

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Atrial fibrillation (AF) is the most common cardiac abnormality associated with ischemic stroke.1,2 Cardiogenic cerebral embolism is responsible for approximately 20% of all ischemic strokes. A number of other clinical features also increase the risk of stroke in patients with AF, including age, congestive heart failure (CHF), hypertension, diabetes, and prior thromboembolism. Left ventricular dysfunction, left atrial (LA) size, mitral annular calcification, spontaneous echo contrast, and LA thrombus on echocardiography also increase the thromboembolic risk.3
Pulmonary veins (PVs) are important structures for the generation and maintenance of AF and are the main targets of radiofrequency catheter ablation.4,5 In a previous report, PVs in patients with AF showed characteristic electrophysiological remodeling, including a lower mean voltage, slower conduction, and higher prevalence of complex signals.6 The positive relationship between LA size and AF is well recognized.7 Herweg, et al.8 demonstrated that AF patients with hypertension had more prominent PV dilatation than patients in the control group, and patients with persistent AF had more increased PV ostial diameter than patients with paroxysmal AF. It is likely that impaired left ventricular diastolic function is associated with a stretch-induced PV arrhythmia. PV dilatation may be the crosslink between LA enlargement and AF.9 However, despite the important role of PVs in the pathophysiology of AF, the association between PV remodeling and stoke in AF patients is poorly understood. This problem might be due to the limitations of current diagnostic tools. Notwithstanding, the latest multidetector computed tomography (MDCT) technology permits cardiac scanning with high spatial and temporal resolution and provides precise measurements (less than 1 mm) and three-dimensional information. Specifically, this technology can be used to obtain reliable information on the diameter, cross-sectional area, and estimated volume of the LA and LA appendage (LAA).
We hypothesized that specific features of PVs might be related to a higher stroke risk in patients with non-valvular AF. Accordingly, we analyzed the three-dimensional (3D) geometry and dimensions of LA structures, including PVs and LAA, using MDCT in AF and control patients. The purpose of this study was to determine the characteristics of remodeling of the LA and PVs in AF patients with stroke, which is different than that in patients without stroke. Finally, we also sought to determine if specific patterns and variants of PV anatomy might be predictive of stroke in non-valvular AF.
MATERIALS AND METHODS
Patient sample
The study protocol was approved by the Institutional Review Board of Severance Hospital, Seoul, Korea, and complied with the tenets of the Declaration of Helsinki. All patients provided written informed consent. From February 2008 to February 2011, 138 consecutive, non-hemorrhagic stroke with non-valvular AF patients who underwent cardiac MDCT were enrolled (AF with stroke group). The AF group included 138 age-sex matched non-valvular AF patients without stroke who underwent MDCT at the same period. The control group included 138 age-sex matched patients without AF and stroke who underwent concurrent MDCT. Similar to a previous study, only patients with non-valvular AF who were not taking anticoagulants at the time of their stroke, or at the time of cardiac MDCT for patients without a history of stroke, were included.10
The CHADS2 (Congestive heart failure, Hypertension, Age >75, Diabetes mellitus, and prior Stroke or transient ischemic attack) and CHA2DS2-VASc (Congestive heart failure, Hypertension, Age >75, Diabetes mellitus, and prior Stroke or transient ischemic attack, vascular disease, Age >65, female) scores of each patient were presented with and without points of stroke. CHF was defined as clinical heart failure (stage C or D) according to the 2009 Focused Update Incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults.11 Hypertension was defined as systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg at two or more visits or past medical history of hypertension. AF was classified as paroxysmal AF when an episode of AF was self-terminating within 7 days and persistent AF when an AF episode either lasted longer than 7 days or required termination by cardioversion, either with drugs or by direct current cardioversion.12
Cardiac MDCT
Contrast-enhanced cardiac CT scans were performed using a 64-slice MDCT (Somatom Sensation 64, Siemens Medical Solutions, Forchheim, Germany). A bolus of 60-80 mL iopamidol (Iopamiro 370, Bracco, Italy) was injected into the antecubital vein at a flow rate of 5 mL/s, which was followed by a 50-mL saline-chasing bolus at 5 mL/s. The start delay was defined as bolus tracking in the ascending aorta, and the scan was automatically initiated 5 seconds after reaching a threshold of 140 Hounsfield units. Scanning was performed using the following parameters: retrospective ECG-gated acquisitions, 80-120 kVp, 500-700 mAs depending on patient size, and 64×0.6 mm slice collimation. Scans were performed from the tracheal bifurcation to the diaphragm. The field of view was adjusted according to the size of the heart. Cardiac CT scans were reconstructed at the end-systolic and mid-diastolic phases using a slice thickness of 0.75 mm, an increment interval of 0.5 mm, and a medium-smooth convolution kernel of B36f. We used end-systolic CT images for this study.
