

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Conventional coronary angiography was the gold standard for confirming the severity of coronary artery disease. It plays however a limited role as a screening test due to its invasiveness, and it detects only intravascular luminal narrowing.1,2,3
American College of Cardiology/American Heart Association/American College of Physicians-American Society of Internal Medicine guidelines recommend that the symptomatic patient with intermediate or high probability of coronary artery disease based on clinical history, exam, or electrocardiogram requires stress testing or conventional angiography.4 Conventional coronary angiography provides data on luminal size; however, it is limited to the detection of plaques in remodeling vessels and is not useful for the evaluation of the extra luminal features of lesions, such as wall thickness or plaque composition. Evaluation of the latter features has required the additional use of intravascular ultrasound (IVUS). Currently, the increased accuracy of multidetector computed tomography (MDCT) permits detection of coronary artery calcification and imaging of coronary artery stenosis after only one peripheral injection of a contrast agent.5 In contrast to conventional coronary angiography, MDCT can evaluate not only intra-luminal narrowing but also extra-luminal plaque and surrounding structures. Many studies have reported that non-invasive cardiac MDCT is appropriate for sensitivity and negative predictive value compared with conventional percutaneous coronary angiography.6,7,8,9
A previous screening for heart attack prevention and education task force report10 recommends coronary artery calcium score (CACS) as a screening method for atherosclerosis, and its categorization as 0, 1-99, 100-399, and over 400. The higher the CACS, the more atherosclerosis suspected. Coronary calcium, which provides prognostic information over traditional risk factors, is known as a limiting factor of evaluation in MDCT evaluation.11,12 However, this results was reported with a 16-channel or early 64-channel MDCT, and technology has evolved.
Therefore, we investigated the diagnostic accuracy of 64-channel MDCT in detecting coronary artery geography by comparing it with IVUS in symptomatic patients of intermediate risk group in each of the four CACS subgroup.
MATERIALS AND METHODS
Study population
Through review of medical records between October 2007 and February 2010, we found 69 patients with suspected coronary atherosclerotic disease who underwent MDCT before conventional coronary angiography with IVUS at Gangnam Severance Hospital, Yonsei University. Patients were included in this study if they had angina pectoris with an intermediate risk. The intermediate risk group was defined as 10-year risk of major coronary events of <30% according to the Framingham scoring system based on the Framingham Heart Study.13,14 For all patients, clinical data was collected including age, gender, body weight, body height, and common cardiovascular risk factors. Body mass index was calculated from body weight and body height. Of the 69 patients, we excluded 15 patients due to past medical history of coronary artery bypass surgery, stent insertion, atrial fibrillation, or a period longer than 180 days from MDCT to IVUS. Patients with acute coronary syndrome (ACS) were also excluded from this study.
64-channel MDCT scan protocol and data analysis
Cardiac MDCT was performed using a 64-channel MDCT scanner (Philips Brilliance 64, Philips Medical System, Best, the Netherlands). The scanning parameters were as follows: step-and-shoot axial scanning direction, 420 msec gantry rotation time, 120 kV, 210 mAs, 64×0.625 mm slice collimation, 4 cm table feed per rotation, and the center of the imaging window was set at 75% of the R-R interval. A 70 mL of iodinated contrast medium (Ioversol, Optiray 350, Tyco Health/Mallinckrodt, Petten, the Netherlands) was administered intravenously at a rate of 5 mL/sec followed by 50 mL of normal saline at a rate of 5 mL/sec using a power injector (Nemoto; Nemoto Kyorindo, Tokyo, Japan). Imaging was performed by using a real-time bolus tracking technique. The scans were started 7 seconds after a trigger threshold of 110 Hounsfield unit (HU) was reached.
Image reconstruction was performed on the scanner's workstation using commercially available software (Extended Brilliance Workstation, Philips Medical Systems, Best, the Netherlands). MDCT data were transferred for post-processing to an Aquarius Workstation V3.6 (TeraRecon, San Mateo, CA, USA). Multi-planar reformatted (MPR), curved-planar reformatted (CPR), and volume rendering images with orthogonal and perpendicular projections to the vessel courses of each coronary segment were generated for the evaluation of coronary artery disease (Fig. 1A).
