

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Dexmedetomidine, a potent selective α2-adrenergic agonist, is frequently used off-label in children because of its efficacy and lack of respiratory depression.1,2 Because dexmedetomidine has sedative, hypnotic and analgesic properties, it can reduce the dose of hypnotics, opioids, analgesics, and anesthetics required to be concomitantly administered.3 Intraoperative administration of dexmedetomidine reduced sevoflurane requirements in children undergoing various surgeries.4-6
Emergence agitation (EA) occurs frequently in children during recovery from anesthesia. The etiology of EA includes multiple factors, such as pain, anxiety, surgical type, personal character, rapid awakening, and anesthetic type, and sevoflurane has been considered to cause a higher incidence of EA than other anesthetics in pediatric patients.7-9 The incidence of EA under sevoflurane anesthesia varies from 10 to 70% depending on the definition of EA.4,10-13 Several preventative strategies have been investigated for EA under sevoflurane anesthesia in children.14-16 Also, intraoperative administration of dexmedetomidine has shown to effectively reduce EA in children because of its anxiolytic and analgesic properties without respiratory depression.4,12,13,17,18
In this randomized double blind study, we hypothesized that intraoperative use of dexmedetomidine would reduce sevoflurane requirements in children undergoing ambulatory surgery. Furthermore, we evaluated the effects of dexmedetomidine on recovery profiles and EA.
MATERIALS AND METHODS
The study was approved by the Institutional Review Board of Severance Hospital (IRB number: 4-2011-0430) and registered to the www.ClinicalTrials.gov (NCT01691001). After obtaining written informed consent from parents, 40 children, ASA 1, aged 1-5 years (≤20 kg) who were undergoing ambulatory hernioplasty or orchiopexy were enrolled in this study. Children with mental retardation, developmental delay, neurological or psychiatric illnesses that may be associated with agitation, coagulation disorder, spinal anomalies, or bilateral procedures were excluded.
The patients were randomly assigned to two groups; those who received dexmedetomidine (Group D, n=20) or saline (Group S, n=20) using a computer-generated randomization. Drugs used in the study were prepared in an anesthesia preparation room and coded as A or B by a nurse who was blinded to the study. For Group D, dexmedetomidine (Precedex™, Hospira Worldwide, Lake Forest, IL, USA) was mixed in normal saline to make 1 µg/mL in a 50 mL syringe. For Group S, normal saline was also prepared in a 50 mL syringe, and no premedication was given. To reduce preoperative anxiety, the children were moved to the operating room while watching an animated movie with their parents, and the parents remained next to the children until the children lost consciousness. Anesthesia was induced via a face-mask with 6-7% sevoflurane in oxygen at a gas flow of 4 L/min. The induction scale was assessed based upon mask acceptance (1=accept mask readily; 2=slight fear of mask, easily calmed; 3=not calmed with reassurance; 4=terrified, crying, agitated).19 A scale score of 1 or 2 was considered to be satisfactory induction. After the loss of consciousness, intravenous access was achieved. The coded drug was accordingly given to each group by the blinded anesthetic practitioner. The drug of 1 µg/kg was administered intravenously over 10 min using a syringe pump, followed by a 0.1 µg/kg/h infusion until the end of surgery in both groups. In Group S, the same amount of saline was administered in an identical sequence. When the bispectral index (BIS) score reached 40, the laryngeal mask airway (LMA) was inserted. A caudal block was then performed with 1.3 mL/kg of 0.2% ropivacaine (maximum volume, 20 mL) in both groups. Successful drug injection within the caudal space was routinely confirmed with ultrasound. As soon as caudal block was done, the operation was started. Anesthesia was maintained by adjusting the end-tidal concentration of sevoflurane (ET-sevo) to achieve a BIS score of 45-50 during surgery. During operation, no additional analgesics were given. Respiration was maintained spontaneously throughout the operation. When skin suture was started, sevoflurane and dexmedetomidine or saline administrations were discontinued. All patients were kept breathing spontaneously throughout the surgery. The LMA was removed when the patients opened their eyes spontaneously or moved when their chins were lifted. Time to LMA removal was defined as the time interval from 'end of operation' to 'LMA removal' and regarded as the time to awake.
