

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Timely reperfusion of jeopardized myocardium is the most effective way of restoring left ventricular systolic function and reducing infarct size, thereby reducing the morbidity and mortality associated with ST-elevation myocardial infarction (STEMI). Microvascular obstruction (MVO) or no-reflow phenomenon refers to a state of poor myocardial perfusion at the microvascular level despite successful restoration of the patency of the epicardial coronary artery.1,2,3 Ischemia itself, reperfusion injury, inflammation, or distal embolization of a thrombus and/or plaque debris can cause development of MVO during primary percutaneous coronary intervention (PCI) for STEMI.1,2,3,4,5 Poor myocardial perfusion is associated with a higher occurrence of extensive infarction, left ventricular remodeling, and increased mortality than good myocardial perfusion.6,7,8 Thus, in the treatment of STEMI, attaining adequate myocardial perfusion is as important as achieving fast epicardial blood flow.
Many studies have assessed the effect of interventional treatments, such as aspiration thrombectomy (AT)9,10,11,12,13 or glycoprotein (Gp) IIb-IIIa inhibitors,14,15,16 on the improvement of myocardial perfusion, which would thereby decrease infarct size in patients with STEMI. It can be hypothesized that combination of abciximab and AT might synergistically improve myocardial perfusion. Thus far, there are limited data about the benefits of combination treatment with intracoronary (IC) abciximab and AT as adjuncts to primary PCI for STEMI.16,17
MVO, visualized by cardiac magnetic resonance imaging (CMR), has been increasingly reported as a useful prognostic indicator in STEMI.18,19 Fearon, et al.20,21 reported that the index of microcirculatory resistance (IMR) can be a novel prognosticator for left ventricular remodeling and mortality in patients with STEMI. An elevated IMR was also linked to MVO as revealed by CMR in patients with STEMI.22 Therefore, we sought to examine whether a combination of IC abciximab and AT is superior to each treatment alone in terms of improving myocardial perfusion, as assessed by IMR and MVO on CMR.
MATERIALS AND METHODS
Study population
We screened 256 consecutive patients between at least 18 years of age and less than 70 years of age with de novo STEMI, who presented within 6 h of symptoms onset and underwent primary PCI at our hospital between December 2010 and February 2012. Sixty-four patients having Killip ≥3, 18 with hemodynamic instability requiring hemodynamic support devices, and 90 who had preprocedural Thrombolysis in MI (TIMI) flow grade ≥2 or thrombus grade ≤2 were excluded. Twenty-six subjects refused to participate in this study. Other exclusion criteria were contraindications for CMR, atrial fibrillation, chronic kidney disease (Cr ≥3 mg/dL), neoplastic disease, platelet count <150000/mL, and hemoglobin <10 g/L. Angiographic inclusion criterion was preprocedural TIMI flow grade 0/1 or evidence of thrombus grade 3/4. In addition, the target lesion should be located in a native coronary artery in the proximal to mid segment with an estimated reference diameter of ≥2.25 mm and ≤4.25 mm. IC thrombus was scored in 5 grades as previously described.23 The final study cohort comprised 40 subjects, divided into 3 groups before primary PCI, according to a random-number table: 10 patients, who received only a bolus of IC abciximab (0.25 mg/kg), 10 patients, only AT, and 20 patients, both treatments (Fig. 1). Our study protocol was approved by the Ethical Review Board of Yonsei University Wonju College of Medicine (Wonju, Korea). Informed consent to participate in this study was obtained from all the patients.
Coronary angiography and antithrombotic regimens
All patients received aspirin (300 mg) and clopidogrel (300-600 mg) immediately after STEMI diagnosis by electrocardiogram (ECG). Aspirin (100 mg) and clopidogrel (75 mg) were administered for ≥12 months after PCI. After an intravenous (IV) bolus injection of unfractionated heparin (70 U/kg), IV infusion (1000 U/h) was continued, and, if necessary, additional boluses were administered to achieve an activated clotting time of 300 s. After passing through the lesion with a 0.014-inch guidewire, AT was performed before balloon predilation. Then, a bolus of IC abciximab (0.25 mg/kg) was administered via the guiding catheter when the distal epicardial coronary flow was visible. The systemic IV infusion of abciximab was not permitted. Either one of IC abciximab or AT was omitted in 20 patients not allocated to the combination group. Stenting of the infarct-related artery was performed in all patients. Direct stenting, the type of stent, and post-stent adjuvant ballooning were at the discretion of the treating physician. Both TIMI flow24 and myocardial blush6 were graded on the coronary angiogram as described previously. The duration of cine filming was prolonged by at least 3 cardiac cycles to make sure that the entire washout phase was included. Myocardial blush grade (MBG) was assessed during the same phase of the cardiac cycle. MBG and other quantitative coronary angiography parameters were measured and analyzed off-line using a primary diagnostic image review and analysis workstation (Centricity Cardiology CA 1000, Milwaukee, WI, USA) by an interventional cardiologist who was incognizant of the clinical information including the IMR result.
