

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Insulin is a hormone that plays an essential role in the maintenance of homeostasis between glucose uptake and production.1 Insulin resistance is defined by a state of reduced reactivity to insulin in target tissues such as liver, muscle, and adipose tissue, and is known to be a major factor in various physiological dysfunctions such as metabolic syndrome (obesity, hyperlipidaemia, hypertension, and glucose intolerance).1,2 Insulin resistance and metabolic syndrome are the most important risk factors for type 2 diabetes mellitus in Western populations. Korean patients with type 2 diabetes mellitus show different clinical characteristics from those in the West because of racial characteristics, dietary habits, and lifestyle. In Korea, however, the number of patients with type 2 diabetes mellitus who have insulin resistance associated with metabolic syndrome has increased.3 We recently showed that insulin resistance is independently associated with peripheral neuropathy in Koreans with type 2 diabetes mellitus regardless of blood glucose level.4
Conventional electrophysiological studies are widely used for the objective diagnosis of diabetic neuropathy. The physiological function of nerves can be evaluated quantitatively by nerve conduction study (NCS).5,6 NCS abnormalities occur early in the course of type 2 diabetes mellitus, and the pattern of progression of peripheral neuropathy shows dependence on the length of the nerve fibers.7 NCS shows complicated abnormalities of sensory, motor, and autonomic nervous systems.8 In addition, NCS shows mildly slow nerve conduction velocity and low amplitude in diabetic polyneuropathy, suggesting that the peripheral neuropathy of type 2 diabetes mellitus is primarily caused by axonal degeneration.9,10
Because type 2 diabetes mellitus is a chronic disease, the management of complications such as neuropathy is important in terms of quality of life. However, a diagnosis of diabetic neuropathy can be difficult to make, when based only on clinical characteristics. Patients do not express symptoms in the course of mild neuropathy, and it is very difficult to identify subclinical diabetic neuropathy without performing procedures such as NCS.11 Moreover, in the early stage of diabetic neuropathy, NCS can only detect the most distal sensory nerves, such as medial-plantar and dorsal sural nerves, which are not usually included in routine nerve conduction studies.12
The purpose of this study is to determine whether insulin resistance is associated with the development and progression of neuropathy in patients with type 2 diabetes mellitus. We previously demonstrated that insulin resistance is independently associated with peripheral neuropathy in Korean patients with type 2 diabetes mellitus.4 In this study, we analysed the follow-up results of blood tests and electrophysiological examinations, conducted 6 years previously, for the screening of diabetic neuropathy.
MATERIALS AND METHODS
Patients
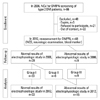
This study involved 48 of the original 86 Korean patients with type 2 diabetes mellitus who were referred from the diabetes mellitus clinic at Gangnam Severance Hospital, Seoul, Korea, to the neurology outpatient clinic for the assessment of diabetic neuropathy from January 2006 to December 2006. These 48 patients received management for glycaemic control and prevention of diabetic complications in the outpatient clinic up to 2012 (Fig. 1). We reviewed blood test results and the nerve conduction study findings of these patients, taken over a 6-year period. Subjects included those with symptomatic neuropathy as well as asymptomatic patients who had been referred for screening purposes. The diagnosis was based on a previous history of diabetes mellitus or using the American Diabetes Association's diagnostic guidelines.13 Exclusion criteria were as follows: type 1 diabetes mellitus, severe liver dysfunction (alanine aminotransferase or aspartate aminotransferase more than 2 times the upper limit of normal values), severe renal dysfunction (serum creatinine >1.6 mg/dL), current smoker, uncontrolled hypertension, recent infection history, malignancy, loss of dorsalis pedis arterial pulsation, and previous history of neurologic disorders including stroke, peripheral vascular occlusive disease, autoimmune disease, or any other possible causes of peripheral neuropathy.
This study was approved by the human research ethical committee at Yonsei University College of Medicine, Seoul, Korea (No.3-2013-0006).
Analytical methods
All patients had height and weight measured for body mass index (BMI) determination, and the following tests were performed upon enrolment in the study.