ET-sevo, mean arterial pressure (MAP), and heart rate (HR) were recorded just before dexmedetomidine administration (T0, baseline), just after dexmedetomidine loading of 1 µg/kg (T1), 10 min after dexmedetomidine loading (T2), start of operation (T3), 10, 20, 30 min after the start of operation (T4, T5, T6), and at the end of operation (T7). Atropine 0.01 mg/kg was administered during the procedure when the HR decreased >30% of baseline value (T0). The patients were monitored in the post-anesthetic care unit (PACU) by a nurse and their parents, both of whom were blinded to the child's group allocation. Because most of the EA episodes occurred within 30 min of PACU arrival,13,18,20 EA was assessed at arrival and every 5 min for up to 30 min in PACU. EA was rated using a four-point scale modified by Watcha, et al.21 (1=calm, 2=crying, but can be consoled, 3=crying and cannot be consoled, 4=agitated and thrashing around). If a child fell asleep, this was defined as a score of 0. Children with scores of 3 or 4 were considered to have had an EA episode. Postoperative pain was assessed with the Children's Hospital of Eastern Ontario Pain Scale (CHEOPS)22 and the Face, Legs, Activity, Cry, Consolability scale (FLACC)23 upon PACU arrival, at 30 min, 60 min, and 120 min postoperatively. When children showed CHEOPS or FLACC scores ≥4, 0.5 µg/kg of fentanyl was administered. Sedation level was assessed with the Ramsay's sedation scale (1=anxious and agitated or restless, or both; 2=co-operative, oriented, and calm; 3=responsive to commands only; 4=exhibiting brisk response to light glabellar tap or loud auditory stimulus; 5=exhibiting a sluggish response to light glabellar tap or loud auditory stimulus; and 6=unresponsive).24 The first oral intake time and discharge time were recorded, and adverse events were also noted.
Statistical analysis
Sample size calculation was based on previous studies.4,25 In these studies, ET-sevo was decreased 33.1% and 41.6% in patients who received dexmedetomidine.4,25 If dexmedetomidine infusion can reduce 35% of the ET-sevo, the difference of the means of ET-sevo would be 1.0%, and SD would be estimated as 1.0%. For an α=0.05 and a power of 80%, 17 patients were required per group. Therefore, 20 patients were included in each group to allow for possible drop-outs.
Data were analyzed using IBM SPSS Statistics 19™ (SPSS Inc., Chicago, IL, USA). The normality of distribution was assessed with a Q-Q plot and the Shapiro-Wilk test. Parametric data were analysed with the independent t-test, and non-parametric data were analyzed using the Mann-Whitney U test. Categorical data were analyzed using the χ2-test or Fisher exact tests when appropriate. A repeated measures analysis of variance was performed to compare repeated measure variables (ET-sevo, MAP, and HR) with a Bonferroni correction for multiple comparisons. Data are presented as mean±SD, median (range) and number. A p-value <0.05 was considered statistically significant.
RESULTS
Of a total of 47 patients assessed for eligibility, 40 subjects received dexmedetomidine or saline after randomization and none were eliminated from the data collection (Fig. 1).
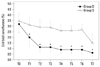
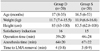
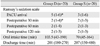
No differences were seen in demographics and anesthetic characteristics between the two groups (Table 1). As shown in Fig. 2, ET-sevo was significantly lower in Group D than in Group S after dexmedetomidine administration; ET-sevo reduced by 60% (±10) in Group D compared to Group S.
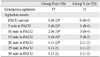
The incidence of EA was lower in Group D than in Group S (5% vs. 55%, p=0.001) and agitation scores were significantly lower in Group D than in Group S during the first 20 min after PACU arrival (Table 2).
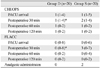
Pain scores were comparable in the two groups except at 30 min in PACU. Fentanyl was given in 2 patients of Group S for pain control in the PACU (Table 3). Sedation scores were significantly higher in Group D than in Group S at the time of arrival in the PACU and at 30 min (Table 4).
The hemodynamic changes are shown in Fig. 3. MAP and HR were significantly lower in Group D than in Group S; MAP and HR decreased by 22-28% and 18-21% respectively in Group D than Group S. Atropine was administered to 6 patients of Group D who showed bradycardia with or without hypotension (p=0.020), during the dexmedetomidine load.
First oral intake and discharge time were not different between the groups. There were no significant adverse effects related to the anesthesia such as nausea, vomiting, or urinary retention (Table 4).
DISCUSSION
The results of this prospective double-blinded randomized study suggest that intraoperative dexmedetomidine infusion reduced anesthetic requirements and decreased emergence agitation without delaying discharge in children undergoing ambulatory surgery.
