

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Advances in medical care have resulted in more patients requiring long-term home mechanical ventilation (HMV), and all too often results in ventilator users left with tracheostomy tubes without physical medicine and rehabilitation (PM&R) interventions.1 The cornerstone of PM&R intervention is pulmonary rehabilitation (PR). While most of the clinical care of pulmonary disease is limited to medical treatments, PR deals with a comprehensive intervention, based on a thorough patient assessment, followed by patient-tailored therapies, which include exercise training, education and behavioral changes designed to improve physical and psychological condition of people with chronic respiratory diseases.2 PR has long been directed to improving the medical and functional status of patients with parenchymal lung diseases such as chronic obstructive pulmonary disease,3 however, similar principles have generally been ignored for patients with neuromuscular diseases (NMDs). These measures can also be of value for patients with NMDs. In addition, the use of inspiratory and expiratory muscle aids, including noninvasive mechanical ventilation (NIV) and mechanically assisted coughing (MAC), can facilitate the decannulation of invasively managed ventilator users to more desirable noninvasive aids.4
Comprehensive surveys on HMV have been carried out in Europe, North America, Chile, and Japan,5 but not in Korea. Based on our previous 10 years of experience, therefore, we aimed to describe HMV and the role of PM&R in optimizing it.
MATERIALS AND METHODS
Patients with chronic respiratory failure requiring HMV were included in the study. We retrospectively reviewed their data from March 2000 when we first adopted systemized PM&R intervention to the HMV program at Gangnam Severance hospital until December 2009.
The management status of patients with HMV
The following parameters were investigated; basic demographic characteristics of all patients, causes of chronic respirator dependence, type and mode of mechanical ventilator use, tracheostomy mechanical ventilation (TMV) vs. NIV use and any transition between them. We supplemented medical record reviews with telephone surveys of those with incomplete records or who had been lost to follow-up for over two years. For patients who were decannulated of their tracheostomy tubes, we analyzed the data before and after the decannulation. A follow-up survey was performed in October 2010 to explore any changes in HMV status.
Pulmonary function evaluations
1) Forced vital capacity (FVC) was measured in sitting and supine positions using a spirometer (Micro™ spirometer; CareFusion 232 Ltd., Chatham, UK). The highest of 3 attempts was recorded as the FVC. We calculated predicted FVC values (FVCpre) based on age and height.6
2) The maximal inspiratory pressure and maximal expiratory pressure measured in mouth in sitting position with an effort sustained for at least 1 second (MicroRPM; CareFusion 232 Ltd., Chatham, UK) to gauge inspiratory and expiratory muscle strength, respectively. The highest value of 3 or more attempts was used.
3) Peak cough flow (PCF) was measured by a peak flowmeter (ASSESS®; Health Scan Products Inc., Cedar Grove, NJ, USA) with the patient coughing as hard as possible and the highest value of 3 or more attempts was recorded.
4) Assisted PCF (APCF) was measured by the same peak flow meter, but the inspiratory phase was augmented by the subjects air stacking,7 and the expiratory phase assisted by application of an abdominal thrust.8
5) The ventilatory status was monitored by arterial blood gas analysis (ABGA) or by monitoring oxyhemoglobin saturation (SpO2) and end tidal carbon dioxide (EtCO2) via oximetry and capnometry (Microcap plus, Oridion Ltd., Jerusalem, Israel) just before HMV prescription, while using mechanical ventilation. For those who could not perform 1)-4) due to intubation or a tracheostomy tube as well as intolerance of breathing with the tube transiently capped for the measurement, the same test was performed after the decannulation or extubation.
Statistical analysis was made by SPSS 13.0 for windows version (SPSS Inc., Chicago, IL, USA), paired t-test was used to find the statistical significance between FVC in sitting and supine position in NMD groups, and Wilcoxon signed rank test was used for the comparison of non-NMD groups.
Application of NIV
When patients presented with subjective symptoms of hypoventilation or when ventilatory abnormality was suspected from the result of a single daytime ABGA or EtCO2 and SpO2 measurement, overnight noninvasive monitoring was performed to detect latent hypercapnea. Initial NIV application was considered when patients showed elevated nocturnal EtCO2 levels (>45 mm Hg) with or without multiple nocturnal SpO2 below 95% on serial overnight monitoring. Nasal interfaces (Goldseal nasal mask, Respironics, Murrysvill, PA, USA) or oronasal interfaces (Performa Track™ SE mask, Respironics, Murrysvill, PA, USA) were used for the transition from TMV to NIV. Candidates for decannulation and transition to NIV had the ability to attain APCF >160 L/min and had minimal or no dysphagia or dysarthria before intubation or tracheostomy. All TMV patients who fulfilled the above criteria without ongoing lung parenchymal lesions were included once for the transition training, and the decannulation processes were performed as previously described.9 Patients who could not follow commands or did not cooperate with training in NIV or with assist coughing were excluded from the consideration for decannulation.
RESULTS
Pulmonary function evaluations
Of the 413 patients, we analyzed the data of 306 patients whose pulmonary function tests at initial HMV application were available (Table 3). The results of pulmonary function assessment were used to determine when and how HMV was used.
