

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Decreases in left atrial (LA) diameters and volumes after successful radiofrequency ablation (RFCA) for atrial fibrillation (AF) have been consistently reported in clinical studies.1,2,3,4,5,6,7,8,9 However, data on the changes in LA function after RFCA have shown conflicting results depending on the types of AF, follow-up period, and the imaging tools of analysis. Because patients with paroxysmal AF have relatively preserved LA function and volume before ablation as compared to patients with chronic AF, it is difficult to identify the subtle changes in LA function and reverse remodeling of LA volume after ablation.
Previous studies had limitations by the lack of follow-up data beyond 6 months,2,3,4,6,7,9 by study groups of less than 50 patients with paroxysmal AF,1,2,3,4,5,6,8 and by the simultaneous analysis of the data of patients with paroxysmal AF with those of patients with persistent AF.1,2,3,4,5,6,8
The purpose of this study was to evaluate the effects of RFCA in patients with paroxysmal AF on LA size, volume, and function at 3 months and at 1 year after ablation.
MATERIALS AND METHODS
Study population
Between March 2009 to May 2011, 105 consecutive patients were referred to our institution for RFCA due to symptomatic drug-refractory paroxysmal AF. Paroxysmal AF was defined as the occurrence of two or more episodes of AF during the previous year, all of which terminated spontaneously within one week. We excluded patients with a permanent pacemaker, more than a moderate degree of heart valve disease, a left ventricular (LV) ejection fraction (EF) of less than 50%, and those lacking sinus rhythm during initial echocardiogram to reduce the impact of other variables on LA function. Finally, 90 patients (65 men; age 57±13 years) with 29.9±4.4 months of mean AF duration were enrolled for RFCA. Echocardiograms of healthy volunteers matched for age and sex were also taken as a control group.
Protocol
Baseline echocardiographic examinations were performed in all patients on the day of or day prior to ablation. Anti-arrhythmic drugs were stopped at least five half-lives before RFCA to localize the arrhythmic triggers. The patients were followed-up at one week after ablation, and then at every 3 months with electrocardiogram (ECG) and 24-hour Holter monitoring. During the follow-up, medications such as anti-arrhythmics and warfarin were continued based on discretion of the physician. At 3 months and again at 1 year after the ablation, echocardiographic studies were done along with clinical histories and physical examinations. Recurrence of AF was defined as any atrial tachycardia lasting more than 30 seconds on 24-hour Holter monitoring or documented on 12 lead electrocardiograms after a three month blanket period. Patients were then divided into two groups on the basis of recurrence: maintained sinus rhythm (SR group) and recurrence of AF (AF group).
The Ethics Committee of our hospital approved the study (IRB number KC 12RISI0860). All patients gave informed consent to participate in the study and all clinical information was obtained from medical records.
Echocardiographic studies
Each patient underwent a complete standard echocardiographic study using a Vivid 7 apparatus (GE Medical systems, Milwaukee, WI, USA) with a 2.5-MHz phased array transducer, and electrocardiograms were analyzed offline using a customized software package (Echopac, GE Medical Systems, Milwaukee, WI, USA). An experienced observer who was blinded to the study performed all the echocardiograms, and a second blinded observer analyzed the parameters in offline mode. LV volume, LV mass index, and LVEF were measured as recommended by the American Society of Echocardiography (ASE) guidelines.10 LA anterior-posterior, superior-inferior, and medial-lateral diameters were measured on the parasternal long axis, the parasternal short axis, and the apical four-chamber views at end-systole, as based on the ASE guidelines.10 As described by the guidelines, LA maximal volume (LAVmax) was measured using Simpson's rule using the maximal LA volume between the apical four-chamber and apical two-chamber views at the end of ventricular systole and LA minimal volume (LAVmin) was measured at the end of ventricular diastole. LA ejection fraction (LAEF) was calculated as [LAVmax-LAVmin]/LAVmax, and the LA active emptying fraction (LAAEF) was calculated as [LA mid-diastolic volume at onset of the P wave on the surface electrogram (LAVmid)-LAVmin]/LAVmid.7 Transmitral [early (E), late (A)], and tissue Doppler myocardial velocity recordings [systolic (S'), diastolic early (E'), and late (A') velocities] from the septal and lateral mitral annulus were also obtained. The E/E' ratio was calculated, and the E-wave deceleration time (DT) was measured.
