

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Introduction of a sliding hip screw (SHS) and cephalomedullary nail (CMN) dramatically reduces the incidence of fixation failure in trochanteric fractures.1 Lag screw sliding allows impaction at the fracture site and enhanced stability, enabling early mobilization. Unfortunately, however, excessive sliding of the proximal fragments sometimes occurs in both CMN and SHS systems causing thigh pain and femoral neck shortening (FNS). Excessive sliding has also been thought as one of important causes of fixation failure such as cut out of the femoral head by a lag screw.2,3 Preservation of hip axis length after fracture treatment is an important factor in functional recovery after bone union in patients with hip fractures.4 In femoral neck fractures, neck shortening has been shown to correlate with functional deterioration after bone union.5,6,7
Cephalomedullary nailing became more popular in treating unstable trochanteric fractures in these days.8,9 Presence of a CMN in the medullary canal has been thought as advantageous in the control of lag screw sliding and FNS compared to extramedullary fixation system in trochanteric fracture. However, researches on the factors that influence the degree of FNS after cephalomedullary nailing are lacking. In this study, we analyzed the factors that influence lag screw sliding distance and FNS in patients who underwent cephalomedullary nailing after sustaining trochanteric fractures.
MATERIALS AND METHODS
Patient group
From January 2006 to December 2010, 565 patients sustained trochanteric fractures (AO/OTA classification 31-A1 to A3) and were treated at two institutions with ITST nails (ITST™, Zimmer®, Warsaw, IN, USA). We selected 116 patients between the ages of 70 and 80 years old to minimize the age related factors such as medullary canal diameter and bone mineral density (BMD). Of these patients, 95 were followed for more than 1 year after surgery or revision surgery.
Surgical method and rehabilitation
Surgery was performed with the patient in the supine position on the fracture table under general or spinal anesthesia. When possible, we aligned the medial cortices of fractured fragments in the antero-posterior image and the anterior cortices in the axial radiological image before the incision. When closed reduction failed, a long hemostatic forceps or pointed bone forceps was used to hold the fragments in reduced position after incision. A nail entry site was created on the medial edge of the tip of the greater trochanter. A CMN was inserted into the reamed medullary canal after trochanteric reaming. The diameter of the CMN was determined during preoperative planning according to the diameter of the medullary canal. Specifically, we measured the inner diameter of the proximal femur 2 cm below the distal border of the lesser trochanter in the Picture Archiving and Communication System (PACS) using a magnification bar. We used a nail 1 mm smaller than the measured value. In patients whose medullary canal diameter was over 13 mm, we used a 12-mm diameter CMN, the largest available nail in hospitals. If the medullary canal was too narrow to accept a 10-mm nail (the smallest available nail in the hospitals), we reamed the proximal femur with the medullary reamer, up to 11 mm. Reaming of the proximal femur was performed only if it was necessary to accept the nail. The end of the lag screw was positioned at the center of the femoral head in the antero-posterior and axial images. Distal locking was performed with one or two screws. Rehabilitation started at the first postoperative day. Sitting and continuous passive motion of the knee and hip joints were allowed. The majority of patients were encouraged to partially bear their weight within 1 week after surgery with walking aids depending on the patient's condition.
Evaluation
Fracture subgrouping was performed using AO/OTA classification. BMD was measured on the normal side of the hip joint using dual-energy X-ray absorptiometry (DXA; Discovery™, Hologic®, MA, USA) in 79 patients (83.2%) after surgery. Femoral neck T-scores were selected to represent patient BMD. The clinical absence of pain, presence of a callus shadow that passed through the fracture line in three cortices, and closure of the fracture line were used to determine bone union. Radiological measurements were analyzed using the PACS.
