

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Prostate cancer (PCa) is the most common nondermatologic cancer in Western men.1 More than 90% of diagnoses involve localized tumors that are potentially curable by radical prostatectomy (RP).2 The incidence of PCa is higher in Western countries. A Western lifestyle, characterized by high caloric intake, low physical activity, and obesity, is believed to increase risk for PCa.3 The incidence of PCa in Asian men has also been increasing, especially in Japan, China, and Korea.4,5 PCa ranked as the fifth leading male neoplasm among Japanese men,6 and the sixth highest cause of cancer-related mortality in 2009.7 Morbidity due to PCa was reported to be 5.1% in Korean men ≥65 years old in 1990 and 9.1% in 2005, indicating an approximately two-fold increase.8 In 2011, PCa was reported to be the fifth most common malignancy in Korean men.9
RP for PCa carries an inherent risk of post-treatment morbidity. Treatment for PCa can change sexual, urinary, and bowel habits, which adversely affect post-treatment quality of life.10 The decision to perform RP for PCa should optimally weigh the benefit of treatment against the risks of treatment-related morbidity. Ideally, RP should be offered to men with a life expectancy of at least 10 years.11,12 However, life expectancy is a subjective measurement with significant bias.13
The presence of comorbidities is one of the important predictors of survival from malignancies.14 Several studies have attempted to develop comorbidity assessment tools for counseling patients about life expectancy before undergoing RP. These assessment tools include life tables, comorbidity indices, and nomograms. Although there is no consensus on which comorbidity assessment tool is most useful, the Charlson Comorbidity Index (CCI) has been one of the most extensively studied in men with PCa.15-18 Thus, the aim of this study was to evaluate the association between the CCI score and death from causes other than PCa among Korean men with clinically localized PCa who underwent RP. To our best knowledge, this is the first study to examine the relationship between the CCI and long-term survival outcomes of the patients with prostate cancer in Asia as well as in Korea.
MATERIALS AND METHODS
Patient cohort
Data from 336 patients who underwent RP for PCa between 1992 and 2005 at the Severance Hospital in Seoul, Korea were analyzed. Data included age, height and weight at the time of surgery, date of surgery, preoperative serum prostate-specific antigen (PSA), biopsy and pathologic Gleason scores, and clinical and final pathologic stages. Data regarding mortality and cause of death were also obtained from patient medical records in the database of the Yonsei Cancer Registry Center at the Severance Hospital. Tumors were staged according to the 2002 American Joint Committee on Cancer staging guidelines. The follow-up period was calculated from the time of surgery to the date of the last known contact with the patient or the date of death. The primary outcome for this study was death from causes other than PCa.
Good clinical practice protocols
The study was performed in agreement with applicable laws and regulations, good clinical practices, and ethical principles as described in the Declaration of Helsinki. The Institutional Review Board of the hospital approved this study protocol (approval number: 4-2012-0906). This report was prepared in compliance with the Strengthening the Reporting of Observational Studies in Epidemiology checklist (version 3, accessible at http://www.strobe-statement.org).19
Definition of survival
PCa-specific survival (PCaSS) was defined as the time from RP to death due to PCa or complications of this disease. Overall survival (OS) was defined as the time from RP to death by any cause. Non-PCaSS was defined as the time from RP to death due to causes other than PCa or complications of PCa. If PCa was recorded as the underlying cause of death, or if a patient with known metastatic PCa died, then mortality was considered to be a result of PCa. Deaths in which PCa was not the underlying cause were classified as non-PCaSS or due to causes other than PCa.
Charlson Comorbidity Index
The CCI score was calculated from hospital discharge records and assigned according to the Dartmouth-Manitoba modification of the CCI, which was used to convert International Classification of Disease 10 code (ICD-10), and is more applicable to studies of surgical patients.20 The CCI features 19 conditions that have assigned scores of 1, 2, 3, or 6 based upon severity of disease. The CCI score was derived by adding the scores for all comorbidities. Based on the distribution of CCI score in our patient cohort, the men who received RP were classified into two CCI score categories, which were 0 or ≥1. PCa was not scored in the CCI calculation for this study. Two researchers (JYL and DHL) independently assessed medical records and assigned CCI scores to all patients. Discrepancies in scoring between the two researchers were resolved by discussion until a consensus was reached or by independent assessment by a third researcher (KSC).
Statistical analyses
Kaplan-Meier curves were used to estimate the probabilities of death from non-PCa-related causes and PCa-related causes by two CCI categories. The Cox proportional-hazards regression model was also used to estimate the hazard ratio (HR) and 95% confidence interval (CI) of death from non-PCa-related causes and PCa-related causes, age, body mass index (BMI), preoperative PSA, pathologic stage, and pathologic Gleason score. Integrated area under the curve (iAUC) was based on Cox proportional-hazards regression model.21 Two-sided tests were performed and p-values <0.05 were considered statistically significant. Statistical analyses were carried out with R (R version 3.0.1, R Foundation for Statistical Computing, Vienna, Austria; http://www.r-project.org) and its risksetROC package for iAUC based on Cox proportional-hazards regression model.