MDCT scan images were analyzed by two radiologists who were blinded to the patients' identity, clinical history and results of coronary angiography. Stenotic area parameters [lumen cross-sectional area (CSA), external elastic membrane (EEM) CSA, among others] were measured on a magnification view of the selected MPR and CPR images including through plane projection with an electronic ruler on an Aquarius Workstation V3.6 (TeraRecon, San Mateo, CA, USA).
Conventional coronary angiography and IVUS technique
Conventional coronary angiography was performed according to standard techniques and at least two views in different planes view obtained for each coronary artery. After coronary angiography, 0.2 mg of nitroglycerin was administered to all patients before the introduction of the IVUS catheter. IVUS was performed using a 20 MHz, 2.9 F phase-array IVUS catheter (Eagle Eye, Volcano Corporation, Rancho Cordova, CA, USA) under fluoroscopic guidance, and motorized pullback at 0.5 mm/sec. All IVUS exams were digitalized for off-line analysis.
Image analysis was performed with the use of dedicated software (pcVH2.1, Volcano Corporation, Rancho Cordova, CA, USA). For each region of interest, relative compositional quantitative plaque parameters were obtained. The lumen and the media-adventitia interface were defined by automatic contour detection and manual editing was performed on all individual frames. For each frame, EEM CSA and lumen CSA were calculated. Measurements were made for the entire lesion, which was defined as the segment between the distal and proximal references.15 Plaque volume was calculated using Simpson's rule and averaged over the length of the lesion to generate a mean plaque area. The length of the lesion was measured in the longitudinal image (Fig. 1B).
Data analysis for MDCT and IVUS
The location of the target vessel and worst stenosis (the stenosis with the smallest lumen size) was selected on the basis of conventional coronary angiography and IVUS. For MDCT, minimal lumen CSA site was detected on the decided target vessel by coronary angiography. The lesion length was measured from normally looking proximal to normally looking distal portion in longitudinal view of IVUS and MPR or CPR view of MDCT. Proximal reference was defined as the site with the largest lumen proximal to a stenosis but within the same segment (usually within 10 mm of the stenosis with no major intervening branches).16 Proximal reference EEM CSA, lumen CSA, lesion length, and plaque volume were measured by IVUS and MDCT for the entire lesion, and EEM CSA, lumen CSA, and plaque components were measured at 3 points (a worst stenosis and 10 mm proximal and distal to a worst stenosis as shown Fig. 1 in each lesion).
Statistical analysis
Continuous values with normal distribution were expressed as means (with standard deviation) and compared with the two-tailed t test for independent samples. MDCT densities of plaques according to different plaque characteristics determined by IVUS were expressed as medians (with interquartile range) and compared with the two-tailed Mann-Whitney test. Correlation of IVUS measurements with MDCT was performed using Pearson's correlation coefficient. If the comparative parameter was too small to use the Pearson's correlation coefficient, the Spearman's correlation coefficient was used. Because of the small sample sizes, the Wilcoxon signed rank test was used for comparison of plaque remodeling between MDCT and IVUS. All analyses were two-tailed and p values <0.05 were considered as statistically significant. Statistical analysis was performed using SPSS (version 15.0, Statistical Package for the Social Sciences Inc., Chicago, IL, USA) software.
RESULTS
Patient characteristics
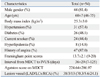
The baseline characteristics of the study population are summarized in Table 1. The location of the lesions in the 54 patients (female; mean age 59.9±6.9 years; age range 46-76) was the left anterior descending artery (LAD) in 38 (70.3%), the left circumflex artery (LCx) in 3 (5.6%), and the right coronary artery (RCA) in 13 (24.1%). Framingham point scores of the 54 subjects ranged from 9 to 20, corresponding to a 10-year risk of major coronary events of 5-30%.14
Comparison for each lesion between IVUS and MDCT
Average lesion length (20.0±8.6 mm on IVUS, 15.3±9.6 mm on MDCT, p=0.060) and plaque volume (160.8±84.7 mm3 on IVUS, 124.4±101.7 mm3 on MDCT, p=0.132) were not significantly different as measured by IVUS and MDCT, but there was a trend toward underestimation in the MDCT measurement (Table 2).