Dexmedetomidine is a potent α2-adrenoceptors agonist, and presynaptic activation of α2-adrenoceptors in the locus ceruleus is responsible for both analgesic and sedative effect.3,26 Therefore, dexmedetomidine may be an effective adjuvant during general anesthesia by decreasing the doses of anesthetics and analgesics.27-29 The primary end-point of this study was the reduction of ET-sevo to maintain a BIS score of 45-50 during surgery. To provide adequate anesthetic depth, the BIS was kept within 45-50 range in both groups. Although it is considered that BIS has low sensitivity and specificity to assess the anesthetic depth and it may be dependent on anesthetics used, it is usual to maintain BIS values less than 50 during anesthesia in children.30
In several studies performed on adults undergoing abdominal surgery, ET-sevo was decreased by 27.3-33% with a dexmedetomidine 1 µg/kg bolus and a 0.4-0.6 µg/kg/h infusion.25,29,31 In pediatric tonsillectomy patients, the ET-sevo can be reduced up to 41.6% with a dexmedetomidine 2 µg/kg bolus, followed by 0.7 µg/kg/h infusion when compared with intraoperative fentanyl bolus.4 The analgesic-sparing effect of dexmedetomidine can be enhanced when using N2O.32 Supplemental drugs such as dexamethasone and acetaminophen may affect the additive analgesic interactions of dexmedetomidine and sevoflurane.4 In our study, no supplemental drugs or N2O were given during surgery, and the ET-sevo of Group D was reduced by 23.8-67% compared to Group S, despite the low dose of dexmedetomidine (1 µg/kg bolus, followed by 0.1 µg/kg/h infusion).
In previous studies in children, dexmedetomidine infusion rate varied (0.2-0.7 µg/kg/h) under sevoflurane anesthesia.1,4,12,17,29 We selected a low infusion rate of dexmedetomidine (0.1 µg/kg/h), because the children were undergoing minor urological surgery and supplemental caudal block. Inguinal hernioplasty or orchiopexy produce less surgical stimulation than other procedures, such as tonsillectomy. The anesthetic-sparing effects of dexmedetomidine may differ according to the type of surgery in addition to dexmedetomidine dose, different age of patients and combined effects of anesthetics or analgesics.3,20,27,28,32,33
EA is not a new phenomenon, though its prevalence has increased with the introduction of sevoflurane, especially in pre-school aged children. EA is self-limiting and resolves spontaneously, but restless recoveries can result in patient injury, surgical site damage and dissatisfaction for patients and parents. This characteristic of EA has been attributed to several factors such as patient-related (age, anxiety, and temperament), anesthesia-related (rapid emergence, and anesthetics), and surgery-related (pain and surgery type).9 In the current study, we tried to exclude several possible factors of EA such as preoperative anxiety, surgical type, and postoperative pain. The incidence of EA has been reported up to 70% in sevoflurane anesthesia.11 Sevoflurane even causes a high incidence of EA in the absence of surgery.9,18 The reason for frequent EA after sevoflurane is not clearly understood. Nevertheless, sevoflurane in any particular situation may exert an irritating effect on the central nervous system,34,35 although it was suggested that the type of inhalation agent may not be directly correlated with the incidence of EA.36
In the current study, we found that dexmedetomidine administration reduced EA significantly without delaying discharge. A single dose or continuous infusion of dexmedetomidine reduces EA after sevoflurane in children.4,12,13 The reason for reducing EA is yet unclear, however, the analgesic and sedative effects of dexmedetomidine may provide a protective effect against EA.4,12,13,18 However, in a recent meta-analysis that evaluated prevention of EA, analgesic properties did not seem to play a role in preventing EA.37 A recent study also suggested that lower incidence of EA could be related to the lower concentration of sevoflurane.14 The combined effects of reduction of sevoflurane and dexmedetomidine administration might have reduced the incidence of EA in our study.
Time to LMA removal which is also regarded as the time to awake was not different between the two groups. Furthermore, the LMA removal time of Group D was short compared to other studies.4,12,38 These different results may be due to the low infusion rate of dexmedetomidine and the type of surgery (minor urological surgery).
Dexmedetomidine can also cause a variety of hemodynamic changes in children.1,2,39 The most common hemodynamic effects of dexmedetomidine are bradycardia and hypotension, which are attributed to central α2-agonist proper-ties.1 Transient hypertension can also be result from perip-heral α-receptor stimulation.1 In the current study, Group D showed significantly lower MAP and HR during operation than Group S. Although the hemodynamic changes varied according to dose and surgical type, hemodynamic instability may occur frequently in minor surgery even if low doses of dexmedetomidine are used.1,2,4,12
The limitation of this study is uncertainty about whether we used a proper scoring tool for EA. The pediatric anesthesia emergence delirum scale developed by Sikich and Lerman40 is a valid and reliable rating scale, but it may not be applicable to children who are asleep in the PACU. Therefore, we used a scale by Watcha, et al.,21 which includes a consolability component. Although there is a risk of mis-scaling due to pain, we excluded the possibility of pain because we confirmed successful drug injection within the caudal space using ultrasound. In addition, since sample size calculation was based on ET-sevo, sample size may not be enough to check emergence agitation. Therefore, emergence agitation observed in Group D may be underpowered.
In conclusion, intraoperative dexmedetomidine 1 µg/kg bolus, followed by 0.1 µg/kg/h infusion, significantly reduced anesthetic requirements and also decreased the incidence of EA during recovery without delaying discharge in children undergoing ambulatory surgery. However, caution should be taken because of the side effects including hypotension and bradycardia.


 XML Download
XML Download