

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Autism spectrum disorder (ASD) is a pervasive neurodevelopmental disorder that according to the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, text revision (DSM-IV-TR) is characterized by qualitative impairment of social interaction, communication and repetitive and stereotypical behavior with onset prior to 3 years of age. There is no significant change in DSM-V (DSM, 5th edition) but the fact that the terms 'social interaction' and 'communication' are integrated in the term 'social communication' highlights the connectivity between the two terms compared to the previous diagnostic category of DSM-IV.1 Social and communication difficulties in ASD tend to overlap, making it difficult to distinguish them.
Some retrospective studies have identified that autistic toddlers can be differentiated from normal developing toddlers in reference to their social communicative behaviors by the age of two.2,3,4 As a result, the following distinguishing features of autistic toddlers from the normal were observed: abnormal eye contact, requesting behaviors, inappropriate use of emotions, decreased initiation of joint attention, and low level of communicative gestures.5,6 Prospective studies showed that toddlers at high risk of autism later diagnosed as ASD demonstrated overt differences in early social communication compared with those who did not develop into ASD. Differences were observed in certain categories, such as social interest and affect, social smiling, orienting to name, imitation, and atypical eye contact.7 Other prospective studies identified that toddlers later diagnosed as ASD showed greater developmental delay in social gestures and babbling than High Risk infants without ASD.8
On the other hand, the developmental language delay (DLD) group is similar to ASD in terms of reduced language skills, but the difference can be seen in social behavior. According to several studies, infants with developmental delay and those with ASD showed no significant difference in the type and frequency of social gestures from 9 months to 12 months.9,10 Evidence supports the premise that there is almost no improvement in social reference and gaze shifting in ASD toddlers as time passes, but those with developmental delay have shown improvement by age 2.5 Clifford, et al.11 observed that toddlers with ASD showed reduced sharing of positive affect and interest in peers compared to toddlers with a developmental delay. There seems to be a clear difference in social behavior by age 2 between toddlers with delayed development and ASD. It should be noted that the difference in language profile between the two groups may play an important role in explaining the different developmental trajectories.
The results of previous studies have shown considerable variation in the language ability of individual ASD children.12 However, the ASD group showed a consistent impairment of language ability associated with social area, with unique features such as echolalia, scripted speech, and unusual prosody, which is clearly distinguished from other developmental disorders.13
Furthermore, according to the DSM-IV, language development of children with Asperger's disorder is not delayed, but there are severe impairments in pragmatic language, causing deficits in the social area.14 Through follow-up of 8 years it was found that verbal skill is the most powerful prognostic factor of social adaptive functioning of ASD.15 Not only is impairment in language ability the earliest symptom of ASD individuals detected by the parents, but it is also closely related to the long-term social function.16
Generally, receptive language skills are usually much more advanced than expressive language skills in normally developing children.17 However, some studies found relatively greater impairment in receptive language skill over expressive language skills in toddlers and children with ASD.18,19
The unique feature of ASD such as echolalia, scripted speech, and unusual prosody reflects the decrease in receptive language ability compared to the relatively conserved expressive language ability in conversations, which is clearly distinguished from other developmental disorders. Furthermore, these unique features may explain the deficits of social behavior in respect of being likely related to the children's overall lack of social responsiveness.20,21
The objective of the present study is to investigate the different pattern of receptive and expressive language abilities in toddlers with ASD and DLD across three age groups. We hypothesized that toddlers with ASD will show a significant difference in the language profile compared to those with DLD, and speculated that these differences in language profile will be apparent even in early childhood in Korea.
MATERIALS AND METHODS
Participants
The participants were 166 toddlers between the ages of 20 months and 50 months who visited the clinic of child and adolescent psychiatry in Severance Hospital (Yonsei University College of Medicine, Seoul, Korea) from December 2010 to January 2013. ASD and DLD were diagnosed by a child and adolescent psychiatrist, using the criteria of the DSM-IV-TR. All participants in this trial were Korean, and all family members were proficient native speakers of Korean. The Institutional Review Board of the hospital approved this study protocol (approval number: 4-2013-0790).
Demographic characteristics
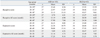
The ASD group consisted of 103 toddlers (17 female) between 20 and 50 months of age (mean age 35.6±7.3) and the DLD group consisted of 63 toddlers (9 female) aged between 22 and 45 months (mean age 34.1±5.8). There was no significant difference between the groups in terms of age and gender. The number of toddlers with ASD and DLD aged between 20 and 29 months were 27 (mean age 26.84±1.82) and 15 (mean age 26.8 ±2.3), respectively, while between 30-39 months there were 37 (mean age 33.8±2.9) and 34 (mean age 34.3±3.2). There were 39 (mean age 43.6±2.8) and 14 (mean age 41.6 ±1.8) toddlers aged 40-49 months with ASD and DLD. The age and gender between ASD and DLD showed no significant difference as well as in mean age across all three age groups (Table 1).