Electrophysiologic procedures
Two 7 Fr decapolar catheters (Woven; Bard Electrophysiology, Lowell, MA, USA) and one 5 Fr Nogami catheter (EP star His-RC Fixed; Japan Lifeline Co. Ltd., Tokyo, Japan) were positioned for pacing and recording in the coronary sinus, right atrium, and His bundle, respectively. Endocardial mapping was performed using a three-dimensional electroanatomic mapping system (CARTO, Biosense Webster, Diamond Bar, CA, USA). Intracardiac electrograms were obtained using a Prucka CardioLab™ Electrophysiology system (General Electric Medical Systems, Inc., Milwaukee, WI, USA). Pulmonary vein isolation was performed through the transeptal approach using a circular decapolar (Lasso; Biosense-Webster, Diamond Bar, CA, USA) catheter and ablated with a 4-mm open irrigated-tip catheter (20-30 mL/min; Navistar Thermocool, Johnson & Johnson, Inc., Diamond Bar, CA, USA). RF energy was delivered with a maximal temperature of 48℃, a maximum power of 35 W, and a maximum duration of 60 seconds per point. The procedural end-point was disconnection of all pulmonary veins (PVs). Additional lines consisting of LA roof and/or LA inferior ablation were performed in cases of persisting arrhythmia after electrical isolation of the PVs.
Statistical analysis
Continuous data are expressed as mean±SD. Categorical data are expressed as absolute numbers or percentages. Differences between the groups (control group, SR group, and AF group) were tested using unpaired Student's t-tests and chi-square tests. Differences between the echocardiographic data for each patient at different time points of assessment were examined with two-tailed paired Student's t-tests. The correlations between AF recurrence after RFCA and the predictors were assessed by multivariable logistic regression analysis. Multivariable analyses employed the forward stepwise method, with entry and removal probability values set at 0.5. A value of p<0.05 was considered statistically significant. A receiver operating characteristic analysis was performed to define cutoff values, and the cutoff values were defined by minimizing the expression of (1-sensitivity)2+(1-specificity)2. Data were analyzed using SPSS (version 12.0; SPSS Inc., Chicago, IL, USA).
RESULTS
Clinical characteristics
A total of 105 patients were treated with RFCA for AF. Fifteen patients were excluded, seven because of atrial fibrillation during echocardiogram, three because of permanent pacemakers, three because they had a LVEFs of lower than 50%, and two because they had more than a moderate degree of mitral stenosis. Finally, 90 patients (65 men; age 57±13 years) were included and completed an initial echocardiogram. The echocardiogram was followed-up with for 88 of the 90 patients (98%) at 3 months, and 78 of the 90 patients (87%) at 1 year. After 12±1 months, all 90 patients remained in follow-up. Among them, 61 patients were in sinus rhythm without any AF recurrence and 29 (32%) patients had AF recurrences. Patients with AF recurrences were treated with antiarrhythmic drugs (n=11), electrical cardioversion (n=9), another ablation (n=7), or a Maze operation (n=1).
The clinical characteristics of the patients in the SR and AF groups are listed in Table 1. The mean age was older in the AF group than in the SR group (61±10 years vs. 54±13 years, p<0.013). Both groups were well balanced with respect to their comorbidity, except for having a history of hypertension (HTN). Patients with a history of HTN were more frequent in the AF group as compared to the SR group (p=0.022). The number of patients using antiarrhythmic drugs before the RFCA was similar in both groups, but flecainide was the most commonly used medicine in the SR group, whereas propafenone was the most commonly used medicine in the AF group. The duration of AF was similar in both groups (29.9±39.5 months vs. 30.7±39.3 months, p<0.782).
Echocardiographic parameters
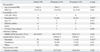
Before the RFCA, the mean LVEF was 62.3±6.4% and the mean E/E' was 9.8±5.3 without significant difference between the SR group and AF group, as summarized in Table 2. There were also no differences in LVEF or diastolic parameters (E/E', DT) between patients with paroxysmal AF and healthy volunteers. However, patients with paroxysmal AF had longer LA diameters, larger LA volume indices, and lower LA functions than those of healthy volunteers at baseline. The SR group had significantly shorter LA superior-inferior diameters, smaller LA volume indices, and higher LAEF and LAAEF than those of the AF group. Whereas initial E/E' had no difference between two groups, follow-up E/E' was significantly lower in the SR group than in the AF group (Table 3).
LA diameters
The LA diameters at baseline, 3 months, and 1 year of follow-up are listed in Fig. 1. There was no difference in baseline LA diameters and those at the 3 month follow-up. However, the LA anterior-posterior and superior-inferior diameters were significantly decreased after 1 year. When reviewed on the basis of AF recurrence, decreases in all three LA diameters after 1 year remained significant in the SR group but only decreases in the LA superior-inferior diameter were significant in the AF group.
Initially, the LA anterior-posterior and medial-lateral diameters of the AF group were similar to those of SR group, but were significantly longer 3 months after RFCA. The difference was maintained at the 1 year follow-up only in the LA medial-lateral diameter. In terms of the LA superior-inferior diameters, there was an initial difference between the SR group and the AF group, and this difference was maintained for 1 year.
