

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
When anesthetizing patients, achieving a precise return of consciousness (ROC) after anesthesia is an important component for successful anesthesia no less than inducing rapid and safe anesthesia.1 Recently, ambulatory anesthesia has been increasingly used to tailor the need of rapid discharge after an outpatient's procedure which is simple and can be done for a short time. Rapid and safe recovery from anesthesia is necessary for successful treatment in the ambulatory setting. In dental practice, mentally disabled patients are subject to general anesthesia for dental treatment because of their poor cooperability.2,3,4 They seem to show different recovery profiles compared to normal patients in our experiences. However, without information on the pharmacodynamic features of mentally disabled patients, we cannot compare inhaled anesthetic concentrations during emergence precisely compared to normal patients. Therefore, population pharmacodynamics modeling incorporating mental difference as a covariate could be clinically useful for investigating the difference of emergence after general anesthesia.
We aimed to investigate the relationship between end-tidal sevoflurane concentration (Etsevo) and ROC in both normal pediatric patients and mentally disabled patients undergoing general anesthesia with sevoflurane and to identify the covariates (especially mental ability) in the pharmacodynamic relationship between Etsevo and ROC.
MATERIALS AND METHODS
Subjects
We enrolled pediatric patients aged 3 to 15 years old scheduled for dental treatment under general anesthesia in the study. Among them, we included patients diagnosed with severe mental disability in the department of pediatrics and American Society of Anesthesiologists (ASA) class 1 patients with intact mental ability into the study. The other exclusion criteria were as follows: those who have history or adverse reaction to anesthetic medication, those who have cardiac, pulmonary, hepatic or renal disease. The study was approved by the Institutional Review Board of the Seoul National University Dental College (S-D20121007). The study was exempt from informed consent by the ethics committee since the study protocol was a routine part of general anesthesia.
Anesthesia protocols
All patients received the same anesthesia protocols. After being transferred to a dental chair, they were connected to a breathing circuit through a tightly sealed facial mask. Sevoflurane at a concentration of 8 vol % was administered with a flow of 6 L/min. We defined loss of consciousness (LOC) as loss of the response to verbal command.5 We also considered stop crying as a behavior of LOC during sevoflurane administration. After achieving LOC, assisted ventilation was attempted until they stopped to breathe spontaneously. After intravenous cannulation, vecuronium at a dose of 0.1 mg/kg was administered as a neuromuscular blockade. After confirming complete neuromuscular blockade, nasotracheal intubation was performed. Next, dental treatments were performed under general anesthesia at the discretion of the dentists. Age adjusted 1 minimum alveolar concentration (MAC) sevoflurane was administered combined with 50% nitrous oxide during dental procedures.6 All efforts were made to maintain normothermia during dental procedures. After the treatments, sevoflurane administration was stopped. Neuromuscular blockade was reversed with the dosages selected depending on their weight of glycopyrrolate (0.01 mg/kg up to 40 kg, 0.4 mg over 40 kg) and pyridostigmine (0.25 mg/kg up to 40 kg, 15 mg over 40 kg). We controlled and assisted their respiration with 100% oxygen with a flow of 6 L/min to keep the end-tidal carbon dioxide in the range of 30-35 mm Hg for maintaining the condition of ventilation consistently as much as possible during emergence from sevoflurane anesthesia. ROC from anesthesia was defined as the recovery of the observer's assessment of awareness/sedation (OAA/S) score 3 defined as the response of after name is called loudly or repeatedly.7 At the end of surgery and at ROC, Etsevo was continuously recorded with a software (Datex-Ohmeda S5™ Collect; GE Healthcare, Helshinki, Finland) and ROC was observed by an investigator every 15 seconds. The patients were extubated when they gained consciousness to the pre-anesthesia level from sevoflurane anesthesia and achieved the reversal of neuromuscular blockade assessed using a peripheral nerve stimulator. The recovery of neuromuscular blockade was evaluated as the train of four count or clinical signs (ex. head elevation, leg elevation, the return of adequate tidal volume). The durations of sevoflurane administration, anesthesia, and dental treatment were recorded. We also recorded hemodynamic variables [systolic, diastolic, and mean blood pressure (BP)] from anesthesia record. The observed ROC was recorded as 0 for unconscious state or 1 for conscious state. A sigmoidal Emax model as described below was used to derive the relationship between Etsevo and the probability of ROC:

where P indicates the probability of ROC from anesthesia, C is the Etsevo, C50 is the Etsevo associated with 50% probability of ROC, and γ is the steepness of the Etsevo-response curve.