Radiological measurement
Standard anteroposterior (AP) radiographs of the hip were obtained with both legs positioned to an internal rotation of 15°. Lateral radiographs were taken with the opposite hip flexed and abducted. The canal occupancy ratio (COR) was calculated by dividing the CMN size by the femoral canal diameter. FNS after union was measured using the method described by Weil, et al.,7 at the time of the final follow-up exam. Briefly, the contralateral femur was overlaid on the shortened femur in the final AP radiogram. FNS was calculated using vectorial addition of changes in the x-axis (shortening in the abductor arm) and in the y-axis (shortening in the vertical plane). The sliding distance of the lag screw was measured from the antero-posterior radiological images taken immediately after surgery and at the time of the final follow-up examination, using the method of Watanabe, et al. 10 The tip-apex distance (TAD) was measured from the postoperative radiographs. The reduction was categorized as good, acceptable, or poor using the method of Baumgaertner, et al.11
Data analysis
We used SAS version 9.1 (SAS Institute Inc., Cary, NC, USA) for statistical analyses. Univariate and multiple regression analyses were performed to assess the individual patient effects on FNS. A stepwise multiple linear regression analysis was performed with backward elimination to select an appropriate model. A p-value greater than 0.10 was used for removal. A p-value by two tailed test less than 0.05 was considered significant for all analyses.
RESULTS
The average period of follow-up was 15 months (range, 12 to 44 months). Among the 95 patients, 11 were male and 84 were female. The average age was 75.1 years old (range, 70 to 80 years of age). Regarding the reduction,11 49 fractures (51.6%) were judged to be good, 43 fractures (45.3%) acceptable, and 3 fractures (3.2%) were poor. Bone union was observed within 14.5 weeks on average (range, 12 to 19 weeks). Fixation failure occurred in 3 patients. These included a femoral head fracture caused by a lag screw after a second fall (31-A2.1; lag screw sliding, 15.6 mm), cut-out of a lag screw after varus collapse (31-A1.2; lag screw sliding, 3.3 mm), and a superior migration of a lag screw (31-A2.2; lag screw sliding, 4.8 mm).
The diameter of the femoral medullary canal measured 2 cm distal to the lesser trochanter was 13.4 mm on average (range, 10.2 to 21.6 mm). The average hip T-score of the intact femur was -2.7 (range: -0.8 to -4.9). The average TAD was 16.9 mm (range, 9.6 to 20.2 mm). The average COR was 0.87 (range, 0.56 to 0.99). According to the AO/OTA fracture classification, there were 37 cases of A1, 55 cases of A2, and 3 cases of A3.
Sliding distance of a lag screw
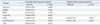
The mean sliding distance was 3.11 mm (range, 0.50 to 16.80 mm); 2.55 mm (range, 0.5 to 8.1 mm) in A1, 3.02 (range, 0.7 to 12.1 mm) in A2, and 11.67 mm (range 8.4 to 16.8 mm) in A3. A3 type fractures demonstrated more screw sliding than A1 or A2 type fractures (p=0.004, p=0.006). Univariate regression analysis was performed to test the association of sliding distance to gender, age at the time of surgery, BMD, medullary canal diameter, COR, TAD, and AO/OTA classification. AO/OTA type (A1 versus A3; R2=0.6241, β=9.121, p<0.001), medullary canal diameter (R2=0.174, β=0.412, p<0.001), and COR (R2= 0.104, β=2.046, p=0.004) were significantly correlated with lag screw sliding distance. Multiple regression analyses (R2= 0.522) illustrated that COR (β=-9.410, p<0.001) and AO/OTA type (A1 versus A3; β=7.803, p<0.001) were more strongly correlated (Table 1).
Femoral neck shortening
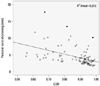
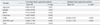
The mean FNS was 4.49 mm (range, 1.7 to 17.8 mm); 3.90 (range, 1.90 to 9.50 mm) in A1, 4.41 mm (range, 1.70 to 13.50 mm) in A2, and 13.27 mm (range, 10.20 to 17.80 mm) in A3. Univariate regression analysis was performed to test the association of FNS to gender, age at the time of surgery, BMD, medullary canal diameter, COR, TAD, and AO/OTA classification. AO/OTA type (A1 versus A3; R2=0.340, β=9.064, p<0.001), medullary canal diameter (R2=0.207, β=0.447, p<0.001), and COR (R2= 0.212, β= -11.052, p<0.001) (Fig. 1) were significantly correlated with FNS. Multiple regression analyses (R2= 0.523) illustrated that COR (β=-8.918, p<0.001) and AO/OTA type (A1 versus A3; β=8.113, p<0.001) were more strongly correlated (Table 2).