Language assessment
For the language assessment in this study, we used SELSI, the Korean semi-structured and examiner-rated scale grading language developmental age between 4 months and 35 months. This is the one and only comprehensive assessment tool for communication and language for the level of toddlers under age of 3. The language levels of ASD and DLD patients are lower than normally developing toddlers. Therefore, regardless of participants' real age, if the level of language skill is between 4 month and 35 month, SELSI can evaluate participant's language level pretty well. There are 4 questions for each 14 specific age groups, and for both receptive and expressive language profile. As a result, the SELSI consists of 56 questions for receptive language and 56 questions for expressive language, totaling 112 questions. Based on the reference data, language development-for-age percentile and age-equivalent scores are calculated.
The reliability and validity of SELSI were confirmed in previous studies in Korea.22 Items of the SELSI were developed from various literatures about the language development and disorder. The items are pilot tested by 233 normal Korean toddlers and then applied to 1090 normal Korean toddlers. SELSI screens the toddlers who are at risk of language disorders. The items of the SELSI were arranged based on difficulty level, % of correct responses, and discriminative level for the equivalent age. There was no sex difference among the items for reliability analyses, internal reliability and test-retest reliability were calculated by Cronbach α with one week interval in both receptive and expressive language test were above 0.98. Correlations between the first and second tests with one week interval in 14 participants were 0.996 in receptive and 0.998 in expressive language tests.
Analysis procedures
Raw SELSI receptive and expressive score of each group were converted into age equivalent score (AE) in order to evaluate the appropriate comparisons. AE is equivalent to the average SELSI score of normal toddlers by month age. For example, 15 Raw SELSI score is equivalent to the average SELSI score of 9 month aged normal infants. Therefore 15 Raw SELSI score can be standardized by 9 AE. For this reason, SELSI can be a useful tool to assess the language function of the toddlers about level of 35 months, regardless of the real age of the participants. Language dominant type was determined by dividing the receptive AE score by the expressive AE score. We categorized participants with a calculated score less than 0.9 as 'expressive language dominant type,' and those with a calculated score greater than 1.1 as 'receptive language dominant type.' Participants with a score between 0.9 and 1.1 were grouped as 'non-dominant type.' All participants of any type in ASD and DLD group were recorded lower AE score than that of the typically developing toddlers.
All data were parametrically distributed and were analyzed by independent t-test for a by-group comparison of demographic characteristics. Chi-square test was used for type-by-group and type-by-age-group comparisons. A linear-by-linear association test was used to analyze the proportion of expressive language dominant type among the age-groups. All data were analyzed by SPSS 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
As noted, each ASD and DLD group was divided into three subgroups based on age (20-29 months, 30-39 months, 40-49 months), with no significant differences in the mean age of each subgroup. All subgroups in both groups reported lower receptive and expressive AE scores than expected for typically developing toddlers. Independent t-test was performed to compare the raw scores of receptive and expressive language profile as well as the AE scores. As a result, significant differences were observed in the raw receptive language score between the groups across all three subgroups, as well as in the receptive AE score. However, no significant difference was found in expressive score and expressive AE scores. Therefore, it was determined that the receptive language ability of the DLD group is superior to that of the ASD group (Table 2). The results were in agreement with several previous studies.9,23 As explained in the method, we divided expressive AE scores by receptive AE scores to determine each individual's language dominant type as either receptive language dominant type, expressive language dominant type, or non-dominant type. Significant differences in the proportions of dominant types between ASD and DLD were observed. Expressive language dominant type was found to be in largest proportion in the ASD group, while on the other hand, receptive language dominant type was in greatest proportion in the DLD group. The proportion of expressive language dominant type in ASD was approximately 4 times greater than in DLD, showing more impairment in receptive language function in the ASD group (F=2, p<0.001) (Fig. 1).
Distribution of dominant types in each age group was observed, and there was a significant relation between the diagnostic group and the type. In the 20-29 months subgroup and the 30-39 months subgroup, expressive language dominant type (ED) occupied the largest proportion in the ASD group. On the other hand, in the DLD group, receptive language dominant type (RD) was found to be in the largest proportion (20-29 M: F=2, p<0.002; 30-39 M: F=2, p<0.001). In the 40-49 months subgroup, there was no relationship between the diagnostic group and type (Fig. 2). Moreover, with decrease in age, a higher proportion of expressive language dominant type was shown in ASD than in DLD by linear-by-linear association (F=1, p<0.006) (Fig. 3).