Diagnosis of peripheral neuropathy
The diagnosis of peripheral neuropathy was made in two stages: objective neurologic exams and electrophysiologic studies, with slight modifications from the Michigan Diabetic Neuropathy Score.11,14
For neurologic examinations, each patient was assessed for sensitivity, muscle strength, and reflexes of the bilateral upper and lower extremities and scored accordingly.11 Vibratory sensitivity was evaluated using a 128-Hz tuning fork and touch sensitivity with a 10 g monofilament. Muscle strength was assessed by abduction of the fingers, extension of the great toe, and the ankle dorsiflexion. In addition, reflexes of upper and lower limbs were evaluated.
NCS were performed using electromyography (Keypoint, Dantec Medical, Skovlunde, Denmark). Skin temperature was measured at the forearm and was maintained at >32℃. Motor and sensory nerve conduction velocities were measured in median, ulnar, peroneal, posterior tibial, and sural nerves using standard methods. Electrical stimuli were produced at supramaximal intensity. Sensory nerve conduction was measured using a 0.2-ms duration square wave pulse, 20-2000 Hz filter, 1 ms/division sweep speed, and 10 µV/division sensitivity. Motor nerve conduction studies were performed using 2-10000 Hz filter, 2 ms/division sweep speed, and 2 mV/division sensitivity. NCS values lower than the 95th percentile of the normal control values were considered abnormal.
The diagnosis of peripheral neuropathy was made when the clinical score was greater than 6 and/or in the presence of at least two abnormal results in NCS, amplitudes, or peak latencies.11,14 A reduction in motor or sensory NCS in two or more nerves independent of the clinical scores was considered sufficient for diagnosis, whereas patients with only one abnormal nerve conduction parameter were not considered affected by neuropathy.11 In the absence of a response, the contralateral nerve was assessed.14
Insulin resistance
Serum insulin resistance was measured using a short insulin tolerance test and estimated by the Kitt index as previously described.15 On the morning of the test day after more than 10 h of fasting, a 20-gauge catheter was inserted into one arm, a 3-way tap was connected, and blood was obtained. A second 20-gauge catheter was inserted for insulin and glucose infusion. After insertion of the second catheter, patients were allowed to rest in the supine position for 20-30 min. A 1:100 dilution of insulin (insulin lispro, 0.1 u/kg) was then injected. Blood was obtained through the 3-way tap just prior to injection (0 min) and at 3, 6, 9, 12, and 15 min after injection and was stored in a tube with ethylenediaminetetraacetic acid. Serum glucose was measured, and the Kitt value was obtained by linear regression analysis of the decrease in the log glucose value between 3 and 15 min as follows:
where t1/2 is the time at which the baseline blood glucose level reached 50% of its initial value.
Peripheral blood markers
All blood sampling was performed in the early morning after fasting since midnight. Plasma glucose was measured by the glucose oxidase technique using an auto-analyser (Beckman, Fullerton, CA, USA). HbA1c was analysed using high-performance liquid chromatography (Variant II, Bio-Rad, Hercules, CA, USA). Insulin and C-peptides (fasting and postprandial) were measured using radioimmunoassay (Instar, Stillwater, MN, USA).
The glycaemic exposure (GE) Index was calculated using the following equation:16
Statistical analysis
Continuous variables are given as means with standard deviation, and categorical variables are given as frequencies and percentages. Univariate analysis was initially performed to evaluate potential covariates associated with the development of neuropathy. Multivariate analysis using binary logistic regression was then used for determination of independent predictors of the presence of peripheral neuropathy. A p-value less than 0.05 was considered statistically significant. A general linear model was used to analyse the variability of NCS data between 2006 and 2012. The Kruskal-Wallis test was used as a non-parametric test for comparisons between the three groups that were classified by the results of NCS.
Statistical analysis was performed using SPSS version 18.0 (Statistical Package for Social Sciences, SPSS Inc., Chicago, IL, USA).