LA volumes
The LA volumes at baseline and the three month and 1 year follow-ups are listed in Fig. 2. After 3 months, the LAVmax indices decreased (from 33±13 to 28±12 mL/m2; p<0.001). The LA mid-diastolic volume indices decreased at 1 year (from 23±11 to 20±13 mL/m2; p=0.002), but the LAVmin indices remained unchanged. However, when reviewed on the basis of AF recurrence, the LA mid-diastolic volume indices were only decreased in the AF group after 3 months (30±12 to 25±12 mL/m2; p=0.034), but were not decreased in the SR group until the 1 year follow-up.
The initial left atrial volume index (LAVI) of the AF group was significantly larger than that of the SR group, and remained larger throughout follow-up, though the LA mid-diastolic volume indices after 1 year only showed a difference in trend, though without statistical significance.
LA function
LA function at baseline and at 3 months and 1 year of follow-up are listed in Fig. 3. LAEF and LAAEF were decreased at 3 months follow-up (from 48±13 to 39±12; p<0.001, from 27±13 to 19±11; p<0.001), and remained similar at 1 year. When reviewed on the basis of AF recurrence, the initial LA function of the SR group was superior to that of the AF group, but they were similar at 3 months. At the 1 year follow-up, the LA function of the SR group was again better than that of the AF group (LAEF 44±13 vs. 34±1, p=0.001; LAAEF 22±11 vs. 14±10, p=0.011).
As compared to the SR group, the LA function of the AF group showed a consistent decreasing trend at both the short-term and long-term follow-up visits, whereas the LA function of the SR group had a trend of recovery at the 1-year follow-up, but was still decreased compared to initial values.
LA volumes and LA function and predicting AF recurrence
The results of the logistic regression analysis of AF recurrence are summarized in Table 4. Univariate analysis showed that being more than 75 years old (p=0.017), having a history of HTN (p=0.021), LAEF (p=0.007), and LAVmax (p=0.001) were associated with AF recurrence. Multivariate analysis identified LAVmax as an independent predictor of AF recurrence (odds ratio 1.037, 95% confidence interval 1.008 to 1.066; p=0.010). When the cutoff value was LAVmax=49.4 mL, the sensitivity of a large LAVmax (>49 mL) for predicting AF recurrence was 89.3% in 26 of 29 patients with AF recurrence and the specificity was 56.7% in 35 of 61 patients. The area under the curve for the prediction of AF recurrence was 0.745 for LAVmax.
DISCUSSION
The main findings of this study are that: 1) successful RFCA in patients with paroxysmal AF decreased LAVmax and function in the short-term and showed a trend of recovery of LA function in the long term, whereas the patients with recurrence of AF had worse LA function; 2) patients with recurrent AF had significantly larger LA volumes than patients without recurrent AF; and 3) the LAVmax RFCA was an independent predictor of AF recurrence after ablation.
LA diameters
In this study, the LA anterior-posterior and superior-inferior diameter was decreased at 1 year, whereas the LA medial-lateral diameter showed no change. A recent meta-analysis showed significant decreases in LA diameter at follow-up imaging ≥1 month after RFCA.7 However, a recent study in patients with paroxysmal AF by two-dimensional echocardiography with a follow-up time of 8±2 months and a study using three-dimensional echocardiography after 6 months of follow-up9 both showed no change in LA diameter after ablation.2 The above three studies used LA anterior-posterior diameters in their analyses. Although LA anterior-posterior diameters represent linear LA measurements, this is often an inaccurate depiction of true LA size. Sometimes the relationships between LA anterior-posterior diameter and other diameters are not consistent because expansion of the LA in the anterior-posterior (AP) direction may be constrained by the thoracic cavity between the sternum and the spine.10 Predominant enlargement in the superior-inferior and medial-lateral diameters will alter LA geometry such that the AP dimension may not be representative of the true LA size. This may explain why our LA diameters showed different results by different diameters.
LA volumes
In the present study, LAVImax and LAVImid decreased after the ablation, but LAVImin did not. The changes were identified in both the SR group and the AF group, but the LAVI of the SR group was smaller than that of the AF group. Previous studies demonstrated reverse morphological remodeling of the LA by ablation for isolated AF by two-dimensional echocardiogram.2,6 Recently, RFCA was found to induce a reduction in LAVmax by three-dimensional echocardiography. The same phenomenon has been patients with repeated RFCAs.
