

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hepatocellular carcinoma (HCC) is the seventh most common carcinoma worldwide and the third most common cause of cancer-related mortality.1 HCC is a highly malignant tumor with a propensity for invading intrahepatic vascular structures, the portal vein (PV), and the hepatic vein (HV). Infrequently, the tumor thrombi within the HV may extend into the inferior vena cava (IVC) and the right atrium (RA). The prevalence of intra-atrial tumor growth in autopsied cases of HCC ranges from 1 to 4.8%.2-4 With advances in imaging, intra-atrial tumor growth has been increasingly recognized in HCC patients.5-7 When HCC extends into the IVC or the heart, the prognosis is poor, with a median survival period of only 2-3 months.8 The prognosis of HCC patients with extrahepatic metastasis is unsatisfactory and often not well known. The median survival period is 4.9 months (range, 1-37 months).9
HCC extension into the heart can induce sudden pulmonary embolism, intractable heart failure, secondary Budd-Chiari syndrome, and ball-valve thrombosis syndrome, and all of these complications can cause sudden death.6,10
Aggressive surgical treatment and nonsurgical local treatment modalities11-15 are efficacious, although such procedures are usually prohibited in most patients with advanced HCC because of underlying cirrhosis and the advanced stage of the primary tumor. No established risk factors, prognostic factors or effective treatment strategies for HCC cases that extend into the heart have been reported to date. Chun, et al.16,17 reported that active treatment, such as radiation, systemic chemotherapy, and transcatheter arterial chemoembolization (TACE) beyond supportive care, may provide a survival benefit in patients with HCC that extends into the IVC/heart, but this study was limited by a small sample size.
Therefore, the current study aimed to evaluate the risk factors and predictive factors for poor prognosis of patients with HCC extending into the RA.
MATERIALS AND METHODS
Patients
From January 2004 to December 2012, a total of 1042 patients with newly diagnosed HCC were admitted to the Division of Gastroenterology at Chonnam National University Hospital in Gwangju, Korea. Overall, 377 patients were excluded because laboratory data available at the end of the follow-up period were incomplete. Information for 665 patients with newly diagnosed HCC were evaluated retrospectively. Among these patients, 33 patients had RA invasion during HCC followed up. In total, 632 patients who were diagnosed during the same period served as the comparison group. To describe the risk factors of HCC extension into the RA and determine predictive factors for poor prognosis in patients with HCC extending into RA, the data collected from the medical records included demographics, laboratory results, tumor characteristics, tumor stage, imaging studies, treatment modalities, and overall survival.
Diagnosis of HCC with RA invasion
The diagnosis of HCC was based on the following guidelines proposed by the Korea Liver Cancer Study Group and the National Cancer Center18: 1) nodules >2 cm in diameter with a typical pattern of HCC in one imaging study or alpha-fetoprotein (AFP) levels >200 ng/mL and 2) nodules between 1 and 2 cm in diameter with a coincidental typical vascular pattern in two imaging studies. If these criteria were not met, biopsies were performed. Clinical staging was based on the modified Union Internationale Contre le Cancer (UICC) tumor-node-metastasis classification and Cancer of the Liver Italian Program (CLIP) scores.18,19 RA invasion was defined as direct invasion from the liver into the RA or intra-cardiac tumor thrombosis and diagnosed using CT, MRI, positron emission tomography, or echocardiography during follow-up of HCC and new symptom development, such as aggravated dyspnea, ascites, and chest discomfort. HCC with RA invasion was commonly diagnosed using CT. On imaging, the RA embolus was commonly observed as having a regular, slightly irregular round, orbicular-ovate, or lobulated type. In the arterial phase, the embolus demonstrated slight enhancement, whereas in the portal phase and the delayed phase, the contrast media were partially discharged.20
Treatment modalities for HCC that extended into the RA
Medical chart review showed that 18 patients received supportive care and 15 patients received active treatment according to the individual situation such as economic state, Eastern Cooperative Oncology Group score, and patient's will to treat. To evaluate whether active treatment was superior to supportive care alone in terms of the overall survival of patients, we stratified 33 patients into the following two groups: a supportive care group (n=18) and an active treatment group (n=15). All of the patients were followed through December 2012.
Definition for poor prognosis group
According to Chern, et al.,8 when HCC extends into the IVC or the heart, median survival period is only 2-3 months.Therefore, we defined poor prognosis group as survival time shorter than 2 months.
Ethics statement
Written informed consent was obtained from all of the patients regarding the nature and the purpose of the treatment, and this study was approved by the IRB of our institution.
Statistical analysis
Continuous variables were expressed as mean±standard deviation. A Student's t-test and Pearson's chi-squared test or Mann-Whitney test were used to compare the baseline characteristics of the patients. Factors that were significant in the univariate analysis were entered into a stepwise multivariate analysis to determine which risk factors retained statistical significance and which factors were dependent on other factors. The survival times were estimated from the date of HCC diagnosis until death. Null hypotheses of no differences were rejected if the p values were less than 0.05 or, equivalently, if the 95% CI of the odds ratio estimates excluded 1. We performed statistical analysis using SPSS 20.0 (SPSS Inc., IBM Company, Chicago, IL, USA).