Measurement of IMR
After successful primary stenting, a calibrated coronary pressure wire (St. Jude Medical, Minneapolis, MN, USA) was equalized to the guiding catheter pressure with the sensor positioned at the ostium of the guiding catheter, and then advanced beyond the culprit lesion. All pressure tracings were recorded on the RadiAnalyzer Xpress (St. Jude Medical) for offline analysis. Coronary wedge pressure was measured after 30 s of balloon occlusion within the stented segment. The IMR [mm Hg.s, or units (U)] was defined as simultaneously measured distal coronary pressure divided by the inverse of the thermodilution-derived hyperemic mean transit time (hTmn) (Fig. 2A). The mean transit time at rest and during hyperemia was measured by the methods described previously.25 The shaft of the pressure wire can act as a proximal thermistor by detecting changes in the temperature-dependent electrical resistance. The sensor near the tip of the wire simultaneously measures pressure and temperature, thereby acting as a distal thermistor. The transit time of room temperature saline injected into a coronary artery can be determined using a thermodilution technique. Three injections of saline (3 mL, room temperature) were administered to the coronary artery, and the baseline mean transit time was measured. Pharmacologic hyperemia was then induced by an IV infusion of adenosine at 140 µg/kg/min; 3 more injections of saline (3 mL, room temperature) were administered, and the hTmn was measured.
CMR protocol and analysis
CMR was performed on day 5 (median 5, range 3-9) using a 3-T magnetic resonance imaging system (Achieva Release 2.1; Philips, Eindhoven, the Netherlands), equipped with a dedicated cardiac software package, cardiac coil, and vectorcardiogram. Following the acquisition of localizing images, we obtained long- and short-axis cine images using a retrospectively gated breath-hold true fast imaging with steady-state free precession technique. The short-axis cine scans of 10-mm slices were used to determine the left ventricular mass, volume, and function. A bolus of contrast medium, gadolinium-diethylenetriamine pentaacetic acid was injected at a dose of 0.1 mmol/kg, and images were acquired for 60 heartbeats immediately following contrast infusion. Delayed enhancement images were then obtained by acquiring an inversion-recovery segmented gradient echo T1-weighted sequence 10-15 min after the bolus. All post-processing and analyses of the left ventricular mass, volume, function, myocardial infarct size, and presence of MVO were performed using the Extended Brilliance Workstation (Philips, Eindhoven, the Netherlands) by a radiologist who experienced in CMR and was blind to all clinical and pressure wire data. Infarct size was assessed manually by planimetry on each short-axis slice, delineating the hyperenhanced area, including areas of hypoenhancement surrounded by the hyperenhanced area-the latter was considered as MVO (Fig. 2B). Transmurality was calculated as the average transmurality of all segments with evidence of infarction in a 17-segment model.26,27 Infarct size was determined as a percentage of left ventricular mass as the sum of hyperenhanced pixels from each of the 6-8 short-axis images divided by the total number of pixels within the left ventricular myocardium multiplied by 100%.28
Main outcome measures
The primary endpoint was the IMR value for each group. The secondary endpoints were the presence of MVO on CMR, MBG on final coronary angiogram after successful coronary stenting and ST-segment resolution on ECG at 90 min after PCI. The occurrence of the composite of death from cardiovascular causes or non-fatal reinfarction at 1 month was also compared.