Two radiologists (with four and eight years of experience in cardiac MDCT) calculated the LA and LAA volumes from CT images using imaging software (Vitrea, Toshiba, Japan). Each reader was blinded to the results of other examinations and to study groups. LA volumes were obtained by segmentation of the LA, and the software automatically calculated the volume. LA segmentation was performed using a semi-automatic approach by tracing the atrial contour to delete the pulmonary veins and the left ventricle in the 3D configuration and multiplanar images. LAA volume was obtained using the same method. The LAA and PV orifices were digitally transected by multi-planar reformatted (MPR) images.13,14 The pulmonary vein ostium was defined by the point of reflection of the parietal pericardium, as identified by intersection of tangents extending from the surface of the PV and the wall of the adjacent LA.15,16,17 The LAA and PVs were first identified in the transverse MPR of the 3D image and the image was reformatted along the center of the vein. The cross-sectional view of each vein was produced by creating a plane perpendicular to the transverse MPR image. This allowed for measurement of the short (D1) and long (D2) diameters of the LAA and PV orifices with electronic calipers in a plane perpendicular to the long axis of the LAA and PVs (Fig. 1). Because the LAA and PV orifices are elliptical in shape, a formula (0.785×D1×D2) was used as a surrogate value for this area.
PV dimensions change significantly between end systole and end diastole, and the ostia of the superior PVs are most vulnerable to dimensional inaccuracies. To overcome this problem, we used ECG-gated cardiac CT to provide a more precise method of PV dimensional measurement than non-gated techniques.18 LAA morphology was evaluated using the method described by Di Biase, et al.19 Thrombus was defined as a filling defect with an oval or convex shape, and blood stasis was defined as a typical triangular filling defect at the ventral side of the LAA, which appeared as fluid-fluid levels.20
Statistical analysis
Normally distributed continuous variables were reported as mean±SD and compared with Student's t-test. Categorical variables were reported as a percentage and compared with either Pearson's chi square test or Fisher's exact test. A multivariable logistic model was used to identify significant predictors of stroke. All potential confounders were entered into the model on the basis of known clinical relevance or significant associations observed in the univariate analysis. A receiver operating characteristic (ROC) curve was computed for the completed prediction model, and we chose a probability threshold for predicting the likelihood of stroke. The Statistical Package for the Social Sciences (SPSS, SSPS Inc., Chicago, IL, USA) was used for all statistical evaluations. All p-values <0.05 were considered statistically significant.
RESULTS
Patient characteristics
Patient demographic and clinical characteristics are presented in Table 1. Compared to age- and sex-matched AF patients without stroke, AF patients with stroke had a higher prevalence of persistent AF (34% vs. 59%, p<0.001) and hypertension (56% vs. 76%, p=0.001), as well as higher CHADS2 (1.4±1.1 vs. 1.7±0.9, p=0.006) and CHA2DS2-VASc scores (1.8±1.2 vs. 2.1±1.1, p=0.014).
Remodeling of the LA and LAA in AF patients with stroke
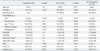
Table 2 shows a comparison of the LA, LAA, and PV features measured by MDCT between patient groups. The mean LA volumes for the control, AF, and AF with stroke groups were 101±25 cm3, 143±43 cm3, and 163±53 cm3 (p<0.001), respectively. The LA dimensions measured by transthoracic echocardiography also showed progressive enlargement from control group to AF and stroke group. Interestingly, AF patients with stroke (5.6±2.2 cm2) had larger LAA orifice areas than the control (3.5±1.3 cm2, p<0.001) and AF only patients (4.7±1.7 cm2, p<0.001). The percentage of volume ratio between LAA and LA in the AF with stroke group were larger than that of AF group (10.6±4.0% vs. 9.2±3.3%, p=0.011). These findings suggest progressive LA remodeling from control to AF with stroke groups.