RESULTS
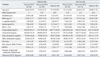
Among 86 patients, 40 (46.5%) were diagnosed with peripheral neuropathy in 2006.4 According to the results of our 2006 study, insulin resistance (1/Kitt value), GE Index, duration of diabetes mellitus, and HDL cholesterol level were significantly different between the peripheral neuropathy group and non-neuropathy group. In 2012, we repeated NCS and blood sampling in 48 of the original 86 patients. In 33 patients, the results of NCS and neurologic examination were normal in both 2006 and 2012, and 6 patients who had normal results in 2006 were diagnosed with peripheral neuropathy in 2012. The remaining 9 patients had peripheral neuropathy already in 2006. The clinical characteristics of the patients are presented in Table 1.
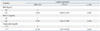
In univariate logistic regression analysis, higher BMI, lower high-density lipoprotein (HDL) cholesterol, and higher triglyceride levels were related to the presence of peripheral neuropathy (Table 2). However, gender, age, C-peptide, insulin, HbA1c, cholesterol, DM duration, GE Index and number of abnormal autonomic function test were not correlated with peripheral neuropathy. In multivariate analysis using binary logistic regression, high triglyceride and low HDL cholesterol were significantly associated with peripheral neuropathy after adjusting for age and gender (Table 3). As in 2006, lower HDL cholesterol in 2012 increased the odds ratio for peripheral neuropathy.
We selected patients with a mean HbA1c <7% and good blood glucose control from 2006 to 2012. Among these patients, a lower Kitt value in 2006 was related to the occurrence of peripheral neuropathy in 2012 (Table 4).
The patients were divided into three groups according to the follow-up NCS results in 2012. In group I patients (n=33), NCS results were normal in 2006 and 2012. In group II patients (n=6), NCS results were normal in 2006, but abnormal at the follow-up NCS in 2012. Group III patients (n=9) had already been diagnosed with diabetic neuropathy by NCS in 2006.
The Kitt value reflects insulin resistance: the lower the Kitt value, the higher the insulin resistance. The Kitt value of these three groups was significantly different (Kruskal-Wallis test, p=0.004). In post-hoc analysis, a significant difference in Kitt value was observed between groups I and II (Dunn's procedure, p=0.046) and between groups I and III (Dunn's procedure, p=0.025). There was no significant difference in Kitt value between groups II and III (Fig. 2).
We compared the follow-up NCS results and the data from 2006 for each group. In group I, there was no difference between the 2006 and 2012 results. In groups II and III, sural sensory nerve conduction velocity and sensory nerve action potential (SNAP) amplitude were reduced in 2012 compared with the 2006 results, but there were no significant differences in the other parameters of NCS, such as median, ulnar, and tibial nerve conduction.
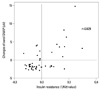
Insulin resistance in 2006 showed a positive correlation (r=0.629, p=0.001) with differences in sural SNAP in group III between 2006 and 2012 after adjusting for age, gender, and height (Fig. 3).
DISCUSSION
In addition to clearly symptomatic diabetic neuropathy patients, asymptomatic patients also often undergo mild neuropathic changes.17 Follow-up NCS should therefore be considered in patients with diabetes mellitus in the absence of overt symptoms of neuropathy.11 Such studies also allow physicians to determine the extent of deterioration due to diabetic neuropathy in patients with very mild symptoms. In this study, we investigated the risk factors for the development of diabetic neuropathy in type 2 diabetes mellitus over a 6-year follow-up period. Our earlier findings showed that insulin resistance and lower HDL cholesterol are associated with diabetic neuropathy. Here, we investigated the relationship between insulin resistance in the past and the later occurrence of neuropathy.
