

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hypertension, a primary risk factor for coronary heart disease,1 is a major health burden and the leading cause of death throughout the world.2 Hypertension is highly prevalent and is a major contributor to cardiovascular disease in the Asia-Pacific region.3 Among 15 Asian-Pacific countries, the prevalence of hypertension ranges from 5% to 47% in men and from 7% to 38% in women.4 In this region, hypertension is said to be the cause for up to 66% of hemorrhagic strokes, 45% of ischaemic strokes, and 39% of ischaemic heart diseases.4
The interest in hypertension for children and adolescents has been climbing for the last 20 years. There is growing evidence that risk for hypertension, a major modifiable cardiovascular risk factor, is established early in life.5 Past studies have shown that the atherosclerotic process begins as early as childhood, and moreover, a person's risk factors in cardiovascular diseases have been shown to continue over time from childhood to adulthood.6 Although clinical manifestations of atherosclerotic cardiovascular disease occur mainly in middle-aged or older subjects, vascular alterations start to appear in childhood.7 Accordingly, the early detection of risk factors can lead to the possibility of early treatment and prevention. In this respect, it has become important to estimate the stability of certain risk factors over time, and there has been an increasing interest in the study of the "tracking" of blood pressure values from childhood to adulthood.
Several longitudinal studies were conducted in the last decades to assess blood pressure tracking over time among children and adults.8-13 Recent findings on blood pressure tracking concluded that reliability of blood pressure tracking is quite high.14 Nevertheless, longitudinal data from different populations have shown different degrees of blood pressure tracking stability.15 Most longitudinal studies have been conducted in North American or European populations, and although there are some studies on blood pressure tracking in Asian populations,16-20 they are all short-term studies with only around 10 years of follow-up. In this study, utilizing data from 266 subjects who participated in the 24-year long Kangwha Study, we examined the stability of blood pressure tracking from childhood through adulthood.
MATERIALS AND METHODS
The Kangwha Study was a community-based prospective cohort study on hypertension and related risk factors. The study began in 1986 in Kangwha County, South Korea with 430 school children of age 6 years old (211 boys, 219 girls). The next year (1987), the number of participants expanded to 741 children (358 boys, 383 girls). The participants were followed annually until 1997 (to age 17 years old). After reaching 17 years of age, three additional follow-up examinations were performed in 1999 (age 19 years old), 2005 (age 25 years old) and 2010 (age 30 years old). The data encompass a 25-year period (1986-2010), in which 15 examinations were conducted. Because the number of participants increased significantly from 1987, we used data from 1987 through 2010 for the analyses of blood pressure tracking. In order to fully leverage the data available, the study was conducted for the longest period of time possible; the study dataset comprised 14 blood pressure measurements taken over a 24-year period (from 1987 to 2010) among 266 (123 male and 143 female) participants who completed the 2010 examination. All available cohort members participated in at least one examination at each time point; however, some eligible subjects withdrew or did not complete all examinations. Therefore, because not all subjects underwent the same number of examinations, the number of subjects for each year was different.
Blood pressure was measured from the right brachial artery with a standard mercury sphygmomanometer (Baumanometer; WA Baum, NY, USA) from ages 6 to 19 years old and with an automated blood pressure monitor (Dinamap 1846 SX/P; GE Healthcare, WI, USA) at ages 25 and 30 years. Blood pressure was measured using an appropriate cuff size, according to the individual's arm circumference after subjects had sat for 5 minutes. Measurements were performed in a standardized way by trained researchers. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured at least two times for each subject; the average of the two measurements was used in the analysis. SBP was determined as the first perception of sound (first Korotkoff sound, K1) and DBP was measured both at the fourth Korotkoff (K4) and fifth Korotkoff (K5) sound up to the year 1999. In the follow-up examinations, years 2005 and 2010, DBP was measured at only K5. For the analysis of DBP tracking, measurements at K5 were used.
Anthropometric measurements were carried out at each examination. Standing height and body weight were measured according to a predetermined protocol, and body mass index (BMI) was calculated as the weight in kilograms divided by the square of height in meters. Informed consent form was obtained from each participant. The protocol was approved by the Institutional Review Board of Severance Hospital at the Yonsei University College of Medicine.