Statistical analysis
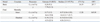
As previously reported,7 we estimated the population base model parameters with the use of the option "LIKELIHOOD LAPLACE METHOD=conditional" incorporated in the Nonlinear Mixed Effects Modeling (NONMEM) software (version VII; GloboMax, Hanover, MD, USA). The inter-individual random variability of C50 and γ was estimated using an exponential error model (Appendix 1). The population model parameters were derived from NONMEM analysis where the objective function value, a statistic proportional to negative twice the log likelihood of the data, was the lowest. After obtaining the population base model, a forward inclusion and backward elimination approach was used in consecutive NONMEM runs to find out the relevant covariates among the covariates (age, sex, height, weight, anesthetic time, and dental procedure time) as previously described.8 The difference in the minimum value of the objective function between two nested models approximately follows a chi square-distribution and could therefore be used to investigate statistical significance [chi square statistics equals to 3.84 at the level of significance (p<0.05) with one degree of freedom]. A non-parametric bootstrap procedure was performed for internal validation using Perl-speaks-NONMEM (PsN) (version 3.6.2, http://psn.sourceforge.net). In brief, the original data set was randomly sampled to generate 2000 bootstrap replicates. We obtained the 95% confidence interval of the nonparametric bootstrap replicates and compared final model parameter estimates with them. Also we performed a randomization test to test whether the selected covariate is a significant one using Wings for NONMEM (version 7.2, http://wfn.sourcefourge.net). We randomly permuted a significant covariate in the original data set 1000 times. We calculated the objective function value (OFV) of the model without the covariate parameter relationship. We considered the covariate as a significant one when the difference between the median OFV calculated from the randomization test and the original OFV was more than 3.84.
RESULTS
Twenty patients that met the inclusion criteria were enrolled into the study. Among them, 10 patients were mentally disabled persons. They were severely mental retarded with the impairment of daily living activities irrespective of their primary causes of neurologic disturbances. All patients underwent restorative treatment for dental caries under volatile anesthetics induction and maintenance anesthesia with sevoflurane. Table 1 shows their demographic characteristics, the duration of dental procedures and sevoflurane anesthesia, which were not significantly different between two groups. Hemodynamic variables (systolic, diastolic, and mean BP) were not significantly different between the two groups (data not shown).
A total of 476 measurements were used to build a pharmacodynamic model. Table 2 lists the estimated model parameter of the basic and final model. To investigate whether mentality have a significant effect on C50 value at ROC, this was included as a covariate in C50. This inclusion significantly decreased the minimum value of the objective function from 207.7 to 185.8. We also included mentality as a covariate in γ. This inclusion significantly improved the performance of model, mentality included in C50 as a covariate. The minimum value of OFV was decreased from 185.8 to 165.1 by more than 3.84 (p<0.05). The difference between the median OFV calculated from the randomization test and the original OFV was more than 3.84 (the original OFV=165.1, the median OFV after randomization test=205.6), confirming that mentality is a significant covariate. Other covariates including age, sex, height, weight, anesthetic time, and dental procedure time did not improve the performance of the selected model significantly. Table 2 lists the estimated model parameter of the finally selected pharmacodynamic model and bootstrap estimates. The relationship between the probability of ROC and Etsevo are plotted in Fig. 1. We also simulated the effect of mental ability on the relationship between Etsevo and the probability of ROC using the final population parameters. The selected C50 and γ value in normal and mentally disabled patients upon computer simulation were the final model parameters. The pharmacodynamic relationship between Etsevo and the probability of ROC in accordance with mental ability using the final population parameters are presented in Fig. 1.
DISCUSSION
In this study, we found that mentality can influence ROC during emergence from sevoflurane anesthesia. Also, preoperative mental ability was proved to be a significant factor influencing γ as well as C50 in the quantitative relationship between Etsevo and ROC. To our best knowledge, this is the first clinical study to investigate the dose-ROC relationship during emergence from anesthesia based on pharmacodynamic modeling with the inclusion of mental ability as a covariate.
In clinical practice, it can be advantageous to apply the predicted Etsevo for ROC in mentally disabled patients rather than a population-based average Etsevo value. In this study, large inter-individual variability of Etsevo for ROC could be explained by incorporating the mental ability as a covariate in nonlinear sigmoid Emax model. A non-linear sigmoidal Emax model has an advantage over other statistical approaches in estimating the quantal response.9,10 Not only the C50 value but the steepness of the concentration-effect relationship (γ) can be estimated from this method, which can make the selection of significant covariates easier in comparison to logistic regression. And we can predict the response of ROC at a certain Etsevo more accurately using non-linear regression analysis.