RESULTS
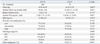
The mean age of enrolled patients was 64.31±6.12 years. The median PSA (interquartile range, IQR) was 11.30 (7.35 and 21.02) ng/mL with a median follow-up period (IQR) of 96 (85 and 121) months. The mean CCI at the time of RP was 0.28 (range 0-4) in 336 men.
A CCI score of 0 was assigned to 266 (79.2%) patients. A CCI score of 1 was assigned to 51 (15.2%) patients. A CCI score of 2 was assigned to 16 (4.8%) patients. CCI scores of 3 or 4 were assigned to three (0.9%) patients. Subjects were then divided into two subgroups according to CCI=0 (Group 1, n=266) or ≥1 (Group 2, n=70). Median PSA (IQR), which were 12.00 (7.75, 21.95) ng/mL in Group 1 and 9.56 (6.12, 15.02) ng/mL, demonstrated statistical differences in both groups (p=0.007). Median follow-up periods (IQR) were 99 (86, 109) months in Group 1 and 91 (82.75, 111.20) months in Group 2 (p=0.001). Only 19 men (27.1%) in Group 2 had histories of other malignancies, including stomach cancer (eight cases), renal cell carcinoma (six cases), colorectal cancer (two cases), laryngeal cancer (one case), duodenal cancer (one case), and bladder cancer (one case). In contrast, patients in Group 1 did not have histories of other malignancies (p<0.001). There were no significant differences in mean age, biopsy Gleason score, BMI, D'Amico risk stratification, or pathologic stage between the two groups (Table 1).
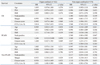
Five-year OS, PCaSS, and non-PCaSS were 91.7% (95% CI 0.888-0.947), 96.3% (95% CI 0.943-0.984), and 95.2% (95% CI 0.929-0.988), respectively. Ten-year OS, PCaSS, and non-PCaSS were 81.9% (95% CI 0.772-0.868), 92.1% (95% CI 0.887-0.956), and 88.9% (95% CI 0.849-0.930), respectively (Fig. 1A). CCI had a significant influence on OS (p=0.022) and non-PCaSS (p=0.008) by log-rank test, but did not affect PCaSS (p=0.681) (Fig. 1B, C and D). In multivariate Cox regression analyses, OS was independently associated with CCI (HR=1.907, p=0.025) and Gleason score (HR=2.656, p<0.001). PCaSS was associated with pathologic N stage (HR=2.857, p=0.031), pathologic T stage (HR=3.775, p=0.041), and Gleason score (HR=4.308, p=0.001). Non-PCaSS had a significant association only with CCI (HR=2.540, p=0.009) (Table 2). The iAUC, based on Cox regression model according to CCI, also demonstrated that the AUC of non-PCaSS was higher than OS and PCaSS (Fig. 1E).
Patients were then sub-grouped as pT2 (n=162) and pT3/4 (n=174). Patients in the pT2 group had disease confined to the prostate. The CCI correlated with OS and non-PCaSS, but not PCaSS. However, the CCI was not associated with OS, PCaSS, or non-PCaSS in the non-organ confined pT3/4 group (Table 3).
DISCUSSION
The National Comprehensive Cancer Network guidelines for PCa suggest that RP and/or radiation therapy should be offered only to men who are likely to survive for more than 10 years.22 According to these guidelines, urologists have to make treatment decisions based upon the life expectancy of a patient and the characteristics of the tumor. However, age is not the sole determinant of a patient's life expectancy. Comorbidities should also be considered. To our best knowledge, the current study is the first to examine the relationship between the CCI and mortality in Asian men with PCa. The results showed that the CCI was independently associated with both OS and non-PCaSS in patients with localized tumors who were treated with RP. However, the CCI had no impact on PCaSS in these patients. This indirectly suggests that comorbidities should be considered during selection of treatment modalities for PCa. Furthermore, the data suggest that radical surgeries should be reserved for physically healthy patients.