Over the past decade, mitochondrial dysfunction has been shown to play a key role in the pathologic features of insulin resistance.18 Mitochondrial fission in both cell bodies and neurites increase during hyperglycaemic injury in dorsal root ganglia and axons.19 Excessive mitochondrial fission may result in dysregulation of energy production, activation of caspase-3, and subsequent dorsal root ganglion neuron injury.19,20 Similar to other peripheral tissues, the expression of the insulin receptor protein on ganglion cells is altered by hyperglycaemia and consequent activation of downstream insulin receptor signalling contributes to the onset of diabetic neuropathy in animal models.20 In addition, hyperlipidaemia causes an increase in oxidized lipoproteins, and lipoprotein receptors on the dorsal root ganglia cause oxidative stress, which induces neuropathy.21 Several studies have provided strong evidence that dyslipidaemia contributes to macro and microvascular complications, and lipid control is a new therapeutic target in type 2 diabetes mellitus.22,23
HbA1c values reflect overall glycaemic exposure over the prior 2-3 months.24,25 The American Diabetes Association-recommended treatment goal to prevent microvascular complications in type 2 diabetes mellitus patients is HbA1c <7%, which is considered the standard for the monitoring of glycaemic control.26,27 Recent studies have shown that high HbA1c is correlated with subclinical diabetic neuropathy.28 However, these studies are likely limited, because the authors did not control the effects of other risk factors such as obesity or dyslipidaemia. Obesity, dyslipidaemia, and impaired insulin tolerance are components of metabolic syndrome that may potentially influence the occurrence of idiopathic neuropathy.29 Therefore, without controlling metabolic risk factors, it may be incorrect to conclude that only glycaemic control affects the development of diabetic neuropathy.
In this study, multivariate analysis showed that patient gender, age, and obesity were not independent risk factors for diabetic neuropathy. However, as in our previous study, low HDL cholesterol showed a strong association with neuropathy, indicateing that the management of dyslipidaemia in patients with type 2 diabetes mellitus is important for the prevention of neuropathy. Microvascular events caused by dyslipidaemia seem to have a lasting impact, even after several years. However, there was no relationship between dyslipidaemia and neuropathy in patients with HbA1c levels <7%.
Our study showed no difference in insulin resistance between groups II and III; however, there were significant differences when comparing groups I and II as well as groups I and III. This indicates that past insulin resistance contributes to the expression of neuropathy after many years. In particular, we found a relationship between low Kitt value in the past and worsened NCS data in the current study, even in patients with good glycaemic control and mean HbA1c <7% over the past 6 years. Therefore, past insulin resistance affects the onset of neuropathy many years later, even if glycaemic control is well managed.
The group III patients already had neuropathy in the previous study. We found that the changes in SNAP in this group between 2006 and 2012 showed a positive correlation with past insulin resistance after adjusting for age and height. Higher insulin resistance in the past can therefore accelerate the deterioration associated with the process of neuropathy in type 2 diabetes mellitus. A decrease in SNAP, compared with past NCS data indicates the progression of neuropathy, even in mildly symptomatic or asymptomatic patients.
The current study has several limitations. First, as in our previous study, this study was conducted only on patients with type 2 diabetes mellitus. Comparison of our results with data for a normal control group would provide more comprehensive results. Second, the gender distribution of our data was not even, and there were many more males than females. Many reports have shown that males are more vulnerable to neuropathy than females;30,31 therefore, this gender bias should be considered when interpreting the results. Third, the Kitt value reflects insulin resistance, as assessed by a short insulin tolerance test instead of the euglycaemic hyperinsulinaemic clamp test. In addition, we could not test the Kitt value in this follow-up study. Insulin tolerance test must be performed in monitoring room because of unexpected low glucose level. Thus, Kitt value is not necessary test for common follow-up patients. We designed this study retrospectively, so that the Kitt value is not checked again. Nevertheless, the values of repeated measurements of insulin intolerance test may allow us to explain the relationship between insulin resistance and diabetic neuropathy. Fourth, small number of patients could not show powerful results in statistical analysis. We added dunn's procedure to calibrate the results of Kruskal-Wallis test.
In conclusion, insulin resistance seems to be associated with peripheral neuropathy, independent of blood glucose level, in Korean patients with type 2 diabetes mellitus, and diabetic neuropathy can be affected by previous insulin resistance in spite of regular glycaemic control. In addition, dyslipidaemia should be controlled in patients who have shown high insulin resistance in the past, because HDL cholesterol and triglyceride levels are strongly correlated with diabetic neuropathy. Physicians should consider regular follow-up electrophysiologic tests in patients with type 2 diabetes mellitus who have no neuropathic symptoms, even if they are normal on NCS.



 XML Download
XML Download