

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Women's sexual activity changes as age progresses through adolescence to menopause; pregnancy can also affect sexual activity. It can also be affected by marital status, the presence of depression, anxiety, and other health conditions.1,2,3,4
The Female Sexual Function Index (FSFI) is a multidimensional self-reporting tool for the assessment of female sexual function.5 It consists of six domains: desire, arousal, lubrication, orgasm, satisfaction, and pain (with 19 items). The FSFI is used for the diagnosis of female sexual dysfunction (FSD) by assigning points to participant's responses. The cutoff point for the diagnosis for FSD has been suggested as a total of 26.55 points,6 but is different in each country.7,8 For international use, the FSFI has been translated into Malay, Chinese, Japanese, Persian, and Korean.7,8,9,10,11,12
The 6-item Female Sexual Function Index (FSFI-6) is a shorter version of the FSFI that was created by Isidori, et al.9 The FSFI-6 contains one item from each of the six domains of FSFI. It therefore has the merits of being quicker to conduct (within 3 minutes) and simpler to measure than the FSFI. The cutoff point for diagnosis of FSD on this scale is 19 points. Because of the survey's simplicity, it is useful for screening FSD in the field and for analyzing the need for prospective cohort studies. Currently, the Ecuadorian version of the FSFI-6 was translated and validated in 2012.13
The Korean version of the FSFI-6 has not yet been developed or validated. Therefore, the purpose of this study is to develop a Korean version of the FSFI-6 (FSFI-6K) and determine its validity in the Korean population with reference to the FSFI.
MATERIALS AND METHODS
Participants
This study was performed in the outpatient department of the Center for Uterine Cancer (Obstetrics and Gynecology) from February 2013 to July 2013 in National Cancer Center Korea. Participants were included in this study if 1) they were not diagnosed with cancer, 2) were above 18 years old, 3) were able to speak and understand Korean, and 4) had sexual activity within 3 months of the inclusion date. They signed a consent form. Participants were excluded from the study if they were not able to understand the questions or refused to participate.
Korean version of Female Sexual Function Index-6 (FSFI-6K)
The FSFI-6 is a shorter version of the FSFI and was created by Isidori, et al.9 for measuring FSD through a short survey for women with or without FSD. It consists of six domains: desire, arousal, lubrication, orgasm, satisfaction, and pain. The domains of desire and satisfaction are scored from 1 to 5 points, and the other domains (arousal, lubrication, orgasm, and pain) are scored from 0 to 5 points. The FSFI-6 is determined by compiling each domain's score, resulting in a range from 2 to 30.
Korean version of Female Sexual Function Index (FSFI)
The FSFI consists of 6 domains and 19 items and was developed by Rosen, et al.5 in 2000. The Korean version was developed in 2002.10 Since then, the FSFI has been translated into many languages, becoming the gold standard for measuring female sexual function.9,14,15 FSD is diagnosed if the FSFI score is <26.55.6
Procedure
After obtaining Institutional Review Board approval (NCCNCS-12-685), the FSFI-6K was translated. Two researchers translated the FSFI-6 into Korean, and a bilingual (Korean and English) physician without access to the original English version performed back-translation. The back-translated version was reviewed by another 2 researchers who decided to use this version without revision. Thus, a pilot test of the Korean-language survey was conducted with 30 participants from February to March 2013. There were no reports of misunderstanding, so this version was used as the final version.
Data analysis
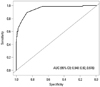
Statistical analysis was performed using the statistical software R version 2.12.1. Number, percentage, and quartile were used to analyze the demographic characteristics of participants. Test-retest reliability was evaluated by using intraclass correlation coefficients (ICC). Internal consistency reliability was estimated using Cronbach's alpha coefficient, and the correlation between each item was calculated using Spearman's correlation coefficient. Discriminant validity was assessed by the receiver operating characteristics (ROC) curve and the area under the ROC curve (AUC).
RESULTS
A total of 267 women were asked whether they had sexual activity within the past 3 months. Among the 267 women, 47 were excluded for the following reasons: 42 responded negatively to having sexual activity within that time frame, 2 had thyroid cancer, 1 had no sexual partner, and 2 did not understand Korean. The primary survey was conducted for the remaining 220 participants, and a follow-up survey was conducted 3 weeks (±1 week) after the primary survey. At follow-up, 199 participants (90.5%) took part in the retest, 18 participants (8.2%) could not be contacted, and 3 participants (1.4%) refused to respond.