Statistical analyses
Results are expressed as mean values with standard deviation. Student's t-tests were used for the comparison of study reparticipants versus non-participants. The data encompasses a 24-year period (1987-2010) with a possible 14 repeated examinations. Because not all subjects had the same number of examinations, tracking coefficients were estimated using a mixed regression model as follows:
Yit is the observations for subject i at time t; β0 is the intercept; Yit1 is the initial (first) observation for subject i; β1 is the regression coefficient used as the tracking coefficient; t is time; β2 is the regression coefficient for time; Xijt is the time-dependent covariate j for individual i; β3 is the regression coefficient for time-dependent covariate j; J is the number of time-dependent covariates; and εit is the 'error' for subject i at time-point t.21 The standardized value of regression coefficient (β1) was interpreted as a longitudinal correlation coefficient (tracking coefficient). To calculate the tracking coefficient for an outcome variable Y, the value of the initial measurement at t1 (Yit1) is regressed in the entire longitudinal development of that variable from t2 to tt. The relationships between the initial value at t1 and the values from t2 to tt are analyzed simultaneously, resulting in one single regression coefficient (β1). This model has two strengths when compared with other tracking models. One, being that it handles any missing values of the dependent variable, so a balanced data set is not necessary. The other, being that the use of covariates allows for adjustment for possible confounders. In the present analysis, BMI was included as a covariate. A Bonferroni correction for multiple comparisons (n=14) was applied, and p-values <0.0039 were considered statistically significant for this comparison. All analyses were performed with SAS software version 9.2 (SAS Institute, Cary, NC, USA).
RESULTS
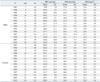
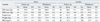
The main characteristics of the study participants at baseline and follow-up examinations are presented in Table 1. Boys and girls had similar SBP levels at baseline (99.9 mm Hg vs. 100.2 mm Hg), but men had higher SBP levels at the end of the follow-up period compared to women (124.9 mm Hg vs. 108.3 mm Hg). Men exhibited a higher increase in SBP levels over time than did women. The mean levels for DBP at baseline and at the end of the follow-up period were 57.0 mm Hg and 74.5 mm Hg in males and 58.2 mm Hg and 66.0 mm Hg in females, while BMI was calculated to be 15.6 kg/m2 at baseline and 24.3 kg/m2 at the last follow-up visit in males and 15.1 kg/m2 and 22.0 kg/m2 in females, respectively. We compared blood pressure and anthropometric measures between participants who were followed until 2010 and those who were not. There were no significant differences in SBP, DBP, height, weight, and BMI between the two groups (Table 2).
As shown in Table 3, significant 24-year tracking stability was observed in both sexes. The tracking coefficient (95% confidence interval) for SBP was 0.81 (0.52-1.11) in men and 0.72 (0.51-0.92) in women; DBP was 0.53 (0.26-0.80) in men and 0.33 (0.15-0.52) in women. Overall, the tracking coefficients were greater in men than in women. In particular, coefficients were higher for SBP compared to DBP. After adjusting for BMI, an indicator of general obesity, the tracking coefficient slightly decreased. The BMI-adjusted tracking coefficients (95% confidence interval) for SBP were 0.68 (0.39-0.97) in men and 0.67 (0.44-0.89) in women, which indicated a moderately high stability of tracking for both genders. The BMI-adjusted tracking coefficients for DBP were 0.51 (0.24-0.78) in men and 0.33 (0.15-0.51) in women. Moderate tracking stability was observed for DBP, although this was stronger for men than for women. All tracking coefficients were statistically significant (p<0.001).
DISCUSSION
This study provides data on 24 years of blood pressure tracking from childhood to adulthood in a Korean cohort. The main findings for this cohort consisted of the following: 1) there is a high tracking stability for blood pressure from childhood to adulthood, and 2) tracking coefficients were higher for SBP than DBP and higher in men than women.
