

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Postoperative ileus (POI) is a transient impairment of bowel motility related to surgical trauma and associated physiological responses.1 The urologic procedure with which POI is most commonly associated is radical cystectomy (RC) wherein a portion of the small bowel, usually the ileum, is resected and utilized as a urinary conduit. Prolonged POI is associated with nausea, vomiting, delayed oral intake, increased postoperative morbidity, and length of hospital stay (LOS) and, thus, increased medical expenditure.2 Therefore, minimizing the duration of POI is a desirable aim for all healthcare services.
The mechanisms underlying POI are known to be complex. Increasing age, body mass index (BMI), operative time, blood loss, activation of inhibitory reflexes, inflammatory mediators, and both endogenous and exogenous opioids are thought to be contributing factors to prolonged POI.3 Although it is not possible to completely eradicate POI, strategies have been explored to shorten its duration. These include minimally invasive surgery, reduction of opioids, prokinetic agents, early mobilization, enteric feeding, and epidural anaesthesia, all of which require cooperation of the entire surgical and anaesthesiology team.4 Considerable advancements in this field of research have led to substantial reductions in POI; however, considering that POI is the most serious burden for patients following radical cystectomy with ileal conduit (RCIC), additional investigations are needed to understand the underlying multifactorial mechanisms and to further improve rehabilitation of bowel function.
The purpose of the current study was to examine whether factors could be identified that predict the prolongation of POI following RCIC with a specific focus on pharmacological analgesic regimens and perioperative determinants during routine RCIC care regimens. Our results suggest that duration of POI following RCIC depends on multiple causative factors; some factors are modifiable during the rehabilitation program to promote early restoration of bowel function.
MATERIALS AND METHODS
Patients
From our prospective bladder cancer database, 196 patients who underwent RCIC between March 2007 and January 2013 were identified. Among them, 78 (75%) open RCICs and 26 (25%) robot-assisted RCICs were identified with adjustment for age, gender, American Society of Anesthesiologists (ASA) grade, and BMI. Patient demographics and perioperative records including operative time, intraoperative positive intravenous (IV) fluid balance, estimated blood loss (EBL), lymph node (LN) yield, and opioid analgesic dose were retrospectively obtained to assess their associations with time to first passage of flatus, tolerable oral diet, and LOS. Patients who had previous histories of abdominal surgery, neoadjuvant or adjuvant chemotherapy, or exposure to pelvic radiotherapy were excluded from the study.
Operative technique and postoperative care
For all patients, our institution used a collaborative clinical care pathway following RCIC. Prior to general anaesthesia, epidural patient-controlled analgesia (PCA) was applied which was consisted of fentanyl, a lipophilic opioid. The total dose of fentanyl was adjusted according to BMI, with epidural infusion rates set at 10-12 µg/h to provide continuous delivery for a period of 72 hrs. RCICs were performed in a standardized manner for pelvic lymph node dissection. Robotic RCICs were performed with a single 12 mm camera trocar; three 8 mm robotic trocars and a 12 mm and a 5 mm assistant trocar with urinary diversions operated extracorporeally. Open RCIC was performed through an infraumbilical incision. Following surgery, all patients were placed on a standard post-cystectomy care plan including early ambulation, placement of nasogastric decompression tubes until the first passage of flatus, and single intravenous injection of 50 mg of tramadol applied according to patient desires. Initiation of diet began after the first passage of flatus and after confirming tolerance to sips of water. The time to diet toleration was defined as the first day of consecutive oral consumption until discharge without signs of abdominal distension, nausea, or emesis.
Outcome measures
The primary outcome was to investigate perioperative factors associated with prolonged duration of POI in terms of time to first flatus, tolerable oral diet, and LOS. For multivariate logistic regression analyses, POI was defined as an absence of passage of flatus by 5 postoperative days.5 Intraoperative factors measured included operative time (incision to closure), EBL, excessive intraoperative fluid overload, LN yield, and surgical modality (i.e., open versus robot-assisted technique). Postoperative factors examined included the total dosage of PCA fentanyl and cumulative dosages of tramadol within the first five days after surgery. All outcome measures were obtained retrospectively.