RESULTS
Patient characteristics
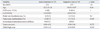
The median duration of follow-up was 857 days (2-3906 days). The mean age of the patients was 59.7 years (range 32-87 years), and there were 561 men (84.4%) and 104 women (15.6%) included in the study. Overall, 373 patients (56.1%) were positive for hepatitis B surface antigen, 105 patients (15.8%) were positive for antibodies against hepatitis C virus (anti-HCV Ab), 121 patients (18.2%) were chronic alcohol drinkers, 36 patients (5.4%) had a combined etiology, and 30 patients (4.5%) had an unknown etiology. Regarding treatment method, 433 patients (65.1%) underwent TACE, 83 (12.5%) RFA, 76 (11.4%) surgery, 2 (0.3%) radiation therapy (RT), 16 (24.1%) Sorafenib, 6 (0.9%) hepatic arterial infusion chemotherapy, and 49 (7.3%) supportive care. There were significant differences between the characteristics of the two groups (HCC with RA invasion vs. newly diagnosed HCC during the same period), including the modified UICC stage, the CLIP score, the Child-Pugh score, the serum C-reactive protein (CRP) levels, PV invasion, HV invasion, IVC invasion, tumor size, tumor type, and the duration of follow-up. The clinical characteristics of the two groups are shown in Table 1.
A total of 13 patients (39.3%) had aggravated abdominal distension and/or dyspnea, 11 patients (33.3%) had non-specific symptoms (fatigue or poor oral intake), 8 patients (24.2%) had aggravated right upper quadrant pain, and 1 patient (3%) had chest discomfort on diagnosis of HCC with RA invasion. Suspicious right heart failure signs, such as aggravated ascites/dyspnea (39.3%), were the dominant symptoms.
Risk factors for advanced HCC with RA invasion in uni-and multivariate analysis
Of a total of 665 patients with newly diagnosed HCC in our institution, 33 patients (4.96%) had RA invasion during HCC follow-up. In the univariate analysis, a modified UICC stage greater than IVA, a CLIP score >4, serum CRP levels >0.8 mg/dL, PV invasion, HV invasion, concomitant IVC and PV invasion, a tumor size ≥5 cm, a multinodular tumor type, and lymph node involvement were risk factors for HCC with RA invasion.
In the multivariate analysis, a modified UICC stage greater than IVA, HV invasion, concomitant IVC and PV invasion, and a multinodular tumor type were identified as independent risk factors (Table 2).
Predictive factors for poor prognosis in patients with HCC extending into the RA
According to survival time, 9 patients survived less than 2 months, 24 patients survived longer than 2 months. The patients with HCC extending into the RA were subdivided into shorter survival group (<2 months) and longer survival group (≥2 months). There were no significant differences between the characteristics of the two groups (shorter survival group vs. longer survival group) including gender, age, cause of HCC, antiviral treatment, the modified UICC stage, the Child-Pugh score, the serum CRP, AFP levels, HV invasion, IVC invasion, tumor size, tumor type, lymph node, distant metastasis except PV thrombosis (p=0.054), CLIP score >3 (p=0.057), and active treatment (p=0.07).
In multivariate analysis, CLIP score >3 (p=0.016, OR: 13.89) and active treatment (p=0.024, OR: 0.054) were associated with prognostic factors in patients HCC extending into the RA (Table 3). Regarding to treatment course of patients with longer survival >6 months, TACE (n=3), RT (n=1), TACE+RT (n=1), and Sorafenib (n=1) were performed.
Active treatment vs. supportive care in patients with HCC that extended into the RA
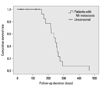
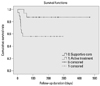
The median duration of follow-up in patients with HCC that extended into the RA was 123 days (range 2-467 days) (Fig. 1). Survival curve of patients with HCC and RA invasion between active treatment and supportive care are shown in Fig. 2.
The mean age of these patients was 60.88 years (range 37-86 years), and there were 28 men (84.8%) and 5 women (15.2%). The mean CLIP score was 3.39 (range 1-6), and the mean Child-Pugh score was 6.46 (range 5-11). There were no significant differences between the two groups (active treatment vs. supportive care) according to age, CLIP scores, Child-Pugh scores, PV invasion, tumor size, tumor type (Table 4). The treatment modalities in the active treatment group, including radiation, TACE, Sorafenib, and combined modalities, were performed according to the indications or situation for each patient (Table 5). After active treatment, most of patients who had right heart failure sign and chest discomfort had more improvement of symptom.
The causes of mortality in the best supportive care group included hepatic failure (n=6/18, 33.3%), tumor progression (n=5/18, 27.7%), upper gastrointestinal bleeding (n=2/18, 11.1%), ruptured HCC (n=2/18, 11.1%), sepsis due to pneumonia (n=1/18, 5.5%), and unknown causes (n=2/18, 11.1%).