Statistical analyses
We hypothesized that combination treatment using a bolus of IC abciximab and AT would be superior to each treatment alone regarding post-PCI myocardial perfusion as assessed by IMR. On the basis of results from the previous studies,20,22,29 we assumed the mean value of IMR of either the IC abciximab or the AT group to be approximately 34±14 U. Upon a superiority design, total 40 patients were needed to ensure a power of 80% to detect a 14 U decrease of IMR using a 2-tailed test, with a sample ratio of IC abciximab:AT: both at 1:1:2, bilateral risk at 5%, and the estimated dropout rate of 10%. Continuous variables are presented as mean±SD or median (range) and categorical variables as frequencies (percentages). The analysis of variance or Kruskal-Wallis test was used for comparing continuous variables. Post-hoc analysis was performed for the parameters found to be significant by analysis of variance. The chi-square test or Fisher's exact test was used for categorical variables. Pairwise p values from the chi-square tests were presented with a Bonferroni correction for multiple tests. The univariate logistic regression analyses were done to investigate the relation of IMR [>34 U (upper tertile); dependent variable] to clinical and laboratory variables, echocardiographic and angiographic parameters, and CMR parameters. Multiple logistic regression analysis was performed to assess the correlates of IMR from variables on the basis of the best results of the univariate regression analyses at the significance level of p<0.1. IMR was compared according to the presence of MVO, ST-segment resolution, or MBG using the unpaired t-test. All analyses were carried out with SPSS version 20.0 (SPSS inc., Chicago, IL, USA). A two-sided p value <0.05 was regarded statistically significant.
RESULTS
Baseline characteristics
Baseline clinical and laboratory characteristics on the basis of treatment modalities are presented in Table 1. Mean age, diabetes mellitus history, hypertension, hyperlipidemia, and current smoking status were balanced between the groups. Most subjects (82.5%) were male. The AT group had lower body mass index as compared with the IC abciximab group (22.6±2.5 vs. 26.9±3.2, p=0.006). The distribution of dis charge medication use, including dual antiplatelet therapy, β-blocker, angiotensin converting enzyme inhibitor or angiotensin receptor blocker, or statin, was similar between the 3 groups. Ischemic times tended to be shorter in the combination group than in the other groups (p=0.053). No significant difference was observed in the frequency of anterior wall MI, Killip classification, left ventricular ejection fraction, B-type natriuretic peptide, peak creatine kinase, muscle and brain, or peak troponin I.
Coronary angiography and PCI data
Table 2 depicts the coronary angiography and PCI data. Approximately 75% of the patients underwent primary PCI for a coronary lesion in the left anterior descending artery. Most lesions had TIMI flow grade 0/1 (90%), collateral flow grade 0/1 (92.5%), and large thrombotic burden (80%), without significant differences between the groups. White or red thrombi were retrieved in 95% of the patients who were treated with AT. All PCI was attempted only for a culprit vessel. No difference regarding stent number per patient was observed. Two patients in the combination group had multi-vessel disease, whereas others had single-vessel disease. No difference was observed in stent diameter and the frequency of post-stent adjuvant ballooning among the groups. The incidence of PCI complications such as distal embolization or dissection was quite low and similar among the groups. All patients received either the everolimus-, zotarolimus-, or biolimus-eluting stents.
Comparison of myocardial perfusion parameters between the groups
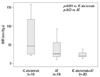
We compared the myocardial perfusion status using following parameters: TIMI flow grade and MBG on final coronary angiography, IMR by the pressure wire immediately after primary PCI, ST-segment resolution on ECG at 90 min, and MVO on CMR at day 5 (Table 3). The combination group had higher TIMI flow grade and MBG than did the IC abciximab group. No difference was found between the IC abciximab and AT groups regarding TIMI flow grade and MBG. IMR values were different between the 3 groups (Fig. 3). Post hoc analysis revealed that IMR was lower in the combination group than in the IC abciximab group (23.5±7.4 U vs. 66.9±48.7 U, p=0.001) and tended to be lower than in the AT group (23.5±7.4 U vs. 37.2±26.1 U, p=0.070). No difference of IMR was found between the IC abciximab and the AT groups (p=0.451). Fractional flow reserve, coronary flow reserve, coronary wedge pressure, and collateral flow index were similar between the groups. Thirty-one patients (77.5%) underwent CMR at day 5 after primary PCI. Four patients refused the exam and others could not complete the study because of claustrophobia (3 patients) and difficulty in breath-holding (2 patients). Ejection fraction, infarct size, and transmural extent of MI on CMR were not different between the groups. The incidence of MVO was not similar between the 3 groups (p=0.001). Post hoc analysis showed that the presence of MVO was lower in the combination group than in the IC abciximab group (18.8% vs. 88.9%, p=0.002) and tended to be lower than in the AT group with barely missed significance (18.8% vs. 66.7%, p=0.054). No difference in the presence of MVO was found between the IC abciximab and the AT groups (p=0.525).
