

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Colorectal cancer is the third most common cancer worldwide and the second leading cause of cancer-related deaths.1,2 The role of colonoscopy has been emphasized as an effective tool for screening colorectal neoplasm.3,4,5 Particularly, colonoscopic polypectomy can reduce the incidence and mortality of colorectal cancer by 76-90%6,7 and 53%,8 respectively. Most colorectal polyps can be removed safely by various polypectomy techniques. However, serious complications, such as bleeding, perforation, and death can occur during the procedures. Among them, post-polypectomy bleeding (PPB) is one of the most common complications.9
PPB can occur immediately following polypectomy or can be delayed up to 30 days. The rate of immediate PPB (IPPB) is reported to range from 2.1 to 9% depending on the study population and center type, and the delayed PPB (DPPB) incidence is 0.7-2.5%.10,11,12 An age ≥65 years, cardiovascular or chronic renal disease, the use of anticoagulants, a polyp size greater than 10 mm, polyp morphology, poor bowel preparation, the cutting mode of electrosurgical current, and inadvertent cutting of a polyp before current application are noted as independent risk factors for IPPB.12 Advanced age, hypertension, large sessile polyps, polyps at the proximal colon and polypectomy with pure coagulation are known to be risk factors for DPPB.10,11,13
Patients with liver cirrhosis have demonstrated greater risks for surgical- and anesthesia-related complications than those with a healthy liver.14,15,16 Thrombocytopenia occurs in 76% of cirrhotic patients and it may increase the risk of bleeding during invasive procedures.17,18 Particularly, procedure-related complications are associated with the severity of liver function. A previous study has reported mortality rates of 10, 17, and 63 percent in cirrhotic patients with Child-Pugh class A, B, and C undergoing abdominal surgery, respectively.19 However, the risk of PPB after colonoscopic polypectomy has not been well known in patients with liver cirrhosis. The aim of the present study was to evaluate the risk of PPB after colonoscopic polypectomy in patients with liver cirrhosis and compare it with those with a healthy liver.
MATERIALS AND METHODS
Patients and methods
From June 2006 to October 2012, 497 patients with liver cirrhosis underwent colonoscopy at Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. Among them, 106 cirrhotic patients (21.3%) received colonoscopic polypectomy and were reviewed retrospectively in the present study. The cirrhosis was diagnosed using clinical tools such as ultrasonography, computed tomography, magnetic resonance imaging, transient elastography, liver biopsy, and serum variables. The liver cirrhosis was stratified by Child-Pugh class to show the disease severity.20 The exclusion criteria of the study were as follows: a final pathology diagnosis of a submucosal tumor including lipoma, carcinoid, and leiomyoma; removal of polyps by biopsy; a history of polypectomy (to avoid overlapping data); and a history of anticoagulant therapy. Finally, 89 patients with liver cirrhosis were included in the present study. The 348 healthy subjects were selected as control group from the Severance Hospital colonoscopy cohort by using the propensity score for matching age, gender, and underlying disease during the same period (Fig. 1). All subjects of control group didn't have abnormal finding in abdominal imaging evaluations and abnormal laboratory finding including viral markers.
We reviewed all of data including age, gender, body mass index (BMI), the use of antiplatelet therapy (aspirin and clopidogrel), underlying disease, bowel preparation, polyp morphology, polyp size, polyp location, polyp histology, and the number of polypectomies. The bowel preparation was classified as inadequate or adequate.21 The polyp location was classified as the distal or proximal colon.11 The proximal colon included the cecum, ascending colon, hepatic flexure, transverse colon and splenic flexure. The distal colon included the descending colon, sigmoid colon and rectum. The polyp histology was classified as neoplastic polyp or non-neoplastic polyp. A neoplastic polyp indicated tubular, villous, tubulovillous and serrated adenomas. A non-neoplastic polyp indicated an inflammatory or a hyperplastic polyp.