It has been proposed that reduced LA size after AF ablation could be secondary to reverse remodeling due to the elimination of the arrhythmia (i.e., only responders would remodel) or because of scarring induced by the radiofrequency lesion (i.e., all patients would remodel).9,11 Recent studies of LA scars induced by RFCA as assessed by cardiac magnetic resonance imaging (MRI) and by a time course of markers of tissue repair after RFCA (matrix metalloproteinase-9 and transforming growth factor-β1) support reduction of LA volume by scarring, which would support the latter opinion.12,13 Our results, which identified reductions in LA volume in both the SR group and the AF group, favor the theory of scarring by RFCA.
However, continuing differences in LA volume between the two groups after RFCA implies the importance of positive remodeling by reducing AF burden. Therefore, the reduction of LA volume observed in both groups may be because scarring by RFCA outweighs the effects of positive remodeling by restoring sinus rhythm in patients with only paroxysmal atrial fibrillation due to the presence of relatively lower AF burden than in patients with persistent AF.
LA function
In our study, LAEF and LAAEF remained decreased until 1 year after RFCA. However, there have been conflicting results regarding atrial function after catheter ablation of AF depending on imaging modality, follow-up period, and the type of AF. Choi, et al.3 reported recovery of LAEF and A velocity at 3 months after ablation, but Rodrigues, et al.6 reported decreases in LAEF at more than 6 months after RFCA by two-dimensional echocardiography. Montserrat, et al.9 reported preserved LAEF and LAAEF even after repeated ablation by three-dimensional echocardiography at 6 months after the ablation. Donal, et al.14 noted decreased LA compliance after 1 year of RFCA by LA strain. Wylie, et al.12 reported reduced atrial systolic function correlated with LA scars at a mean of 48 days by cardiac MRI. Masuda, et al.15 demonstrated that AF ablation appears to have a beneficial effect on LA function, as assessed by cardiac CT at 3 months after RFCA.
The left atrium has three functions: acting as a contractile pump that provides up to 1/3 of the left ventricular volume, as a reservoir that collects pulmonary venous return during ventricular systole, and as a conduit for the passage of stored blood from the LA to the LV just after the isovolumetric relaxation phase of ventricular diastole, when the mitral valve opens.11 LAEF reflects LA conduit and contractile function and LAAEF shows only contractile function. In contrast to other reports, the LAEF and LAAEF of the SR group were significantly decreased at 3 months after the RFCA, but not in the AF group in our study. We hypothesized that the cause of significant decreases of LA function in the SR group was because of the differential changes between LAVmax and LAVmin. While the LAVmax of both groups changed significantly in serial follow-ups, LAVmin remained unchanged. In addition, the range of the decreases in LAVmid and LAVmax were larger in the AF group than in the SR group. We believe that these changes in LA volumes resulted in significant decreases in LA function in the SR group at the 3 month follow-up due to the formulae of LAEF and LAAEF.
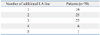
One of the most persuasive studies done with MRI showed improved LAEF in patients without recurrence and no change in those with recurrence.16 The method of ablation in the study was only 4 pulmonary vein isolation, whereas we conducted additional LA ablations (anterior, roof, posterior, perimitral and septal line) in most of our patients (Table 5). The additional LA ablation may affect the deterioration of LA function whereas pulmonary vein isolation was not.
Study limitation
Our study was a retrospective echocardiographic evaluation of reverse LA remodeling after RFCA of AF, including morphological and functional changes in the LA only in patients with paroxysmal AF. Major limitations of this study are the small sample size, the low recurrence rate, and the relatively wide range of the odds ratios in the multiple logistic regression analysis. In addition, echocardiography has limitations in terms of poor acoustic windows and may underestimate true LA size and volume compared to computed tomography or MRI.7
In addition, the different kinds of antiarrhythmic drugs being taken by the patients may have influenced the results. These drugs may assist in maintaining sinus rhythm and latently improve the LA function seen during follow-up. Different ablation lesions targeting the additional LA lines and variation in the duration of RFCA may all affect the recurrence of AF. Due to the above limitations and growing concern about AF recurrence after RFCA, a large cohort study is needed in the future.
Conclusion and clinical implications
Successful RFCA in patients with paroxysmal AF significantly decreases LAVmax and function shortly after ablation and improves LA function gradually with time. Patients with recurrent AF had significantly larger LA volumes than patients with SR. LAVmax before RFCA was an independent predictor of AF recurrence after the ablation.
Because delayed functional improvements could cause thromboembolism and other cardiovascular events, careful anticoagulation during prolonged follow-up is warranted, but this potential management approach requires further study. In addition, the assessment of LA using new echocardiographic parameters such as LA strain, three-dimensional LA volume, and CT or MRI may lead to more accurate assessments in patients with AF.






 XML Download
XML Download