Relation of IMR to clinical, angiographic, and CMR parameters
IMR was higher in subjects with MVO or MBG 0/1 than in those without MVO or with MBG 2/3 (53.4±44.3 U vs. 21.5±5.2 U for MVO, p=0.015; 75.2±50 U vs. 25.3±12.1 U for MBG, p=0.007). No difference of IMR was found in the ST-segment resolution (41.6±33 U vs. 33±32 U, p=0.408) (Fig. 4). Combination treatment using IC abciximab and AT [odds ratio (OR) 0.091, confidence interval (CI) 0.017-0.501, p=0.006], body mass index (OR 1.245, CI 0.983-1.577, p=0.052), hypertension (OR 4.083, CI 0.998-16.868, p=0.052), ischemic time (OR 1.008, CI 1.001-1.014, p=0.028), presence of MVO on CMR (OR 2.5, CI 1.345-4.646, p<0.001), and MBG 2/3 (OR 0.017, CI 0.002-0.174, p=0.001) were associated factors of high IMR (≥34 U) at the significance level of p<0.1. On multiple logistic regression analysis, the combination treatment (OR 0.111, CI 0.015-0.809, p=0.03) and body mass index (OR 1.346, CI 1.012-1.791, p=0.041) remained as independent parameters for the prediction of high IMR. One event that indicated recurrent MI occurred in the IC abciximab group, which was not related to the target vessel. No other event occurred during the 1-month follow-up period.
DISCUSSION
The main findings of the present study are as follows: 1) A combination of IC abciximab and AT seemed to be superior to each treatment alone in terms of enhancing myocardial perfusion, as assessed by on-site measurement of IMR after primary PCI for STEMI. 2) Higher IMR value was linked to lower MBG on coronary angiography and the presence of MVO on CMR.
Even when TIMI 3 epicardial flow is restored, patients with poor myocardial perfusion have a higher mortality than those with good myocardial perfusion.6 To attain adequate myocardial perfusion in patients with STEMI, prompt and proper revascularization is important. AT seemed to be beneficial because it can reduce distal atherothrombotic embolism through retrieval of in situ thrombus. Svilaas, et al.11,13 reported the advantages of manual thrombectomy over conventional PCI in terms of improving MBG as well as reducing the 1-year incidence of MI and cardiac death. Sardella, et al.12 also reported reduction in infarct size on CMR 3 months after primary PCI in subjects treated with manual thrombectomy, compared to those treated with conventional PCI. However, other studies9,10,16 failed to demonstrate the superiority of AT to conventional PCI in the treatment of STEMI. One meta-analysis17 showed that manual AT without a distal protection device was better than PCI alone for STEMI patients. Thus, AT is regarded as an important adjunctive tool in the treatment of STEMI, but its routine use is not yet a class I indication in the updated guidelines.30,31 It can be inferred that the benefit of AT might be enhanced in patients with a shorter ischemic time and heavy thrombotic burden.11,12 Lesion- or clinical-specific studies aimed at revealing the benefits of AT as an adjunct for STEMI is warranted.
The effect of several medications, such as verapamil,32 adenosine,33 nitroprusside,34 nicorandil,35 and Gp IIb-IIIa inhibitor,14,15,16 on preventing or reducing reperfusion injury has been investigated. However, their efficacy in improving myocardial perfusion was not consistent and remains debatable. Routine use of a Gp IIb-IIIa inhibitor such as abciximab is reasonable, but is not recommended as class I indication by the current guidelines.30,31 This may be partly due to the potential increase in bleeding. Instead of a bolus injection followed by continuous infusion of abciximab, a single bolus administration of abciximab was proposed to decrease bleeding complications while maintaining anti-ischemic efficacy.15 It was also suggested that direct IC injection of abciximab might be superior to its IV injection for improving myocardial perfusion.36,37,38,39 High local doses of abciximab may facilitate the dissolution of the antibody to platelets inside the flow-limiting thrombus, thus resulting in improved dissolution of thrombi and microemboli at the ruptured plaque and further downstream in the microcirculation. In fact, a few meta-analyses38,39 showed that IC abciximab was more effective in decreasing mortality than IV application. However, the largest randomized abciximab IC versus IV drug application in the STEMI (AIDA STEMI) trial40 and other meta-analysis,41 including the AIDA STEMI trial, showed no difference in mortality between IC and IV abciximab application. The neutral effect of IC versus IV abciximab might be due to its subsequent systemic IV infusion. In fact, the Intracoronary Abciximab and Aspiration Thrombectomy in Patients With Large Anterior Myocardial Infarction (INFUSE-AMI) trial16 revealed that IC abciximab via an infusion catheter reduces infarct size, as assessed by CMR after 30 days. All patients in our study and a majority of the patients in the INFUSE-AMI trial16 had only a bolus of IC abciximab without subsequent systemic IV infusion. Further studies comparing the efficacy of IC and IV abciximab bolus application without subsequent infusion are warranted.
