

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pancreatic cancer is one of the most lethal cancers. According to a recent report, about 15% of patients with pancreatic cancer survived 1 year after diagnosis, and fewer than 5% survived 5 years.1 Only 20% of patients with pancreatic cancer have resectable tumors at the time of presentation, with a long-term survival rate of approximately 20%.2,3 A much higher percentage (40% to 45%) of patients present with metastatic disease and have a median survival of only 3-6 months.4,5
Patients with locally advanced pancreatic cancer (LAPC) are an intermediate favorable prognostic group and are associated with a median survival of 6-10 months.4,6 Treatment for LAPC has evolved to consist of chemotherapy alone or in combination with radiotherapy. Although chemoradiation therapy (CRT) remains a treatment option, only a small number of randomized clinical trials have reported improved survival outcomes,7,8,9 and many have argued the value of radiation therapy (RT) for the subset of patients with LAPC due to the high rate of distant metastasis and subsequent poor survival outcomes even after successful local control.10
18F-fluorodeoxyglucose (FDG) positron emission tomography-computed tomography (PET/CT) is now widely used to assess many different types of malignancy, and several studies have demonstrated an important role of FDG PET/CT in staging, detecting postoperative recurrence, and evaluating treatment response in patients with pancreatic cancer.11,12 Other studies have shown that the standardized uptake value (SUV) of primary pancreatic cancer lesions measured on pretreatment FDG PET/CT scans can help to predict survival outcomes in patients with pancreatic cancer.12,13,14,15,16 Recently, PET/CT-based volumetric imaging parameters, including metabolic tumor volume (MTV) and total lesion glycolysis (TLG), have also been shown to be useful prognostic indicators for various neoplasms.17,18,19 However, few studies have evaluated volumetric parameters as prognostic factors in patients with LAPC.20 Moreover, while investigators have established prognostic factors for pancreatic cancer, data regarding LAPC are limited. The objective of this study was to investigate the prognostic significance of volumetric parameters measured on pretreatment FDG PET/CT scans for predicting treatment outcomes in patients with LAPC treated with CRT.
MATERIALS AND METHODS
Patients
We retrospectively reviewed the medical records of all pancreatic cancer patients who underwent FDG PET/CT as part of a staging work-up prior to treatment at our institution from January 2007 to December 2010. Patients with a diagnosis of stage III biopsy-confirmed ductal adenocarcinoma, who were initially deemed surgically unresectable upon staging work-up and who received CRT, were included in this study. Sixty patients met the inclusion criteria. Baseline patient and tumor characteristics were reviewed, including age, gender, Eastern Cooperative Oncology Group (ECOG) performance status, history of diabetes mellitus, tumor diameter (mm), tumor location, T stage, nodal status, and non-obstructive pre-CRT and post-CRT CA19-9 levels. The Institutional Review Board of our university approved this retrospective study, and the requirement to obtain informed consent was waived.
Acquisition and analysis of FDG PET/CT scans
All FDG PET/CT scans were performed using a dedicated PET/CT scanner (Discovery STe, GE Healthcare, Milwaukee, WI, USA or Biograph TruePoint 40, Siemens Medical Systems, CTI, Knoxville, TN, USA). All patients fasted for at least 6 h prior to the PET/CT scan. Median blood glucose level was 100 mg/dL with a range of 72-210 mg/dL. A dose of approximately 5.5 MBq/kg of FDG was intravenously injected 60 min before imaging. After the initial low-dose CT (Discovery STe: 30 mA, 130 kVp; Biograph TruePoint: 36 mA, 120 kVp), the PET scan extending from the neck to the proximal thighs with an acquisition time of 3 min per bed position in 3-D mode was performed. The PET scans were reconstructed using ordered subset expectation maximization with attenuation correction.
Volume-based assessment of the primary pancreatic cancer lesion was performed using the volume viewer software on a GE Medical Systems Advantage Workstation 4.5. Each tumor was examined with a spherical-shaped volume of interest (VOI) that included the entire lesion in the axial, sagittal, and coronal planes. The maximum SUV (SUVmax) of the VOI was calculated as (decay-corrected activity/tissue volume)/(injected dose/body weight). Once the threshold for volumetric analysis was assigned, the software automatically calculated MTV and mean SUV of the VOI from PET data by grouping all spatially connected voxels equal to or above the threshold. In this study, MTV was defined as total tumor volume with SUV ≥2.5, and TLG was calculated as (mean SUV)×MTV.