Many longitudinal studies have demonstrated significant stability for blood pressure tracking from childhood to adulthood,8-13 which is of considerable public health interest because children who are at high risk for developing adult hypertension could potentially be identified at an early age. However, while the evidence for significant blood pressure tracking stability from childhood to adulthood is numerous, evidence for the reported degree of tracking stability is conflicting.22,23 The values of a tracking coefficient theoretically range between -1.0 and 1.0; however, since negative values indicate inverse relationships, which are unlikely between repeated measurements, only values from 0 to 1 are considered. Ulmer, et al.24 suggested a method for the interpretation of tracking coefficients: ≤0.30 is low stability, 0.30 to 0.59 is moderate stability, 0.60 to 0.89 as moderately high stability, and ≥0.9 is high stability. The tracking coefficients reported from previous review studies vary considerably from -0.17 to 0.81 for SBP and from -0.22 to 0.80 for DBP.12,14 In the five studies conducted on Asia populations,16-20 the lengths of the follow-up periods ranged from 4 to 11 years, and the tracking coefficients ranged from 0.35 to 0.53 for SBP and from 0.14 to 0.36 for DBP. However, it is difficult to compare tracking coefficients calculated in different studies. The five major factors that determine the size of the tracking coefficients include: the initial age of the subject, number of repeated measurements, time passed between measurements, length of the total time, and methodology used to assess tracking.13
Tracking coefficients are often found in longitudinal studies to be calculated as Pearson's correlation coefficients. Studies of blood pressure tracking have shown that as length of time between examinations increase, correlation coefficients become lower.14 Relatively few studies have investigated long-term tracking starting in childhood and continuing into adulthood. Other studies that assessed blood pressure tracking showed a slight increase with an increasing mean age at baseline.25
This study showed that the tracking stability of SBP was higher than that of DBP. Previous studies and meta-analyses have also shown the average SBP tracking coefficient to be higher than that of DBP.25 In the Kangwha Study, DBP was measured at both K4 and K5 until 1999; it should be noted that the measurement of DBP in children can be difficult in terms of discrimination and use of K4 and K5. The Fourth Report of the US National High Blood Pressure Education Program officially recommends the use of K5, and K4 should be used only if a very low K5 persists.26 In this study, results using K5 were presented.
In the present study, men exhibited a greater increase in SBP levels over time compared to women, and men had higher blood pressure tracking coefficients than women. Previous studies have reported conflicting findings regarding this issue. In earlier studies concerning gender differences in blood pressure tracking, neither the Tromso Study,10 nor the Amsterdam Growth and Health Study,13 found any major differences. In the Dormont High School Follow-Up Study,27 SBP tracking was higher for men than women (0.27 vs. 0.24, respectively), whereas in the Muscatine Study,28 women had higher DBP tracking than men of the some age groups. A recent meta regression analysis showed marginally higher SBP tracking in men compared with women (0.39 vs. 0.38, respectively) and higher DBP tracking (0.29 vs. 0.26).14 Dasgupta, et al.29 showed that boys are more likely than girls to develop high SBP as they approach adulthood. Although the differences in males and females from childhood to adulthood in this study cannot be explained fully, one possible explanation is that female blood pressure in adolescence or early adulthood tends to be influenced by pubertal circadian activities (e.g., menstrual cycle), as the tracking of blood pressure has been shown to be influenced by growth and development in puberty.30
Higher blood pressure is well-recognized to be associated with body weight or weight gain in children and adults,31 as well as with height in children.32 However, most studies reporting the tracking of blood pressure from childhood have not investigated the influence of weight or weight gain. When we adjusted for BMI, the tracking coefficients decreased slightly, but the tracking stability remained from childhood to adulthood.
This study has several strengths. First, one of the major and distinctive strengths of our study is that this study is the first long-term follow-up study of tracking individuals spanning over a 24 year period in an Asian population. Most longitudinal studies of blood pressure in childhood have generally included children with a wide range of ages, or frequently had a short follow-up interval. Therefore, our study is unique in that all participants were 7 years old when the study began and were followed for the next 24 years. Second, blood pressure was measured by trained observers using standardized methods every time, and we believe the measurement errors would be minimal. Third, a statistical analysis methodology that considered missing values was used. Our data set contained some missing values, so this methodology is appropriate. This study calculated the tracking coefficients using a different method than in other studies (i.e., correlation coefficients). The size of tracking coefficients in this study should not be directly compared with those assessed using other methods.
Our study has a potential limitation. Differences between non-participants and participants in the follow-up study may have led to some bias. However, our results are representative of the overall study population, as no significant differences between the non-participating and participating subjects were found when comparing either anthropometric or blood pressure measurements at baseline; it is implausible that there would be substantial differences in tracking of blood pressure over time in individuals who were and were not included in these analyses.
For this 24-year-long longitudinal study, we confirmed the stability of blood pressure tracking from childhood to adulthood in Korean population. In Asian countries, hypertension is particularly important because it is highly prevalent and is a major health burden. The results of our study call for a need to develop strategies and put into practice improvements in preventing hypertension. Because atherosclerotic vascular alteration begins in early life, preventive efforts that start in childhood may delay its progression to clinical disease and a portion of its burden.

 XML Download
XML Download