The C50 for ROC in this study is equivalent to MAC-awake value previously reported. According to our results, the typical C50 value of Etsevo for ROC in normal pediatric patients was 0.37 vol %, which was considered as a low value of C50 for ROC because MAC-awake value of sevoflurane was 0.6-0.67 vol % for healthy adults11,12,13 and 0.78 vol % for healthy children,14 respectively. It is unclear why our value of C50 is lower than MAC-awake value reported in the previous reports, but this difference may be attributed to the difference of methodological approach to calculate C50 value. In this study, we collected dissipating Etsevo rather than stable Etsevo during emergence, which could represent sevoflurane concentration in brain, described in Kihara, et al.14 The observed Etsevo would be lower than actual brain tissue concentration of sevoflurane due to hysteresis phenomenon during decreasing phase of sevoflurane concentration. However, our results may be more applicable in clinical practice because stepwise decrement of sevoflurane administration is rarely used during emergence.
It is notable that mentally disabled patients emerged at lower Etsevo compared to normal patients. This result suggests that patients with mentally disabled patients are more sensitive to the anesthetic action of volatile anesthetics. The anesthetic requirement is reported to be increased due to the inhibition of glutamate transporter crucial in regulating a major excitatory neurotransmitter.15 It can also be speculated that the requirement of volatile anesthetics may be decreased when the brain's activity is inhibited. Dosing strategy of inhalational agents based on data of normal population can result in unnecessarily deeper level of anesthetic in the mentally handicapped persons. The ratio of MAC-awake to MAC for sevoflurane is known to be within the range of 0.31-0.38.15 We may also predict Etsevo for maintaining adequate depth of anesthesia if the ratio of MAC-awake to MAC for sevoflurane can also be applied to the mentally disabled patients. The requirement of anesthetic gas concentration for a certain anesthetic depth in mentally disabled patients may be lower than that in normal patients, although further pharmacodynamic approach should be investigated.
From a non-linear regression analysis, we found that the value of γ, indicating the steepness of return of consciousness, was smaller in mentally disabled patients than in normal patients. This indicates that mentally disabled patients may recover more slowly and take a longer time to discharge from the hospital compared to normal patients, which is accord with previous other report.16 Hence, more attention with close monitoring is necessary for mentally disabled patients to reduce the incidence of re-sedation after initial ROC during emergence.8 It is unclear why recovery profile is different in accordance with mentality. However, it is possible to hypothesize that functional integration of the brain regions associated with ROC during emergence may be impaired in mentally disabled patients compared with mentally intact patients. Thalamocortical connection is closely related with the maintenance of consciousness.17 Recent studies have published that long projections between the thalamus and the cortex are disturbed in neuropsychiatric disorders.18 Impaired recovery of connection between the brain region involved in cognition in the disabled may affect the recovery from anesthesia, although further studies to clarify the exact mechanism of the delayed emergence in the disabled is needed.
In general, mentally disabled patients, especially pediatric patients, have a high incidence of dental problems.19 However, because most of them are uncooperative to dental treatment or even dental exam, their dental condition is usually worsened and finally renders them to be treated under general anesthesia. Most of dental treatment under general anesthesia has been performed in the ambulatory setting. In this sense, prolonged recovery from anesthesia can be a significant obstacle in performing ambulatory anesthesia for safety of mentally disabled patients. Therefore, it is of utmost importance to maintain an adequate level of anesthesia during dental treatment to prevent prolonging recovery and to facilitate the patient's recovery.
However, our study has some limitations. We regarded the recovery of OAA/S score 3 as ROC from anesthesia. There might be some bias in the observation of ROC during emergence since mentally disabled patients responded to the stimuli less promptly. However, neurophysiologic surrogate for consciousness in mentally disable pediatrics has not been properly evaluated. And this method such OAA/S score is still clinically acceptable during emergence from general anesthesia. In this study, we measured rapidly decreasing Etsevo rather than stable Etsevo during emergence. Therefore, the measured Etsevo may not reflect effect site concentration of sevoflurane due to hysteresis phenomenon. Although stepwise decrement of sevoflurane during the time long enough to allow the equilibrium of sevoflurane between the blood and the brain is rarely used during emergence, this administration technique makes it possible to evaluate the effect of mentality on pharmacodynamic relationship between the actual brain sevoflurane concentration and ROC. A further study should be needed to investigate whether mentally disabled patients recover from anesthesia at lower effect-site sevoflurane concentration.
In conclusion, mentality of patients significantly affects the pharmacodynamic relationship between Etsevo and ROC. Mentally disabled patients may have different recovery profiles reflected by lower sevoflurane concentration at ROC and γ value compared to normal patients. Clinicians should be cautious about the possibility of delayed recovery from general anesthesia for mentally disabled patients.


 XML Download
XML Download