Treatment delivery
All 60 patients who underwent CRT received gemcitabine-based chemotherapy. Only gemcitabine (1000 mg/m2 on days 1, 8, 15, 29, and 36) was administered to most patients. Cisplatin (70 mg/m2 on days 1 and 29) or capecitabine (total daily dose of 2000 mg/m2 for days 1-14 and 21-35) was additionally administered to some patients depending on the preference of the responsible physicians and the general condition of the patient. Chemotherapy was withheld until the resolution of any grade 3 or 4 non-hematologic toxicity.
Patients also received conformal radiotherapy or tomotherapy as a part of CRT. According to the standard CRT protocol, patients received involved-field irradiation consisting of the gross tumor volume (GTV) with a liberal margin (2 cm). If significant lymphadenopathy was noted on the pre-treatment scans, radiotherapy of the specified lymph node areas was also performed. A median total dose of 50.4 Gy with a range of 45.0-58.4 Gy was applied with daily fractions of 1.8 Gy for 5 days per week using a 10 MV linear accelerator. After CRT, patients received maintenance gemcitabine chemotherapy (1000 mg/m2 on days 1, 8, and 15, every 4 weeks) until disease progression or unacceptable toxicities occurred.
Response evaluation
All 60 enrolled patients had clinical follow-ups that included diagnostic imaging studies and blood tests. Tumor response was assessed according to the Response Evaluation Criteria in Solid Tumors on contrast-enhanced CT scans obtained at 4 weeks after completion of CRT. Disease control status, defined as complete response, partial response, or stable disease, was also evaluated at each time point.
Data analysis
All 60 patients were assessed and grouped according to whether they had experienced progression of disease at the 1-year follow up. The SUVmax, MTV, and TLG on FDG PET/CT scans, as well other tumor factors, were compared between the 2 subgroups using Mann-Whitney U tests, chi-squared tests, t-tests, and Fisher's exact tests. Survival curves were estimated using the Kaplan-Meier method to calculate the cumulative locoregional progression-free survival (LRPFS), progression-free survival (PFS), and overall survival (OS). LRPFS was defined as survival without local or regional treatment failure, calculated as the time between the first day of treatment and the date of local or regional failure, death, or last visit. The PFS was calculated as the time between the first day of treatment and any type of disease progression, while the OS was defined as the time between the first day of treatment and the date of death or last visit.
For statistical analyses, all variables for survival were grouped into two categories according to specific cutoff values. The optimal cutoff values were determined using receiver-operating characteristic (ROC) curve analysis. The significance of the predictive value of each variable was evaluated using log-rank tests for univariate analysis and Cox proportional hazards regression tests for multivariate analysis. Multicollinearity between MTV and TLG was evaluated by calculating the Spearman rank correlation coefficient before multivariate analysis. Statistical analyses were performed using SPSS 20.0 for Windows (SPSS Inc., Chicago, IL, USA). Results with p-values <0.05 were considered statistically significant.
RESULTS
Patient characteristics
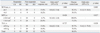
Table 1 summarizes the pretreatment characteristics of all 60 patients enrolled in the study according to disease status at the 1-year follow up. The median PFS was 6.2 months [95% confidence interval (CI): 3.8-8.6 months] and the overall 1-year progression-free survival rate was 68%. Distant relapse (n=34; 82.9%) was the main cause of initial treatment failure, 31 instances of which were isolated (75.6%) and 3 (7.3%) that were concomitant with locoregional progression. Local treatment failure without concomitant distant metastasis was observed in 8 patients (19.5%), 6 (75%) of whom eventually had relapse with distant metastasis. Sites of distant metastasis included the liver (n=17), peritoneum (n=9), multiple organs (n=7), and lungs (n=1). There was no significant relationship between the pattern of initial disease progression (distant versus local) and PET/CT parameters (SUVmax, MTV, and TLG). In comparing patients with and without disease progression, SUVmax, MTV, and TLG were significantly different between these two groups (p<0.05, all) while the other demographic and clinical characteristics did not show statistical significance. From the ROC analyses, the optimal cut-off values for SUVmax, MTV, and TLG were set at 6.5, 10.0 cm3, and 45.0 g, respectively. Cut-off values for the pre-CRT CA19-9 level, post-CRT CA19-9 level, and decline in the CA19-9 levels after CRT were also defined as 646 U/mL, 144 U/mL, and 87.8%, respectively.
Tumor response assessment
Overall treatment response was 16.7% at the 4-week follow up after CRT, and the disease control rate (DCR) was 80%. To assess the predictive value of the PET/CT parameters and CA19-9 levels, we classified patients into 2 groups, higher and lower, based on the cut-off values obtained from the ROC analyses described above. There were no significant statistical differences in the PET/CT and CA19-9 results between the responder and non-responder groups. However, the DCR was significantly higher in patients whose tumors had lower SUVmax, MTV, or TLG values than those in the other group, while none of the CA19-9 parameters showed statistical differences. These results are summarized in Table 2.
