAP have garnered greater concern; however, the exact incidence of non-nosocomial pneumonia with MRSA is difficult to determine. Although there are a number of case reports and small case series in the literature, there has yet to be any substantial epidemiologic study. HCAP has been described as pneumonia more similar to HAP than CAP in terms of epidemiological patterns and prognosis.14,15,16 However, the influence of MRSA on the different characteristics of HCAP and CAP is not well-known.
As CAP and HCAP are classified as different types of pneumonia, the purpose of this study was to examine the incidences of MRSA CAP and MRSA HCAP. We also attempted to determine the impact of MRSA on differences in clinical characteristics, treatment outcomes, and medical expenses between CAP and HCAP.
MATERIALS AND METHODS
Study design and subjects
We conducted a retrospective observational study on adult patients (≥20 years old) admitted with MRSA pneumonia at Severance Hospital (a university-affiliated tertiary hospital) in South Korea between January 2008 and December 2011. Among 943 pneumonia patients with identified pathogens, 78 patients with MRSA pneumonia were included in this study. Patients were classified into CAP or HCAP groups. We compared baseline characteristics, treatment outcomes, medical expenses, and drug resistance patterns between the groups. This study protocol was approved by the Institutional Review Board of Severance Hospital.
Definitions
Pneumonia was defined as the presence of a new infiltrate on chest radiograms with at least one of the following symptoms: fever or hypothermia, cough with or without sputum, chest pain, dyspnea, or altered breath sounds on auscultation.17
CAP and HCAP were defined according to American Thoracic
Society/Infectious Diseases Society America (ATS/IDSA) guidelines.18 HCAP included patients with at least one of the following criteria: hospitalization within 90 days before the pneumonia diagnosis, admission from a nursing home or a long-term care facility, infusion therapy such as that with intravenous antibiotics, chemotherapy, or wound care within 30 days before the pneumonia diagnosis, and/or chronic hemodialysis or peritoneal dialysis.18
We defined immunosuppressed patients as those that comprised at least one of following: daily treatment with systemic corticosteroids (≥15 mg of prednisone/day for more than 1 month) or combination therapy with low-dose corticosteroids and other immunosuppressants (azathioprine, mycophenolate, methotrexate, cyclosporine, or cyclophosphamide), seropositivity for human immunodeficiency virus, receipt of a solid organ or bone marrow transplant, radiation therapy or chemotherapy for an underlying malignancy within 6 months prior to hospital admission, or diagnosis with an underlying acquired immune deficiency disorder.19
Total hospital charges included all medical expenses during hospitalization, except charges for a hospital room.
Microbiological studies
Pathogens from sputum, blood, bronchoalveolar lavage fluid, pleural effusion, or lung abscesses were investigated using standard microbiological procedures. Blood cultures were considered as an etiological diagnosis if there was no other infection source for a positive blood culture. Sputum samples were cultured using semi-quantitative manner and an etiological diagnosis was confirmed when a predominant microorganism was isolated from group 4 or 5 sputum, according to Murray and Washington's grading system.20 MRSA pneumonia was defined as pneumonia coinciding with isolation of MRSA as the only potential pathogen. The qualitative polymerase chain reaction (PCR) amplification of mecA is a rapid and sensitive method for detecting MRSA, but cultures were used because of high rate of false positives in PCR method.21 VITEK system was used to evaluate minimum inhibitory concentrations (MICs) of antimicrobial agents.
Patients were treated in accordance with ATS/IDSA guidelines although the detailed antibiotic regimens were decided by the attending physician, taking into consideration patient risk factors and the severity of the disease.
Statistics
We conducted univariate analyses with the χ2 test or Fisher's exact test for categorical variables and the Mann-Whitney U test for continuous variables. Non-normally distributed variables are presented as medians (interquartile range). All tests were two-sided, and a p value <0.05 was deemed to indicate statistical significance. SPSS software (ver. 18.0; SPSS Inc., Chicago, IL, USA) was used for all statistical analyses.
RESULTS
Incidence of MRSA in culture-positive CAP and HCAP during 2008-2011
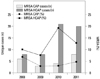
The total number of hospitalized patients with non-nosocomial culture-positive pneumonia was 943 (496 in CAP, 447 in HCAP) between January 2008 and December 2011. The total numbers of culture-positive CAP and HCAP for each year are as follows: 86 and 79 in 2008, 105 and 105 in 2009, 133 and 108 in 2010, and 172 and 155 in 2011, respectively. The incidence of MRSA in non-nosocomial culture-positive CAP and HCAP was 4.2% and 12.8% over the 4 years. The change in the proportion of MRSA is shown in Fig. 1. While the proportion of MRSA in culture-positive CAP increased from 2.9% in 2009 to 4.7% in 2011 that in culture-positive HCAP fluctuated between 7.6% and 19.4%. MRSA pneumonia was observed most frequently in April (16.7%), November (12.8%), and December (11.5%).