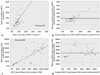
Each lesion was measured at 3 sites as shown as Fig. 1. In total, 162 sites identified on MDCT and IVUS were evaluated. IVUS and MDCT measurements were 14.84±4.73 mm2 versus 12.33±2.94 mm2 (p<0.01) for mean EEM CSA, 6.19±4.03 mm2 versus 6.45±4.53 mm2 (p=0.188) for mean lumen CSA. Although MDCT did not yield a significantly different lumen CSA, it significantly underestimated EEM CSA and plaque area (Table 2). Correlation for those measurements were close (r=0.514, 0.837, 0.578, p<0.01) (Fig. 2).
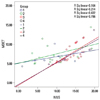
For evaluation of MDCT accuracy by coronary calcium content, 162 lesions were divided into 4 groups by CACS (Group 1, CACS 0; Group 2, CACS 1-99; Group 3, CACS 100-399; and Group 4, CACS over 400). There was also a good correlation for plaque area between MDCT and IVUS, although CACS was higher (Table 3, Fig. 3).
Inter-observer variability between two observers of plaque area on MDCT and MDCT values of plaque in MLA
The correlation coefficient of plaque area on MDCT was 0.797 between two observers and the Bland and Atman plot of plaque area revealed difference ±2 SD of 6.17±17.94 mm2 (Fig. 4).
The correlation coefficient of MDCT values of plaque in MLA was 0.608 between two observers and the Bland and Altman plot of MDCT values of plaque in MLA revealed a mean difference ±2 SD of 219.79±528.74 HU (Fig. 4).
DISCUSSION
This study showed that 64-channel MDCT allows accurate noninvasive determination of intra/extra-luminal coronary lesion in each CACS, comparing to IVUS. In this study, we divided all 162 lesions into 4 groups by CACS in MDCT. Even in the higher CACS categories, EEM CSA, lumen CSA, and plaque area showed good correlations between MDCT and IVUS.
For 64-channel MDCT, Leber, et al.7 reported a sensitivity of 84% and a specificity of 91% in the detection of proximal coronary plaques. There were correlations for plaque volume, EEM CSA, and lumen CSA measurements between MDCT and IVUS.
On the other hand, the present study revealed that MDCT relative to IVUS particularly underestimated lesion length, EEM CSA, and plaque area as previously reported studies.7,8,9 The reason could be that IVUS examination was performed after intracoronary nitroglycerine administration while MDCT was not. Also, after the guide wire passed through the lesion, the IVUS catheter was inserted for measurements which straightened the vessel possibly influencing measurement of the lesion length and plaque area. The fact that the LCx and RCA are more tortuous than the LAD could explain why measurements in LAD lesions were better correlated than in other vessels.17 Lumen CSA was relatively not affected probably because of its smaller magnitude and of contrast dye actually passing through the lesion.
Detection of intraluminal stenosis and atherosclerotic plaque by MDCT would be important determinants of treatment plan in intermediate-risk patients. Several studies have reported the diagnostic accuracy of MDCT in the quantification of coronary artery plaques,5,18,19 but it is only a structural and not a functional evaluation. The atherosclerotic plaques that are causally related to ACS reveal a variable extent of luminal narrowing but are almost always associated with expansive or positive vessel remodeling, and soft plaque composition.20 MDCT has the potential to enable detection of not only significant luminal stenosis but also vessel remodeling or plaque composition. Some institutions are now also using 128-channel MDCT and both a 256- and 320-channel MDCT have been introduced.21 The latter configurations offer the potential to image the entire heart in more detailed.
This study had several limitations. The use of IVUS during conventional coronary angiography was at operator discretion, thereby possibly introducing operator bias. Also, the study was retrospective and a single center study, therefore population was too small to generalize this result.
Despite these limitations, contrast enhanced MDCT has emerged as a promising noninvasive screening method for the detection and exclusion of obstructive coronary artery disease, since tomographic imaging allows multiplanar reconstructions of the tri-dimensional structure of the coronary arteries and it provides a more accurate description of eccentric stenosis and extra luminal structures such as plaque.
In conclusion, the information content of MDCT is broader than that of conventional coronary angiography, and the results of this study support that MDCT as being reliable enough for the evaluation of coronary artery stenosis in the intermediate-risk group independent of CACS. Therefore, MDCT might be used as an alternative screening method for the intermediate CAD-risk group and for plaque burden monitoring of known coronary atherosclerosis. However, 64-channel MDCT currently has a limited role in plaque characterization and further study is needed.




 XML Download
XML Download