A subgroup analysis of INFUSE-AMI16 and a meta-analysis17 suggest that a combination of AT and abciximab administration is the most efficient treatment for decreasing infarct size and mortality as compared to each treatment alone or no treatment with AT or abciximab. These findings are consistent with those of our study. If most thrombotic materials are retrieved by AT, IC abciximab could further dissolve residual in situ thrombus as well as microemboli in the microvasculature. Thus, IC abciximab application alone without AT may have a limited effect on decreasing a heavy thrombotic burden.
There are several methods to assess the adequacy of myocardial perfusion such as MBG on coronary angiography,6 ST-segment elevation recovery on ECG,42 or MVO on CMR.2 MBG can be easily assessed on angiography but is too subjective, and there is substantial inter- and intra-observer disagreement.6 High MBG and ST-segment resolution are not always consistent because of a potential electromechanical dissociation between microvascular blood flow and myocyte function.42 Meanwhile, the use of CMR has been increasing because it provides a comprehensive and multifaceted view of the heart, including left ventricular function and volumes, infarct visualization, viability, and MVO.18 A central hypoenhanced region within a hyperenhanced region corresponds to poor myocardial perfusion as assessed by MVO, which is a poor prognosis-related CMR parameter in patients with STEMI.19 Despite these advantages of CMR, its use is limited because of the following reasons. First, it is costly. Second, some patients, especially advanced-aged subjects, are not eligible for CMR because of claustrophobia or difficulty in breath-holding. Actually, because of the aforementioned reasons, only 77.5% of the patients underwent CMR in the present study. Fearon, et al.20,21 reported that IMR obtained immediately after primary PCI can be a novel method for the prediction of left ventricular remodeling and mortality. IMR was also a determinant of myocardial viability as assessed by 18F-fluorodeoxyglucose positron emission tomography.29 McGeoch, et al.22 observed that IMR was higher in patients with MVO on CMR. This corresponds well with our results that IMR was higher in subjects with MVO or MBG 0/1 than those without MVO or with MBG 2/3. Thus, IMR may be a useful semi-quantitative onsite tool to assess the state of myocardial perfusion and to predict mortality after primary PCI for STEMI. ECG or CMR can be used only as a prognostic indicator, whereas IMR may be used as a therapeutic guidance such as nicorandil application35 as well as a prognostic marker.20,21,29,35
There are several limitations in the present study. First, this is a single-centre study involving a small population. Thus, we could not sufficiently compare clinical and safety endpoints such as mortality and bleeding complications. Second, the study population was highly selective (15.5% STEMIs screened were randomized), that is, high-risk patients such as cardiogenic shock patients were excluded while hemodynamically stable subjects, who presented within 6 h of symptom onset and had a large angiographic thrombus burden, were included. Therefore, our findings cannot be extrapolated to all STEMI patients undergoing primary PCI. Third, 25% of non-anterior MI included in this study may influence the IMR value because IMR may be different according to the extent of myocardial territory. However, the frequency of anterior MI was similar between the groups. Fourth, even though ischemic time was not an independent factor for the prediction of high IMR value, shorter ischemic time would affect better myocardial perfusion status in the combination group. Finally, we did not use an IC infusion catheter to deliver abciximab. Therefore, the drug might have leaked into the aorta or the subtending coronary vessel, resulting in inefficient delivery to the plaque rupture site and corresponding myocardium.
In conclusion, AT followed by a bolus of IC abciximab may be an efficient adjunctive combination therapy to enhance myocardial perfusion in patients with STEMI who presented within 6 h and have a large angiographic thrombotic burden. Onsite measurement of IMR following primary PCI may be useful for the semi-quantitative assessment of the adequacy of myocardial perfusion. A randomized, controlled trial powered for clinical and safety endpoints is required to confirm the benefits of combination treatment using IC abciximab and AT in STEMI.






 XML Download
XML Download