DISCUSSION
This cross-sectional study was conducted with a sample of 166 subjects between 20 and 50 months of age who had visited the hospital due to DLD or social function impairment, and had been diagnosed as either ASD or DLD. The study assessed and compared the receptive and expressive language abilities in two diagnostic groups: ASD and DLD. The results showed that ASD group had relatively more impairment, to a statistically significant extent, in receptive language abilities when compared to the DLD group. This pattern of impaired receptive language was more apparent in younger age groups. Our findings suggest that ASD and DLD groups may have different developmental trajectories, and early differentiation of ASD from DLD will be closely associated with better prognosis for ASD. Therefore, it is important to distinguish between the two groups in the early stages. This is emphasized in this study by clearly showing the difference in receptive and expressive language subabilities between ASD and DLD groups and the more distinct difference seen in the younger age groups between 20 and 29 months. The reason why this age trend appears is unclear. However, we can guess these results came from the treatment effect from earlier intervention. If the symptom of ASD can be found earlier, the patient can get proper treatments earlier and then the symptom may be milder with intervention. Actually, there are some reports that intensive early intervention can decrease the number of non verbal status with ASD.24 There is another study that children received early intervention show less autistic later.25 In the line of these, the importance of early ASD detection is emphasized.
While recent studies related to ASD have focused on the difference between normal and delayed developmental groups using receptive and expressive language scores, this study examined receptive and expressive language scores for each subject to identify the difference by analyzing data obtained from ASD and DLD groups. Although a large individual variation was observed in language abilities ranging from normal to severe impairment in the ASD group, receptive and expressive language abilities of both ASD and DLD children are generally considered to be lower than the abilities of normal.26 Our study also confirmed this trend. In our study, the level of language development of all participants is lower than the typical developing toddler of the same age. The term 'dominant type' in our study refers to relative superiority between receptive and expressive language ability of our participants.
Many previous studies that compared language abilities between preschoolers with ASD and the typically developed have confirmed that preschoolers with ASD presented a relative lack of receptive language over concurrent expressive language.18,27,28 A study conducted by Ellis Weismer, et al.23 that compared early language abilities in toddlers with ASD and toddlers with developmental delay also showed that toddlers with ASD had relatively more severe receptive than expressive language delays. However, in contrast to "preschoolers" with ASD, the atypical pattern observed in "toddlers" with ASD group may be associated with certain language measures. According to previous studies, some language measures cannot find atypical pattern in "toddlers" with ASD. Even if an atypical pattern is observed, individual gaps were large to summarize. The present findings were consistent with the findings of previous studies that examined and compared receptive and expressive language abilities in ASD and DLD groups.27
Unlike other research, we compared the abilities between the two groups following the examination of impairments in an individual's receptive and expressive language abilities. Thus, the pattern of having more severe impairment in receptive language abilities compared to expressive language among toddlers with ASD was more clearly shown in this study.
In this study, relative comparison of individual's expressive-receptive language abilities was limited to the language area. However, considering that language comprehension is a basic element of social communication, comparison of expressive-receptive language abilities in toddlers with language impairment can be an important measure for ASD diagnosis and evaluation. Correlation between expressive-receptive language ability pattern and ASD diagnostics tools such as Autism Diagnostic Intervie, Revised (ADI-R) and Autism Diagnostic Observation Schedule (ADOS) needs to be investigated further in the future.
Echolalia, which is the meaningless repetition of the words of others' language and is characterized as being extremely literal and automatic, is commonly observed in ASD subjects. These show the characteristics of language abilities in the ASD group, which include relatively well-preserved expressive language ability but impaired receptive language ability.29,30 Language comprehension is used as a subscale of language ability, and at the same time is an essential element of social reciprocity since it allows understanding of another person's intention.
Theory of mind (TOM) is an ability to infer what another person is thinking or feeling, and it is critical for development of social skills. Several functional Magnetic Resonance Imaging studies indicate that posterior superior temporal sulcus is an important part of TOM that is involved in interpreting others' mental states from cues. Boddaert, et al.31,32 reported that hypoactivation of the posterior superior temporal sulcus is observed during speech perception. This area is called the Wernicke area, which is known to be involved in language comprehension. This implies that the area of communication and social interaction are closely related to each other, and further research is necessary to explain the association between language comprehension in ASD group and deficit in the social area.
There are several potential limitations to this study. As mentioned before, firstly, toddlers were clinically diagnosed as either ASD or DLD by a child and adolescent psychiatrist, but ADOS and ADI-R were not used to confirm the diagnosis. Secondly, a smaller number of toddlers were diagnosed with DLD when compared to the number diagnosed with ASD. Lastly, since the study was a cross-sectional comparison, it is not certain that the difference in expressive language abilities were more apparent in toddlers between 20 and 29 months was due to a particular pattern that could be observed during this specific period. Longitudinal studies examining various language-related measures are necessary. However, to the best of our knowledge, this study provided valuable results since it is the one of first studies examining language development in toddlers with ASD.
In conclusion, the ASD group showed more clinically significant impairment of receptive language abilities when compared to the DLD group. This difference in language abilities was most apparent in toddlers between 20 and 29 months. Since language comprehension is a basic factor that influences ASD social communication, relatively more severe impairment in receptive language in toddlers with ASD below 3 years of age could be an important component for early identification and early detection. In addition, regarding the point of view that early intervention of language impairment both ASD and DLD groups is critical and that the direction and the approach to language therapy of the two groups is different, results of current study could play a vital role. A longitudinal prospective cohort study examining language development process in toddlers with ASD is necessary in the future for further support.




 XML Download
XML Download