Colonoscopic polypectomy was performed by experienced endoscopists. In most of cases with Child-Pugh class B or C cirrhosis, colonoscopy was performed due to abdominal pain, diarrhea, constipation, hematochezia or meleana. The procedure type, such as snare polypectomy or endoscopic mucosal resection (EMR), was chosen according to the patient's condition and polyp characteristics. High-frequency electrocautery with blended current was used. No case in the present study was treated by cold polypectomy. Antiplatelet therapy, such as aspirin or clopidogrel, was discontinued at least 3-7 days before the procedures. Immediate and delayed bleedings were controlled with hemo-clipping or electrocoagulation.
This study was performed in accordance with the ethical guidelines of the 1975 Declaration of Helsinki. Written informed consent was obtained from each participant or responsible family member after possible complications of colonic polypectomy had been fully explained. This study was approved by the independent Institutional Review Board of Severance Hospital.
Definition of IPPB and DPPB
PPB was divided into IPPB and DPPB. IPPB was defined as bleeding observed immediately after polypectomy and required hemostatic procedures because the bleeding continued for over 60 s. DPPB was defined as bleeding that occurred at the polypectomy site within 30 days of the procedure and requiring hospitalization or treatment.
Statistics
The primary outcome was to compare the risk of PPB in cirrhotic patients with that in control patients. The secondary outcome was to evaluate risk factors for PPB in patients with liver cirrhosis. The risk factors for PPB were analyzed according to patient factors and polyp factors. The patient's factors included age, gender, body mass index, underlying disease, number of polypectomies, and bowel preparation. The polyp factors were size, location, morphology, and histology. In sub-analysis, risk factors of PPB were evaluated in patients with liver cirrhosis according to Child-Pugh class. Statistical analysis was performed using χ2-test, Fisher's exact test, Student's t-test, and logistic regression analysis. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated to estimate the effect of variables. All tests of significance were two-tailed, and p values less than 0.05 were deemed statistically significant. All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS), version 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Demographics
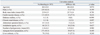
Baseline characteristics of the patients are summarized in Table 1. The mean number of polypectomies was 2.4 in the liver cirrhosis group and 2.2 in the control group. The insertion time tended to increase in the liver cirrhosis group compared with the control group (9.7 min vs. 7.7 min, respectively; p=0.063). The withdrawal time was not different between the two groups. Other clinical characteristics including age, gender, BMI, underlying disease (such as cardiovascular disease, diabetes, and chronic renal disease), history of abdominal operation, and antiplatelet use were not statistically different between the two groups. Among 89 patients with liver cirrhosis, 75 (84.3%) were Child-Pugh class A, 10 (11.2%) were Child-Pugh class B and 4 (4.5%) were Child-Pugh class C. The cause of liver cirrhosis included 69 patients with hepatitis B virus infection, 6 with hepatitis C virus infection, 7 with alcohol abuse and 7 with miscellaneous reasons.
In the liver cirrhosis group, 11 (12.4%) and 2 patients (2.2%) developed IPPB and DPPB, respectively. In the control group, 29 patients (8.3%) and 1 patient (0.3%) developed IPPB and DPPB, respectively. The incidences of IPPB and DPPB were not statistically different between the two groups.
Risk factors for IPPB
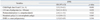
The risk factors for IPPB were analyzed according to the patients' factors (Table 2). Univariate analysis showed that underlying disease (such as cardiovascular disease, diabetes mellitus and chronic renal disease), antiplatelet use, bowel preparation, and the number of polypectomies were not significant risk factors for IPPB. Liver cirrhosis itself was not a risk factor for IPPB (p=0.240).
Subgroup analysis of risk factors for IPPB was performed in patients with liver cirrhosis (Table 3). Univariate analysis showed that Child-Pugh class B and C were significant risk factors for IPPB compared with Child-Pugh class A (p=0.013). Other factors, including the hemoglobin level, total bilirubin level, albumin level, alanine aminotransferase level, platelet count and prothrombin time, were not significantly associated with IPPB. The etiology of liver cirrhosis and the presence of varices were not significant risk factors for IPPB.