Statistical analyses
Demographic and baseline data were summarized using proportions and medians where appropriate. The χ2-test was used to evaluate associations between categorical variables, and the Mann-Whitney U test was used for continuous variables. Liner regression analyses were performed to identify factors associated with the duration of bowel recovery indices. Univariate and multivariate analyses were performed according to logistic regression models. Variables considered as potential predictors for multivariate modeling were selected by univariate analyses and subsequently tested in a stepwise forward conditional manner with entry and retention in the model set at a significance level of 0.05. All reported p-values were two-sided with statistical significance set at p<0.05. All analyses were performed using SPSS version 18 (SPSS Inc., Chicago, IL, USA).
RESULTS
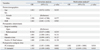
Patient demographics and perioperative data according to surgical modality are shown in Table 1. Comparisons of gender, age, ASA grade, and BMI confirmed appropriate cohort matching. Compared to the open RCIC group, the robot-assisted RCIC group experienced less EBL and shorter times to tolerable oral diet and LOS, even though extents of surgery were wider, as shown by higher LN yields. Total infused doses of fentanyl and tramadol were comparable between the two surgical groups. Mean operative time and time to first passage of flatus were not significantly different between the groups. However, utilization of the robotic-system resulted in significantly shorter time to diet and shorter LOS.
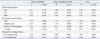
Multivariate logistic regression analysis incorporating patient age, gender, ASA grade, BMI, EBL, intraoperative positive IV fluid balance, operative time, and cumulative dosages of fentanyl and tramadol, demonstrated that both fentanyl and tramadol dosages were associated with an increased risk of POI (Table 2). Multiple linear regression analysis was performed to investigate the dose-response relationship between studied determinants and bowel recovery indices (Table 3). For the overall cohort, age, gender, ASA grade, BMI, EBL, intraoperative positive IV fluid balance, LN yield, and operative time had no associations with the duration of POI. However, the total dosages of fentanyl and tramadol revealed significant positive associations with time to flatus, tolerance to diet, and LOS.
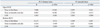
Effects of fentanyl and tramadol dosages were investigated according to each surgical modality and are presented in Table 4. In the open RCIC group, both fentanyl and tramadol doses were significantly positively associated with all bowel recovery indices. In the robotic RCIC group, only tramadol dosage had a significant positive association with time to first flatus and oral diet. Perioperative factors including EBL, positive IV fluid balance, LN yield, and operative time did not show any associations with bowel recovery indices for either surgical modality (data not shown; p>0.05).
DISCUSSION
RC with pelvic lymph node dissection is the standard treatment for muscle-invasive bladder cancer and yields a 10-year recurrence-free survival rate of 50-59%; overall survival rates are approximately 45%.6 RCIC is a technically challenging procedure, after which patients often face uncertain postoperative courses. Among various postoperative complications-including surgical site infection, pelvic lymphocele formation, and anastomosis leakage-POI is the most common, occurring at a rate anywhere from 1.58% to 25.5%.6 The etiology of POI is complex. It is primarily associated with surgical stress, as it is an acute inflammatory response to manipulation of the bowel during surgery wherein endogenous opioids are secreted through the gastrointestinal (GI) tract in response to surgical trauma.7 Recent advancements in anaesthetic and surgical techniques have led to substantial reductions in convalescence and LOS after major GI surgeries. To gain further insight into how treatment regimens affect bowel recovery following RCIC, components of our institutional rehabilitation program including pharmacologic, anaesthetic, and surgical modality regimens were collected and investigated. Observations of our study assumed a dose-response relationship between postoperative opioid-based analgesics and bowel recovery time. The result that robotic RCIC quickened bowel recovery lends further support to the notion that decreased handling and exposure of the intestines and less manipulation of the abdominal wall are strong factors in reducing the duration of POI.2
Opioid effects in the prolongation of POI
Our results revealed that the total doses of fentanyl and tramadol each converted into morphine equivalents were not only independent predictors of POI, but also had a dose-response relationship with the duration of POI. Opioids directly act on cerebral and spinal µ-opioid receptors at the level of the myenteric plexus to suppress pain transmission.8 Opioid-based analgesia is currently the standard of care for the management of perioperative pain after major bowel surgeries due to their strong analgesic effect. At the same time, however, opioids act on peripheral µ-opioid receptors in the GI tract, resulting in disruptions of the migrating motor complex and propulsive motor activity associated with GI motility, thereby exacerbating POI.2,7 The exacerbation of bowel dysfunction is one of the most distressing side effects of opioids, which restricts their use.