Differences in enlargement of the left and right PVs in AF patients with stroke
Orifice areas of the LAA were larger in the AF group (4.7±1.7 cm2) than the control group (3.5±1.3 cm2, p<0.001). The AF group also had larger orifice areas of all PVs than control patients. The orifice areas of the LAA (5.6±2.2 cm2 vs. 4.7±1.7 cm2, p<0.001), left superior PV (3.8±1.5 cm2 vs. 3.4±1.2 cm2, p=0.019), and inferior PV (2.3±1.0 cm2 vs. 1.8±0.7 cm2, p<0.001) were larger in the AF with stroke group than the AF group. However, the orifice areas of the right PVs were not different between the AF only and the AF with stroke groups (Table 2, Fig. 2). We could not identify any differences in the LAA morphology between the three groups. There were no differences in PV type between the three groups.
Thrombus or blood stasis of LAA and left side PV enlargement
For all 276 patients with AF, thrombus or blood stasis were observed in 20 (7.2%) and 42 (15.2%) patients, respectively. While thrombus or blood stasis were observed in 51 (37.0%) AF patients with stroke, these complications were found in only 11 (8.0%) patients in the AF group (p<0.001). Table 3 shows a comparison of the clinical features and LA remodeling between patients with and without thrombus or blood stasis of the LAA. Patients with thrombus or blood stasis were older (67.3±7.2 years vs. 65.1±7.6 years, p=0.04), had a higher prevalence of persistent AF (82% vs. 36%, p<0.001), higher CHADS2 scores (1.8±0.8 vs. 1.5±1.0, p=0.006), and higher CHA2DS2-VASc scores (2.3±1.0 vs. 1.8±1.2, p=0.004) than those without thrombus or blood stasis. LA volume (190.2±52.8 cm3 vs. 141.0±41.4 cm3, p<0.001), LAA volume (17.1±8.0 cm3 vs. 13.9±6.8 cm3, p=0.01), and the left superior (4.1±1.8 cm2 vs. 3.5±1.2 cm2, p=0.007) and inferior PV orifices (2.5±1.2 cm2 vs. 2.0±0.8 cm2, p=0.003) were larger in patients with thrombus or stasis of the LAA. However, the orifice areas of the right superior and inferior PVs showed no differences between two groups.
Multiple logistic regression analysis of risk factors for stroke
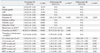
Multiple possible clinical predictors and CT measurements were assessed as univariate and multivariate risk factors for stroke (Table 4). The significant univariate risk factors of stroke were hypertension, diabetes mellitus, persistent AF, thrombus or blood stasis on MDCT, higher CHADS2 and CHA2DS2-VASc score, larger LA volume, and larger LAA, LSPV, and LIPV orifice areas. When adjusted for CHA2DS2-VASc score, the orifice areas of the left superior PV (OR 1.55, 95% CI 1.31-1.84, p<0.001), the left inferior PV (OR 2.66, 95% CI 1.96-3.61, p<0.001), and the LAA (OR 1.53, 95% CI 1.35-1.74, p<0.001) were independent risk factors of stroke with LA volume (per 10 cm3, OR 1.16, 95% CI 1.09-1.23, p<0.001) and thrombus or blood stasis seen on MDCT (OR 11.94, 95% CI 5.95-23.98, p<0.001). When the orifice areas were accounted for individual components of CHA2DS2-VASc score and the presence of thrombus or blood stasis on MDCT, ostial areas of left side structures, i.e., LAA, LSPV, and LIPV, were still independent risk factors of stroke but ostial areas of right side structures were not.
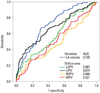
In the ROC curve analysis, LAA orifice area, LA volume, LIPV orifice area, and LSPV orifice area predicted stroke in AF patients with area under the curves of 0.739, 0.720, 0.674, and 0.587, respectively (Fig. 3).
DISCUSSION
Major findings
The main finding of this study was significant dilation of the left PVs and the LAA in AF patients with stroke. However, similar findings could not be demonstrated in the right PVs. Additionally, significant dilation of the left PVs and LAA was observed in AF patients with thrombus and blood stasis compared with those patients without these complications. Our study suggests that prominent anatomic remodeling of the left LA structures may play an important role in the occurrence of stroke in AF patients. To the best of our knowledge, this is the first study to show more prominent structural remodeling of left-side structures such as LAA and left PVs than right PVs in non-valvular AF patients with stroke.
Remodeling of the LA and LAA in AF
It is well known that the relationship between LA chamber enlargement and AF is complex and that structural changes may lead to persistence of arrhythmia. The Framingham heart study showed that the relative risk for the subsequent development of stroke was 2.4 in men and 1.4 in women for every 10-mm increase in LA size.21 This finding is consistent with the results of this study. Increased LA volume by every 10 cm3 was an independent risk factor of stroke in multivariate logistic analysis (OR 1.09, 95% CI 1.02-1.17, p=0.014).