Baseline characteristics
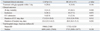
Among the 78 patients with MRSA pneumonia, 21 (26.9%) presented with CAP and 57 (73.1%) presented with HCAP. Baseline characteristics of the patients with MRSA CAP and MRSA HCAP are listed in Table 1. Median ages in the MRSA CAP and MRSA HCAP groups were 73 (60.5-77.5) and 71 (66.0-79.5) years old, respectively (p=0.491). Males were dominant in both groups (76.2% in MRSA CAP vs. 73.7% in MRSA HCAP; p=1.000) and hypertension was the most predominant underlying disease in both groups (52.4% in MRSA CAP vs. 57.9% in MRSA HCAP; p=0.798). Hypoxemia at admission was observed in more than half of the patients in both groups (66.7% in MRSA CAP vs. 61.4% in MRSA HCAP; p=0.794), while shock (38.1% vs. 21.1%; p=0.15) and MRSA bacteremia (28.6% vs. 17.5%; p=0.346) tended to occur more in MRSA CAP than in MRSA HCAP. Immunosuppressed status (35.1% vs. 19.0%; p=0.269) and previous MRSA infection history within 1 year (29.8% vs. 14.3%; p=0.244) tended to be more common in MRSA HCAP than in MRSA CAP, but without statistical significance. CURB65 scores and Pneumonia Severity Index scores did not differ between the groups.
Chest radiographs
Chest radiograph findings did not differ between the groups. Multiple infiltrates were the most common finding in both groups (52.4% in MRSA CAP and 40.4% in MRSA HCAP; p=0.342) (Table 2). Diffuse bilateral infiltrates tended to be more common in HCAP than in CAP (38.6% vs. 23.8%; p=0.223). Pleural effusion was observed in about one-fifth of patients in both groups, but no empyema was observed.
Antibiotic treatment and clinical outcomes
Treatments and clinical outcomes of pneumonia patients with MRSA CAP and MRSA HCAP are shown in Table 3. Treatment with glycopeptides within 1 day was higher for MRSA CAP than for MRSA HCAP, but without statistical significance (28.6% vs. 14.0%; p=0.184). Intubation rates (38.1% vs. 17.5%; p=0.072) and intensive care unit (ICU) admission (42.9% vs. 22.8%; p=0.095) tended to be higher in MRSA CAP, while 28-day mortality tended to be higher in MRSA HCAP (14.3% vs. 26.3%; p=0.368). The median total hospital charges were 6899 American dollars in MRSA CAP and 5715 American dollars in MRSA HCAP (p=0.161).
Drug resistance patterns
Drug resistance patterns of MRSA pathogens in MRSA CAP and MRSA HCAP are shown in Table 4. Comparing various drugs resistances, MRSA HCAP showed significantly more resistance to gentamicin than MRSA CAP (58.3% vs. 16.6%; p=0.037). Ciprofloxacin (78.5% vs. 66.7%; p=0.542) and clindamycin (83.9% vs. 61.9%; p=0.079) showed tendencies for more resistance in MRSA HCAP than in MRSA CAP. Resistance to rifampicin was observed only in MRSA HCAP, with an incidence of 2.7%, and the proportion of resistance to trimethoprim-sulfamethoxazole was also low in both groups (4.8% in MRSA CAP and 7.4% in MRSA HCAP; p=0.826). All patients showed sensitivity to vancomycin and linezolid. For vancomycin, the MIC was 2 µg/mL or less in both groups. For linezolid, the MIC was 2 µg/mL or less in all MRSA CAP cases, while 8.3% (3/36) of MRSA HCAP cases showed an MIC of 4 µg/mL or less.
DISCUSSION
We compared clinical characteristics, outcomes, and drug resistance patterns between MRSA CAP and MRSA HCAP from 2008 to 2011. Baseline characteristics, initial clinical manifestations, including radiological findings, disease severity, clinical outcomes, and medical expenses were similar between the groups. More patients with MRSA HCAP tended to show resistance to ciprofloxacin, clindamycin, and gentamicin. However, all MRSA isolates examined showed susceptibility to vancomycin and linezolid.
There are several reports on comparisons of CA-MRSA and HA-MRSA.22 However, there are few detailed reports about MRSA HCAP, because HCAP only recently became a defined group, since 2005, and is composed of heterogeneous patients with varying severities of illness and different reasons for contact with the healthcare environment. Previous studies have suggested that the characteristics of HCAP are more similar to those of HAP than CAP. Nevertheless, MRSA infection is frequently a fatal illness with high mortality, regardless of the origin of infection. Thus, we sought to compare the characteristics and clinical outcomes of MRSA CAP and MRSA HCAP.