Methods of HMV
Of the 284 patients who initially used NIV, NMD accounted for the majority (97.5%). On the follow up, 233 patients were still using NIV, and of 46 patients who switched to TMV, 42 were amyotrophic lateral sclerosis (ALS) who could not tolerate NIV any further because of stridor occurring from upper airway spasticity and paralysis (Table 4). One spinal muscular atrophy (SMA) patient started nocturnal NIV, but underwent tracheostomy due to extubation failure after scoliosis surgery. After transition training of NIV, he succeeded in decannulation once again, and is using nocturnal NIV. One spinal cord injury (SCI) patient developed hypoxic brain injury, and 2 myopathy patients underwent emergency tracheostomies during respiratory arrests.
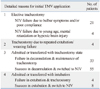
One hundred twenty-nine patients started HMV invasively; 121 were using TMV, and the other 8 patients were extubated to NIV (Table 5-1). Two major causes of transition failure to NIV were accompanying bulbar muscle weakness and insufficient cooperation due to either young age (<7 yrs old) or mental retardation (Table 5-2). Details of the 63 initial TMV users who succeeded in decannulation are described in Table 6-1 and 6-2, and flow diagram of HMV application by lapse of time is described in Fig. 1.
The most frequently prescribed mode of HMV was assisted controlled ventilation based on volume cycled systems. Although there were initially 42 bilevel positive airway pressure (BiPAP) and 3 continuous positive airway pressure users, all except for 4 patients [2 myotonic muscular dystrophy (MMD), 1 SMA and 1 cerebral disease] who were using BiPAP were switched to assist control mode ventilation on prescription. Major cause of the mode change was either unsatisfactory ventilation results or patients' maladjustment to the preset modes.
At initial HMV application, 231 patients used nocturnal HMV, 125 patients used HMV nocturnally plus some daytime, and 57 patients required near full time HMV (≥22 hours). When the application time was reinvestigated in 2010, 16 patients no longer used HMV; 5 voluntarily quitted the use of HMV against advice, 11 totally weaned off HMV. Changes of HMV dependent hours in each diagnostic group are described in Table 4 and 5.
Management of patients with HMV
Among the HMV users investigated, only 96 patients [ALS 41, Duchenne muscular dystrophy (DMD) 40, SMA 2, other myopathy 13] received regular PM&R interventions including serial pulmonary function evaluations and ventilation monitoring. Eighty-six patients from this group started NIV, and 10 initially used TMV. Of the 86 NIV users, 68 were maintaining NIV, but 18 (ALS 16, MMD 1, DMD 1) were switched to TMV during follow-up periods (Table 4 and 5-1). Nine initial TMV users, except 1 SMA who succeeded in decannulation, were still using TMV at the follow-up.
DISCUSSION
Although a few studies exist on the management status of ventilatory impairment in NMDs,10,11 the present study is the first report which contains detailed information of different disease groups in relation to HMV in Korea. Previous surveys revealed variations between countries in the proportion of lung and neuromuscular patients ventilated, preferred ventilator and interface types.1,5 The most striking difference of our result is higher proportion of NIV in NMDs, most likely due to a large number of patients with regular PM&R check-ups. NIV is currently identified as a preferred ventilation strategy and recommended only if the basic requirements such as proper swallowing function, basic cooperation, and ability of self-expectoration are fulfilled.11,12 Despite the advantages, ventilation via tracheostomy still accounts for the highest percentage in NMDs worldwide.1,5 Total number of progressive NMD patients is also high in this study. Improved availability to HMV since the introduction of a public subsidy for NMDs, and the characteristics of a center at which the survey was conducted may contribute to this.
PM&R intervention for patients with chronic respiratory failure mainly consists of regular monitoring of ventilation and pulmonary function, maintenance of pulmonary compliance, optimization of sputum clearance, and timely application as well as transition training to NIV. In the present study, only 96 patients received regular PM&R check-ups before the onset of subjective symptoms or overt respiratory failure occurred. Although 10 patients initially used TMV, 9 were severe bulbar ALS patients. In contrast, 62 of the decannulated patients (98.4%) did not benefit from early PM&R check-ups before developing respiratory failure. Although they finally succeeded in decannulation, patients could have avoided unnecessary invasive procedures which caused pain, increased medical costs and hospitalization if they had been optimally managed at the onset.
Of the 413 patients, 293 turned out to be alive at the follow-up in 2010, whereas 120 patients were either expired or presumed to be dead; 118 of them were NMDs (ALS 86, DMD 15, other myopathies 14, SMA 3), and 2 were non-NMD patients (1 SCI, 1 brain stem glioma). Specific causes of death were not fully investigated in this study. In spite of prolonged median survival of these patients, respiratory failure comprised the major cause of death to certain NMD patients, especially in ALS.13 As proven in recent literatures,14,15 aggressive use of continuous NIV and MAC can result in more favorable outcomes and better survival.
A growing population of patients exist who have chronic respiratory failure due to conditions such as NMDs, SCI, or lung parenchymal disorders, and who require either tracheostomy or mask ventilation.1,8 However, the lack of concrete local guidelines and shortage of experienced physicians specialized in PM&R interventions are the main obstacles to extensively employ the management. Furthermore, the availability and practical details of complex respiratory support at home involve many variables.5
Even though this study includes a large number of HMV users, the results cannot fully reflect general status of Korea. Future collaboration with several district university hospitals will be necessary to expand the results.
In conclusion, a thorough understanding and application of PM&R interventions can be of value in improving the care and quality of life for patients with long-term HMV.








 XML Download
XML Download