Survival analysis and prognostic factors
At a median follow up of 13 months (range, 3-67 months), 58 out of the 60 evaluated patients (96.7%) had died. One patient was alive without disease progression, and the other remaining patient was also alive but had liver metastasis and peritoneal carcinomatosis. Both patients had consistently lower SUVmax, MTV, and TLG and lower pre-CRT and post-CRT CA19-9 levels, which declined significantly after CRT. During follow-up, 41 patients (68.3%) experienced some degree of treatment failure. The median durations of PFS, LRPFS, and OS were 6.2 months (95% CI: 3.8-8.6 months), 10.9 months (95% CI: 8.1-13.7 months), and 13.2 months (95% CI: 11.9-14.5 months), respectively.
Comparison of survival data using the log-rank test showed that MTV and TLG were significant prognostic indicators for PFS, LRPFS, and OS (Figs. 1 and 2), as was SUVmax for PFS and LRPFS. Through univariate analysis, pre-CRT and post-CRT CA19-9 levels were found to have prognostic significance for PFS, LRPFS, and OS. In addition, disease progression at 4 weeks after treatment was an adverse prognostic factor in terms of PFS, LRPFS, and OS. Median survival times and corresponding results of univariate analysis are shown in Table 3.
Among the significant prognostic variables found by univariate analysis, only those variables that could be assessed before treatment were included in the multivariate analysis (i.e., SUVmax, MTV, TLG, and the pre-CRT CA19-9 level). As TLG is calculated by multiplying the mean SUV and the MTV, there was a significant correlation between the MTV and TLG (r=0.946, p<0.0001). Therefore, MTV and TLG were assessed separately. On the multivariate analysis, the pre-CRT CA19-9 level and MTV were identified as independent prognostic factors for PFS, LRPFS, and OS (p<0.05, all) (Table 4), while TLG remained statistically significant for both LRPFS (p=0.008) and OS (p=0.019) (Table 5).
DISCUSSION
To date, few prognostic factors from heterogeneous study populations have been identified for LAPC. Bjerregaard, et al.21 reported that good performance status with small tumors was significantly associated with favorable prognosis. In a multi-center study including patients with LAPC and metastatic pancreatic cancer, the pretreatment CA19-9 level (<1000 U/mL) as well as a CA19-9 decline of >25% after treatment were strongly correlated with longer time-to-progression and OS.22 A decrease in the CA19-9 level (>90%) was also an independent predictor of improved median survival in a study performed by Yang, et al.23 Our analysis indicated that a pre-CRT CA19-9 level of >646 U/mL was an independent prognostic factor for poor survival in patients with LAPC who were treated with CRT, while a decline in the CA19-9 level was not. The post-CRT CA19-9 level did have statistical significance upon univariate analysis; however in the present study, it was excluded from multivariate analysis due to our focus on prognostic factors that can be assessed before treatment. Nevertheless, we believe that our study has reinforced the prognostic value of CA19-9 levels.
Several recent studies have investigated the prognostic value of FDG PET/CT results in patients with pancreatic cancer. Despite an absence of standardized cutoff values, poorer survival has consistently been associated with high SUVmax values measured on pretreatment FDG PET/CT scans of patients with primary pancreatic cancer.13,14,15,16 However, to the best of our knowledge, only one other study has evaluated the use of FDG PET/CT volumetric parameters for predicting clinical outcomes in patients with LAPC. In that study, Parlak, et al.20 used the GTV measured during radiotherapy planning as a metabolic parameter measured on FDG PET/CT scans of 30 patients with LAPC and showed that those with a GTV of <100.0 cm3 had significantly longer OS and PFS than those with a GTV of >100 cm3. GTV is typically used as a parameter for radiotherapy, and MTV and TLG are corresponding FDG PET/CT volumetric parameters used for survival analysis.17,18,19 In this study, we evaluated the prognostic value of MTV and TLG measured on pretreatment FDG PET/CT scans of patients with LAPC who underwent CRT. Although TLG failed to remain statistically significant for predicting PFS by multivariate analysis, the results of our study demonstrated that MTV and TLG were independent prognostic factors and had a stronger association with survival outcomes compared to SUVmax. MTV is defined as the volume of tumor tissue that shows increased FDG uptake over a certain threshold, which in our study was an SUV of 2.5, and TLG is representative of the metabolic activity throughout the entire tumor. Therefore, volumetric parameters such as MTV and TLG can more accurately reflect the metabolic tumor burden and predict survival outcomes when compared to SUVmax, which is a single-voxel value.17,18,19,24
Previous studies on prognostic significance of volumetric parameters of PET/CT used simple fixed SUV threshold, percentage threshold of SUVmax, or SUV of the liver or mediastinal blood pool; however, there is still no consensus or standardization on defining the threshold for metabolic tumor volume delineation.25,26 We used a fixed SUV threshold of 2.5 and demonstrated that MTV and TLG had prognostic significances. The choice of a fixed SUV threshold of 2.5 was largely based on early studies demonstrating that an SUV within this range is optimal for differentiating benign lesions from malignant lesions and minimizes inclusion of unwanted physiological FDG uptake in normal tissues.26,27,28,29 One recent study using a phantom demonstrated that an SUV of 40-50% of the maximum was appropriate for the contouring of actual tumor volume;30 however, we could not clearly delineate the primary tumor from surrounding normal structures when 40-50% of the SUVmax of the tumor was applied to a threshold in several cases. In addition, it is noteworthy that suggested cutoff values to identify a favorable prognostic group vary widely by tumor site and study group. Therefore, further studies should focus on both standardization of threshold SUV and individualization of cutoff values in order to eventually integrate volumetric analysis of FDG PET/CT into clinical practices.