In previous studies, incidences of MRSA HCAP and MRSA CAP have been reported up to 30.6% and 14.6%, respectively.3,4,5,19,23,24 While the incidence of MRSA HCA
P fluctuated from 7.6% to 19.4% over the 4 years in our study that of MRSA CAP increased since 2009, from 2.9% to 4.7%. Fluctuations in MRSA HCAP incidence were likely associated with local patterns of nosocomial pathogens during the period because most of the patients with HCAP had experienced repeated exposure to the hospital. The prevalence of MRSA CAP in 2008 was as high as 7.0% because the overall number of pneumonia cases with culture-positive pathogens was low due to relatively less effort being devoted to detecting atypical pathogens using serological tests. Thus, the relative proportion of MRSA was high, compared with other periods.
CA-MRSA pneumonia is associated with an influenza-like prodrome; severe respiratory symptoms with a rapidly progressive pneumonia, evolving to acute respiratory distress syndrome; high fever (body temperature ≥39℃); hemoptysis; hypotension; leucopenia; and a chest radiograph showing multilobar cavitating alveolar infiltrates.1,22 Young age has been a remarkable feature of CA-MRSA pneumonia in European and US studies.25,26,27 However, we demonstrated different features of MRSA CAP from previous studies. The ages of patients in the present study were not remarkably young, with an average in the 70 s, likely the result of population aging to the point where the level of immunocompromised subjects increased. Moreover, severe illness features of high fever and hemoptysis were not frequent, although hypotension was seen in about 40% of MRSA CAP cases. No patient with MRSA CAP showed cavitation on a chest X-ray.
MRSA HCAP in this study showed characteristics similar to the previously reported HA-MRSA pneumonia. The patients were elderly, with the average age in the 70 s, and half of the patients had significant underlying diseases, such as malignancies. Moreover, most of the MRSA isolates from HCAP showed resistance to multiple antibiotics.22
In this study, we compared MRSA CAP with MRSA HCAP. The average age was similar between the groups, with male dominance. Immunocompromised status and MRSA infection history for the previous year tended to be more common in MRSA HCAP than MRSA CAP. Pneumonia Severity Index scores were similar due to more severe clinical status in MRSA CAP and more severe underlying disease in MRSA HCAP, resulting in higher intubation rates and ICU admission for MRSA CAP than for MRSA HCAP. Although the proportion of requests for "do not resuscitate" was similar in both groups (33.3% in MRSA CAP and 40.0% in MRSA HCAP; data not shown), 28-day mortality tended to be higher in MRSA HCAP, probably as a result of severe underlying diseases. Both groups frequently showed multiple infiltrates but few cavitations on chest X-rays.
Comparing drug resistance patterns, MRSA HCAP showed more resistance to gentamicin than MRSA CAP. Although MRSA in all patients was sensitive to vancomycin and linezolid, the proportion of MICs of 1 µg/mL or less tended to be higher in MRSA CAP than in MRSA HCAP (83.4% vs. 71.4%).
HCAP is generally associated with higher mortality and higher healthcare costs than CAP, but MRSA infection did not show significant differences in clinical features and outcomes between HCAP and CAP.14,15,16,28 Total hospital charges were slightly higher for MRSA CAP than for MRSA HCAP, but the differences were not statistically significant. This might have resulted from more patients with MRSA CAP receiving aggressive treatment, including intensive critical care, versus those with MRSA HCAP.
The present study has several limitations. First, the definition of MRSA CAP in this study differs from that in several studies where CA-MRSA was restricted to only Panton-Valentine leukocidin (PVL)-positive S. aureus.1,22,25 Because of the retrospective method of this study, we were not able to analyze whether MRSA in CAP or HCAP produced PVL, which usually presents only in CA-MRSA. However, the purpose of this study was to compare the characteristics of MRSA CAP and MRSA HCAP, regardless of the presence of PVL. As the boundary between community and hospitals is blurring due to the back and forth movement of patients between them, the presence of PVL will not be limited to the community in the future. Moreover, a recent meta-analysis study reported that PVL genes were consistently associated with skin and soft-tissue infections, but were comparatively rare in pneumonia.29 Second, this study was conducted at a single tertiary referral hospital, so our findings may not generally represent MRSA CAP. Third, we included only patients with pneumonia that required hospitalization; they were older than the general population and had higher rates of comorbidities. Finally, the sample size was small despite a 4-year study period because of the relatively low incidence of MRSA CAP. Significant differences may be expected with increased numbers of cases.
In summary, our study presents a comparison of clinical characteristics, outcomes, and drug resistance patterns between MRSA CAP and MRSA HCAP from 2008 to 2011. The incidence of MRSA CAP has increased, unlike that of MRSA HCAP. Although HCAP should be generally distinguished from CAP because of differing clinical features, MRSA infection seems to have broken the boundary between HCAP and CAP, and the severe, infectious features that MRSA possesses may surpass the supposed differences in disease severity and characteristics between HCAP and CAP.



 XML Download
XML Download