Our study revealed a dose-dependent association between opioid dose and duration of POI following RCIC. This association could be explained by the assumption that the effect of epidural administration of opioids is mediated not only by a local effect on spinal µ-opioid receptors, but also by therapeutic serum levels achieved after systemic absorption and distribution of opioid.9 An indirect effect of opioids on bowel dysfunction has been experimentally studied by Topcu, et al.,10 who showed that inflammation sensitizes opioid receptors in the myenteric and submucosal plexus as well as in the peripheral and central terminals to increase effects of exogenously administered opioids. Whereas intestinal inflammation is known to increase pharmacologic effects of opioids by 1.9-fold, bowel resection and re-anastomosis as in RCIC may lend further weight to the evidence of this adverse effect.11
Tramadol, a synthetic analogue of codeine, is a centrally acting analgesic with a low affinity for µ-opioid receptors.10 Nevertheless, studies found that tramadol also has a dose-dependent prolonging effect on colonic transit time, although the effect is relatively small compared to other opioids.12 Our study confirmed that cumulative dose of tramadol is a contributing factor to POI, and that minimizing its dosage, in consideration of pain degree, could be a promising strategy for patients with prolonged bowel recovery.
Utilization of minimally-invasive surgical techniques to reduce the duration of POI
Utilization of the robotic system provided significant reductions of duration to tolerable oral diet and LOS compared to the open technique. Our results in Asian men are in part consistent with previous studies with Western men in which the duration of POI was significantly reduced by robotic surgery compared to the open technique (Table 5).13,14,15,16 Several mechanisms are suggested. First, the duration of POI has been shown to correlate with the degree of surgical trauma.3 Activation of inhibitory reflexes in the afferent limbs originating from the incision (somatic fibers) as well as from intestines (visceral fibers) have been proposed to be one of the underlying mechanisms in the development of POI.17 This stress response, which inhibits GI motility, is attributed to increases in the release of cytokines and catecholamines, e.g., norepinephrine.18 Second, excessive manipulation of the intestines has been reported as a pathogenic factor in the development of POI.17 This is thought to be the result of activation of resident immune cells, particularly macrophages, and the recruitment of circulating leukocytes to the bowel wall.17 Excessive manipulation of the bowel during surgery has been shown to increase mucosal permeability, resulting in endogenous bacterial products which act synergistically with this inflammatory process.19 In conjunction with these mechanisms, secretion of prostaglandins and cytokine cascades, including a pivotal role for tumour necrosis factor-α and interleukin-1β, are also known to contribute to inflammatory responses, which cause intestinal smooth muscle dysfunction.20
Significance of alternative strategies in reducing the duration of POI
A series of strategies to reduce the duration of POI that had been proposed in previous studies did not show significant correlations in our study. First, there was no significant effect of minimizing perioperative fluid excess to prevent intestinal edema, even though restricting intraoperative fluid was shown to significantly reduce POI in patients undergoing colonic surgery.21 Accordingly, patients who received liberal amounts of fluids had a significantly longer time to first passage of flatus.22 In our study, intraoperative positive fluid balance was correlated with time to tolerable diet (r=0.278, p=0.032) and LOS (r=0.352, p=0.002); however, the correlation coefficients were too low to be considered significant. Second, high EBL has been shown to be a predictor for paralytic ileus.6 In our study, however, EBL showed no significant associations. Third, preoperatively higher ASA score, older age, and female gender are widely accepted determinants that affect prolongation of POI.3,6 Therefore, we considered these factors as confounders and adjusted for them when selecting our cases, supporting the idea that other determinant factors should be weighed based on relative importance rather than being assigned equal weights. Lastly, performing intracorporeal rather than extracorporeal urinary diversions has been suggested to quicken bowel recovery by reducing unnecessary fluid loss from the bowels, thus preventing electrolyte imbalance.23 However, comparison studies between both procedures have so far failed to show a benefit of intracorporeal urinary diversions in terms of bowel recovery.24
The retrospective nature and the selective bias inherent in surgical studies are limitations of this study. Although patients of the open RCIC group were selected upon adjustment of confounding factors, there were patients who were not considered as candidates for cystectomy due to comorbidities. Urologists should set an evidence-based consensus upon the management of this complex issue, considering that POI is an entity which depends not only on the hands of the surgeon, but also on multiple other factors.
POI has long been thought to be an obligatory response following bowel surgery; however, evidence indicates that multimodal rehabilitation strategies may reduce the duration of POI. In our study, utilization of the robotic system was found to be a feasible option for shortening the time to POI recovery. Moreover, minimizing the dosage of opioid-based analgesics was observed to confer additional benefit in further shortening the duration of POI following both open and robot-assisted RCICs.


 XML Download
XML Download