CRT has been regarded as a reasonable treatment option for LAPC, although the role of radiation therapy remains highly controversial. As LAPC is associated with a high rate of distant metastases and subsequent poor OS, it is now considered as part of the spectrum of metastatic diseases. Multiple clinical trials have attempted to identify the best treatment for LAPC, and trials of only chemotherapy versus CRT have reported mixed results regarding the survival benefits of CRT; therefore, the debate continues.7,8,9,31,32 Recently Iacobuzio-Donahue, et al.33 have identified a promising biomarker, the tumor suppressor SMAD4, as a potential predictor of local versus distant disease progression. Interestingly, patients with intact SMAD4 expression had a local-dominant pattern of disease spread, while those with the loss of SMAD4 had a distant-dominant pattern. This correlation between SMAD4 expression and the pattern of disease spread has been validated by a phase II clinical trial.33,34 It has been argued that patients with occult metastatic disease or a high risk of distant metastasis might not be candidates for RT because the benefit from RT would not outweigh its side effects. In the present study, none of the PET/CT parameters that were analyzed succeeded in predicting a pattern of initial disease progression or which group of patients would show response to CRT at the 4-week follow up. However, the DCR was significantly higher in patients with lower SUVmax, MTV, or TLG, and the univariate analysis showed that the DCR was a significant prognostic indicator of survival outcomes (all p<0.001 for PFS, LRPFS, and OS). Therefore, we postulate that the metabolic activity of pancreatic cancer lesions demonstrated on FDG PET/CT scans might be helpful to guide treatment decisions in cases of LAPC. Given the rapid disease progression and shorter survival times of patients with LAPC, RT would not be recommended when high metabolic activity is detected on pretreatment FDG PET/CT scans. As FDG PET/CT is a relatively non-invasive diagnostic tool, these metabolic parameters are more easily assessed compared to SMAD4 expression. However, a large-scale comparative study is mandatory to validate the clinical use of FDG PET/CT for predicting survival outcomes and guiding treatment decisions in patients with LAPC.
There were several limitations to our study. First, as we enrolled only patients who completed full cycles of CRT and as our hospital is a tertiary referral center, those patients with poor performance and tolerability who chose to discontinue treatment or to receive palliative care at hospice centers were excluded, potentially skewing the study population to a group of better prognosis. Second, we used a threshold SUV of 2.5 for measuring the MTV of pancreatic cancer lesions. Some of the enrolled patients showed diffuse FDG uptake by the pancreatic parenchyma distal to the cancer lesion, mainly due to obstructive pancreatitis. In those patients, it was difficult to clearly differentiate tumor uptake from inflammatory uptake due to pancreatitis, which may have affected the measurement of MTV. We theorize that simultaneous anatomic correlation with other imaging modalities, such as PET-contrast-enhanced CT or PET-magnetic resonance imaging (PET/MRI) would be one solution to this problem. Third, use of different PET/CT scanners may have contributed to SUV variability to a certain extent and biased the results of the present study, although the variations of SUV among PET/CT systems in our institute were within the acceptable limit.35
In conclusion, MTV measured on pretreatment FDG PET/CT scans was an independent and significant prognostic factor for predicting the PFS, LRPFS, and OS, as was TLG for predicting the LRPFS and OS, in patients with LAPC treated with gemcitabine-based CRT. FDG PET/CT volumetric parameters might have the potential to identify the subgroup of patients who would benefit from RT as a part of CRT.






 XML Download
XML Download