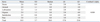
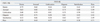
The responses of the 220 women were analyzed statistically. The median age of respondents was 48.1±7.6 years. Among the respondents, 53.2% had a college degree or higher education, 50.0% had an occupation, 47.7% had reached menopause, 52.8% had less than 1 of Charlson comorbidity index, and 40.5% had been diagnosed with FSD (Table 1). The mean total score for the FSFI-6K was 18.9±5.7; the highest score was in the pain domain (3.8±1.5), and the lowest score was in the desire domain (2.8±0.9) (Table 2).
Cronbach's alpha was used to assess the internal consistency and the score was 0.888. Reliability based on the test-retest was calculated of ICC (0.606).
The concurrent validity was measured using the correlation of the ROC curves. The concurrent validity between FSFI-K and FSFI-6K was measured using Spearman's correlation coefficient. All domains ranged from r=0.67 to r=0.81 (p<0.001) (Table 3). The FSD and non-FSD groups were divided using the FSFI-K. The cutoff score for diagnosis of FSD on the FSFI-6K was 21 points, as determined by analyzing the ROC curve (sensitivity, 89.9%; specificity, 86.3%). The AUC of the FSFI-6K total score was 0.948 (95% CI, 0.920-0.976) (Fig. 1).
DISCUSSION
In this study, the original FSFI-6 was translated into Korean, and the translated version was validated through a survey of healthy women. Cronbach's alpha, which measures internal consistency of each domain, was 0.888, a relatively high result. However, the ICC, which is used for assessing the test-retest reliability, was 0.606, a mid-range result. This difference might be explained by differences in sexual activities during the period between assessments. The reason for a low ICC is that the follow-up retesting was conducted between 2 and 4 weeks. As the follow-up retest period was defined as 3 weeks±1 week after the first survey, it is natural that there is a gap in the response to having sexual activity within the past 4 weeks. The relatively low retest reliability implies the possibility of changes in sexual activities during the period of test-retest. The original FSFI-6 contains the phrase "over the past 4 weeks"; this phrase was used unchanged in the Ecuadorian version.13 However, it was changed slightly to "in the recent 3 months" in the Japanese version because the participants were having difficulty in responding.12 The frequency of sexual activity is different in each country in Asia.16 The Korean version uses the phrase "over the past 4 weeks," but it is used for women who have had sexual activity within the past 3 months, reflecting the Japanese version.12 Forty-two women (15.7%) were excluded from this study because they did not meet the requirements of having sexual activity in the past 3 months.
In this study, the cutoff score for diagnosis of FSD was 21 points. In the FSFI-6 validation review table presented in Table 4, the cutoff score is measured at 19 to 20 points.9,13 When no sexual activity is reported in the past 4 weeks, a score of 0 is assigned in the full FSFI and FSFI-6. The response rate was low (5.5%) for those who reported having no sexual activity over the past 4 weeks in the FSFI-6K. The other cutoff scores used in this study were measured differently, and the difference may have been caused by the participants' linguistic, cultural, and health conditions.17,18,19
The advantage of the FSFI-6 is that it is simpler to measure compared to other female sexual function tests and is easily applicable and convenient because it requires less than 3 minutes to complete. The reliability of the FSFI-6 is 0.888, which is higher than that of the FSFI-6K, but the AUC is similar, measuring 0.948 (0.92-0.976) in FSFI-6K and 0.984 (0.951-0.997) in FSFI-6.9
The main limitation of this study is that it was only conducted in the obstetric and gynecologic outpatient population and in those who were mostly disease-free. Obstetric and gynecologic conditions may have affected the responses to the survey. Second, there is a lack of clarity regarding the cutoff score for FSD diagnosis, because it was not determined using Diagnostic and Statistical Manual of Mental Disorders diagnostic criteria.
In conclusion, the FSFI-6K has high internal consistency and acceptable reliability. This validated questionnaire can be used in the Korean population.


 XML Download
XML Download