DISCUSSION
Controlled lag screw sliding and fracture site impaction are fundamental concepts in treating intertrochanteric fractures as well as femoral neck fracture. However, excessive sliding of lag screw and resultant short femoral neck sometimes ends up with unfavorable functional recovery. In this study, we identified that lag screw sliding distance and FNS were determined by many uncontrollable factors by the surgeons and the presence of CMN alone couldn't effectively control them, especially in low COR and 31-A3 type fractures. The sliding distance in the SHS system depends on many factors including inclination angle of the lag screw,12 fracture type,13 reduction status,11 and bone quality.14 The CMN system theoretically has been regarded as having several advantages over SHS system such as a shorter lever arm, the ability to more efficiently deliver weight through the calcar femorale, and nail placement inside the medullary canal that abuts the neck fragment.15 However, studies assessing the sliding distance and final FNS after CMN are limited. We reviewed 11 randomized clinical trials comparing SHSs and CMNs in trochanteric fractures.16,17,18,19,20,21,22,23,24,25,26,27 There were little mention regarding the differences in lag screw sliding between two systems and only one study by Hardy, et al.,21 showed a statistically significant decrease in sliding of the lag screw with CMN compared to SHS.
Excessive sliding, FNS and thigh pain due to protrusion of the lag screw also occurs in the CMN system and are an unsolved problem. We showed herein, with univariate linear regression, that the diameter of the medullary canals, COR, and AO/OTA type were significantly correlated with FNS. The sliding distance of the lag screw revealed similar results as FNS. The increase in medullary canal diameter is closely related to aging. In a preliminary study (unpublished data), we analyzed lag screw sliding distance in 119 patients who were implanted and fixed with a 12 mm CMN which was the largest nail available in the hospital. We recognized that aging was well correlated with canal diameter and COR were prominent factors in lag screw sliding. For this reason, we selected patients aged 70- to 80-years-old to minimize the effects of aging. It is very importance due to following reasons. First, if the canal diameter is large, a relatively smaller nail may not be able to effectively support the proximal fragment because of toggling motion at the fracture site during gait cycle. Second, ageing causes an increase in canal diameter and a decrease in cortical thickness of the proximal femur.28 Third, it is unrealistic to manufacture and supply a full-set of nails (length and size) due to cost effectiveness.
A limitation to the study is the retrospective design. Three of the most difficult factors to control are aging, surgical skill of the surgeons and correct measurement of FNS and sliding distance of the lag screw due to rotation. To minimize the effect of aging, we limited the patient age to 70-80 years old in this study. The two institutes which collected the patient data in this study were referral hospitals. Only a single orthopedic surgeon who experienced CM nailing for more than 200 cases in each hospital was designated and performed the operations to minimize the technical errors. As a result, reduction status was acceptable at 96.9% or higher and TAD was well controlled under 20 mm in most of the case. The rate of fixation failure was low as 3.2% and decreased to 2.1% when we discarded the case of cut-out caused by a second fall during rehabilitation. Effect of limb rotation in calculating FNS was minimized by using the method described in the literatures.6,7
In conclusion, we analyzed 95 cases of CM nailing and confirmed that the presence of a CMN in the medullary canal alone could not effectively prevent FNS in patients with low COR and A3 type fracture. This study added important information in treating trochanteric fracture with a CMN. However, low fixation failure rate and insertion of 10 mm CM nail after reaming in patients with extremely narrow canal might have influenced our results. Therefore, further studies with prospective, large number of patients are needed to assess the factors affecting femoral neck shortening and lag screw sliding.
 XML Download
XML Download