In the active treatment group, the causes of mortality included hepatic failure (n=3/14, 21.4%), tumor progression (n=1/14, 7.1%), upper gastrointestinal bleeding (n=4/14, 28.5%), ruptured HCC (n=3/14, 21.4%), and cardiac problems (n=3/14, 21.4%). One patient is still alive until last follow-up.
DISCUSSION
The clinical course of HCC with a tumor thrombus in the PV, IVC, or RA is dismal. The median survival times of patients with an IVC tumor thrombus have been reported to be as short as 2-3 months without effective treatment.22 Because cases of HCC extending into the IVC/heart are rare and occur at a prevalence of 1-4%,10,23 effective treatment strategies and prognosis for these patients remain unclear.24,25 A few large-scale clinical studies of patients with HCC extending into the IVC/heart have been published,8,16 and no research has been done regarding the risk factors and the outcomes for HCC extending into the RA.
In our retrospective study, risk factors/predictive factors for prognosis and treatment outcomes were assessed with univariate and multivariate analysis.
The current study showed that HCC that extends into the RA is a rare disease (4.96%).
A modified UICC stage greater than IVA, HV invasion, concomitant PV and IVC invasion, and multinodular HCC are risk factors for advanced HCC with RA invasion. A CLIP score ≤3, active treatment may prolong survival in patients with HCC extending into RA. To the best of our knowledge, this study is the first to characterize the risk factors and predictive factors for poor prognosis of HCC extending into the RA.
In an autopsy study of 439 HCC cases, Kojiro, et al.3 found intra-atrial tumor growth in 18 cases. In addition, a continuous tumor thrombus that involved the RA, the IVC, and the HV was observed in 15 cases, and the tumors were observed to cross the tricuspid valve and enter the ventricle in five cases. Consistent with the findings of another studies,3,20 our study found a prevalence of HCC with RA invasion of 4.96%, and HV and IVC invasion were observed in most cases. IVC invasion was observed in 100% of the HCC cases with RA invasion. In our study, a modified UICC stage greater than IVA, HV invasion, concomitant IVC and PV invasion, and a multinodular tumor type were independent risk factors for HCC that extended into the RA. Therefore, tumor seeding through the venous system may be the most important route for HCC with RA invasion. As for symptoms, 13 patients (39.3%) had aggravated abdominal distension and/or dyspnea, 11 patients (33.3%) had non-specific symptoms (fatigue or poor oral intake), 8 patients (24.2%) had aggravated right upper quadrant pain, and 1 patient (3%) had chest pain. Because right heart failure signs (39.3%) were the dominant symptoms in patients with HCC that extended into the heart, we suggest that heart involvement should be suspected when HCC patients with high risk factors develop right heart failure signs, such as dyspnea, aggravated ascites, and/or lower leg edema.
In agreement with Chern's study, our study found that the median survival time for HCC patients with RA invasion was 123 days (approximately 4.1 months).
In regard with predictive factors for poor prognosis, neither liver function nor tumor stage are associated with survival. No active treatment and CLIP score >3 are significantly associated with short-term mortality.
As for treatment modalities, the results of earlier studies on surgical resection for the treatment of HCC with a metastatic IVC and RA tumor thrombus are disappointing results, with a mean survival time of approximately 8 months.26 Recent studies have found that TACE is the most widely used and effective treatment in patients with advanced HCC with IVC/RA invasion, and this treatment has been shown to provide a survival benefit to selected patients.8,13,20 Oral thalidomide and external beam radiation therapy have also been effective in advanced HCC with IVC/RA tumor thrombi; however, these treatment modalities were evaluated in small scale studies.14,27 Chun, et al.16 reported that active treatment, such as radiation, systemic chemotherapy, and TACE beyond supportive care, provided a survival benefit in patients with HCC that extended into the IVC/heart. In consistent with other studies, our study demonstrated that the active treatment such as RT, TACE, and Sorafenib prolong survival of patients with HCC extending into RA. However, it was difficult to evaluate the efficacy of each treatment modality because of the small sample size. To date, no effective therapies have been advanced for the treatment of HCC with IVC and RA tumor thrombi. Therefore, further studies are required to develop treatment strategies for HCC with IVC and RA invasion.
This study had several limitations. First, this was a retrospective, single-center analysis. Second, we did not confirm whether the intra-cardiac masses indicated HCC invasion or a benign cardiac tumor, such as myxoma. However, the incidence of cardiac tumors is low (0.02%), therefore, this might not have greatly influenced the results. Furthermore, the intra-cardiac masses were consistent with HCC according to the radiological findings. Third, we had a small sample size for comparing the poor prognosis factors among the patients with HCC extending to RA invasion.
In conclusion, HCC that extends into the RA is a rare disease (4.96%), and the median survival time of the patients in our study was 123 days.
A modified UICC stage greater than IVA, HV invasion, concomitant PV and IVC invasion, and multinodular HCC are risk factors for advanced HCC with RA invasion. Active treatment beyond supportive care may prolong survival.
However, larger prospective studies are needed to confirm these findings.




 XML Download
XML Download