LAA is an important source of emboli in 70-90% cases of AF.22,23,24,25 Embryologically, the LAA is a remnant of the primordial LA. The LAA lies anterior to the atrioventricular sulcus and is in close proximity to the left circumflex artery, the left phrenic nerve, and the left PVs.26,27 A study of postmortem and explanted hearts showed that atrial appendages from patients with atrial fibrillation have three times the volume of those in sinus rhythm.28 In this study, LAA dilation and enlargement of the LAA orifice were related to a higher risk of stroke. Previously, it was reported that the dilation of the LAA dimensions predict stroke in patients with AF.29 In our study, the LAA/LA ratio was significantly higher in patient with stroke than other groups (Table 2). Although the volume of both LA and LAA were larger in patient with thrombus/stasis, the ratio of LAA/LA was not significantly different between the two groups. However, previous studies demonstrated that the thrombus was not observed in 20-40% of AF patients with recent thromboembolism.30
Recently, Di Biase, et al.19 reported that patients with Chicken Wing LAA morphology are less likely to have an embolic event, even after controlling for comorbidities and CHADS2 score. This result is consistent with our results in that stroke incidence is lower when there is less remodeling of the LAA. However, we could not find a relationship between stroke and LAA morphology.
Prominent enlargement of left-sided LA structures in patients with stroke
In the AF group, atrial myocardium in the PVs was characterized by more severe discontinuity, hypertrophy, and fibrosis.31 However, PV remodeling has not been fully elucidated in AF patients with stroke. Interestingly, the ostia of left-sided PVs were larger in AF patients with stroke than in those without stroke. However, right-sided PVs showed no differences between the AF groups. Kim, et al.13 reported that the ostia of the left-sided PVs were more elliptical than right-sided PVs. Tsao, et al.32 investigated the change of PV by magnetic resonance angiography and showed that the diameter of LSPV was progressively enlarged from control group to paroxysmal AF and to chronic AF, but the diameter of RSPV was not significantly different between paroxysmal AF and chronic AF. In our study, the stroke group had a significantly larger number of persistent AFs; therefore, LSPV areas were larger in the stroke group than the AF only group; meanwhile, RSPV area did not show a significant difference between the two groups. The right superior PV passes behind the junction of the right atrium and the superior caval vein, and the inferior PV passes behind the intercaval area. Therefore, the orifices of the right PVs are directly adjacent to the plane of the atrial septum. These anatomic characteristics of the right PVs might have prevented further enlargement in AF patients with stroke. Tsao, et al. found no enlargement of inferior PV ostia in chronic AF, compared to paroxysmal AF or control group. However, the number of patients in their chronic AF group was only eight; therefore, the lack of significance may be due to insufficient power due to the small sample size. In our study, all four PV ostia showed significant enlargement in chronic AF, compared with paroxysmal AF (Supplementary Table 1, only online). This study is consistent with a previous study that reported PV enlargement in chronic AF. Additionally, this study showed that left PV and LAA enlargement is more common in AF patients with stroke than no-stroke.
This study also showed that the average area of the superior PV is larger than the area of the inferior PV within each group. This finding is consistent with previous studies that reported simultaneous dilation of the superior PVs and LA enlargement in patients with paroxysmal AF and chronic AF.32,33 However, although the superior PVs were larger in those patients with AF,32,34 when this was adjusted with the concomitant increase in LA size, this difference was not significant.32
In this study, the RSPV and RIPV ostial areas were larger in persistent than paroxysmal AF. However, the RSPV and RIPV ostial areas were not different between patients with and without stroke. This finding might be related with confounding factors such as smaller body mass index and slightly higher proportion of female patients in the stroke group.
Study limitations
Our study had several limitations. Although we found an association of increased ostial size of left side PVs and stroke, it is possible that the differences are reflective of inherent anatomical differences rather than structural remodeling. Because this study was performed as a case-control study, we could not show a progressive increase in the orifice areas in the same AF patient group. It would be better if the changes in LAA and PV orifice diameters were evaluated by serial CT scan. Another issue is whether left atrial appendage and left pulmonary vein enlargement is caused by atrial fibrillation or whether it is related to hypertension, diastolic dysfunction, or other cardiovascular diseases that are prevalent in stroke patients. A more detailed, prospective study is needed to address these issues.




 XML Download
XML Download