Population-based or retrospective cohort studies have been performed in Western countries to evaluate relationships between cancer-specific survival and preoperative comorbidities. Post, et al.23 showed that comorbidity was the most important prognostic factor for 3-year survival among 1337 men who were younger than 75 years old and were diagnosed with T1-T3M0 PCa. Furthermore, subgroup analysis revealed that individuals treated with RP were younger and had fewer comorbid conditions than patients receiving non-surgical treatment. Lund, et al.24 also demonstrated a correlation between comorbidity and survival in Danish patients with PCa, suggesting that comorbidities were negative prognostic factors for survival in men with PCa. Recently, the European Multicenter Prostate Cancer Clinical and Translational Research Group reported that long-term PCaSS after RP was modest and represented the leading cause of death in young and healthy patients. However, according to a multi-institutional study involving a cohort of 3832 men who received RP, patients with PCa who were older, sicker, and had multiple risk factors were at the highest risk of dying from non-PCa-related causes.25
Daskivich, et al.26 also assessed the competing risks for non-PCa-related mortality and PCa-related mortality among 1482 men in the California Cancer Registry who had nonmetastatic prostate cancer and differing CCI scores and tumor risks. After a mean follow-up period of 6.0 years, 370 (25%) men died from other causes, whereas 44 (3%) died of PCa. According to a competing risks regression analysis, each point of increase in the CCI was associated with a 2-fold increase in hazard of non-PCa-related mortality. Furthermore, they concluded that men with the highest CCI should consider conservative management of low-risk and intermediate-risk tumors because of exceedingly high risk of death from other causes and low risk of prostate cancer mortality. Thus, several population-based studies on PCa and preoperative morbidities have been published from western countries. However, studies with long-term follow-up focused on Asian populations have not been reported prior to our current analysis.
Albertsen, et al.27 examined the survival probabilities for 767 patients with localized PCa who were treated conservatively (either by observation or with immediate or delayed androgen withdrawal therapy). The 15-, 20-, and 25-year OS rates in patients with a CCI of 0-1 were 26%, 15%, and 8%, respectively. However, the 15-, 20-, and 25-year OS rates in those with a CCI ≥1 were 11%, 6%, and 3%, respectively, clearly showing that a higher CCI correlated with a worse survival outcome. These long-term follow-up results with conservative management were similar to our results with RP. In addition, our study also suggested that CCI had a strong influence on OS and non-PCaSS, but not on PCaSS, in patients with organ-confined disease. These data indicate that patients with early-stage disease and comorbidities should be managed conservatively. In contrast, the significance of CCI was different for patients with locally advanced or high risk PCa. Hsu, et al.28 analyzed the relationship between age, CCI, and outcome in 200 patients with cT3a PCa from Belgium, and concluded that the CCI did not influence the outcome in patients with locally advanced PCa. These results are consistent with our subgroup analysis for non-organ-confined T3/4 disease. We could not conclude from our study which treatment option is optimal. Nevertheless, a more aggressive approach might be considered for PCa patients with advanced T3/4 disease regardless of their CCI.
There were some limitations and intrinsic shortcomings due to the retrospective nature of this study. First, the sample size was relatively small compared with previous population-based trials. Second, there is inherent selection bias due to the fact that patients with many comorbidities are often treated with less invasive methods, such as radiation therapy, hormonal therapy, or watchful waiting. Actually, the median PSA in Group 1 was significantly higher than Group 2 [12.00 (7.75, 21.95) ng/mL versus 9.56 (6.12, 15.02) ng/mL, respectively; p=0.007]. Treatment decision in our patient cohorts may be based on comorbidities, however, there were no statistical differences in D'Amico risk stratification unlike the median PSA between two groups. Third, there is bias derived from the differences between preoperative and postoperative treatments, which may be an important confounding factor in our study. Despite these limitations, the present study demonstrates a novel association between the CCI and both OS and non-PCaSS after RP in Asian men with PCa. These findings have particular clinical relevance, as they suggest that patients with localized tumors and multiple comorbidities should be managed more conservatively.
The incidence of cardiovascular disease and metabolic syndrome in Asian men is different from that in Western men according to epidemiologic studies.29 However, Asian elders also have a higher risk of chronic diseases, including myocardial infarction, diabetes mellitus, hypertension, stroke, chronic bronchitis, asthma, and peptic ulcer disease.30 In a Korean geriatric cohort study, 78.0% reported that they had a diagnosed disease, 11.0% reported being cured of previous disease, and 46.8% were diagnosed with more than two diseases. The mean number of morbidities per elderly Korean was 1.62±1.35.31 A westernization of diet and a reduction in physical activity may have contributed to metabolic imbalance, obesity, and a dramatic increase in cardiovascular disease and diabetes within the Asian community.32 Although the Asian lifestyle has become westernized, the similarities and differences between comorbidities in Asian and Western countries remain to be elucidated. Nonetheless, the relationship between comorbidity and survival in Asian men with PCa must be emphasized.33 CCI is clearly a valuable preoperative tool for evaluating and counseling Asian patients with PCa. An Asian-specific cormobidity index should be designed and made clinically available in the near future. Recently, a newly developed comorbidity index using Korean hospitalized patient data based on the ICD-10 was also validated.34
In summary, the CCI was independently associated with both OS and non-PCaSS after RP, but had no impact on PCaSS. Selection of RP as a curative modality for PCa should take a patient's comorbidities into consideration. The CCI is a potentially valuable tool for preoperative evaluation and counseling of Asian patients with PCa. An Asian-specific cormobidity index should be designed and made clinically available in the near future.


 XML Download
XML Download