Risk factors for IPPB were analyzed according to polyp-related factors (Table 4). IPPB occurred in 50 (4.8%) of 1045 polyps. Polyps with IPPB were larger than polyps without IPPB (11.9±9.4 mm vs. 6.7±3.7 mm, respectively; p<0.001). Polyps larger than 10 mm were significantly associated with IPPB compared with those less than 10 mm (p<0.001). Pedunculated polyps were significantly associated with IPPB compared with nonpedunculated polyps (p=0.002). Neoplastic polyp was a significant risk factor for IPPB compared with non-neoplastic polyp (p=0.016). Regarding IPPB of neoplastic colon polyps, 38 polyps were low-grade tubular adenomas, 3 were high-grade tubular adenomas, 1 was a low-grade tubulovillous adenoma and 3 were high-grade tubulovillous adenomas. The polyp location was not associated with IPPB (p=0.09). In patients with liver cirrhosis, univariate analysis showed that polyps greater than or equal to 10 mm, proximal colon location, and EMR were significant risk factors for IPPB (Table 5).
Multivariate analysis for IPPB including patient factors and polyp factors are shown in Table 6. The multivariate analysis revealed that liver cirrhosis with Child-Pugh class B or C (HR, 3.5; 95% CI: 1.9-6.3; p<0.001), polyp size ≥10 mm (HR, 3.6; 95% CI: 1.1-12.1; p<0.032) and pedunculated polyp (HR, 2.4; 95% CI: 1.1-5.4; p=0.022) were significant risk factors for IPPB (Table 6).
DISCUSSION
The current study revealed that liver cirrhosis itself is not a risk factor for IPPB. However, patients with decompensated liver cirrhosis had a high risk for IPPB after colonoscopic polypectomy compared to those with normal liver function. Thus, endoscopists should be cautious to perform colonoscopic polypectomy in patients with liver cirrhosis of Child-Pugh class B or C.
A previous study has reported that 31% of patients with less than 75000 platelets per mm3 displayed bleeding in invasive procedures.22 Because splenomegaly is related with thrombocytopenia,23 invasive procedure can lead to the complications in liver cirrhosis. Additionally, patients with liver cirrhosis have coagulopathy originating from the disease itself. The disruption of these opposing coagulation pathways can change hemostatic activity for individual patients with cirrhosis.24 Thus, colonoscopists have been reluctant to perform these invasive procedures that can cause bleeding.
However, a previous prospective multicenter study showed that chronic liver disease was not a significant risk factor for IPPB.12 In this study, chronic liver disease included simple elevation of liver enzymes as well as liver cirrhosis. Furthermore, a recent single center study with a small sample size reported IPPB in 3.03% of patients with early liver cirrhosis, and the authors concluded that early liver cirrhosis was not a significant risk factor for immediate bleeding after colonoscopic polypectomy.25 However, the study failed to show the risk of IPPB in patients with decompensated liver cirrhosis because only one patient with Child-Pugh class C liver cirrhosis was included. In our present study, we found that the compensated liver cirrhosis is not a risk factor for IPPB, however, the decompensated liver cirrhosis is a significant risk factor for IPPB.
The present study revealed that each laboratory result, such as the platelet count or prothrombin time, could not predict the risk for IPPB in patients with liver cirrhosis. Additionally, the severity of portal hypertension was not associated with the risk of IPPB. Because liver cirrhosis itself has bleeding tendency, it would be interesting to know whether antiplatelet would increase the risk of bleeding after colonoscopic polypectomy in liver cirrhosis. Sub-analysis in patients with liver cirrhosis showed the use of antiplatelet such as aspirin or clopidogrel was not a risk factor for IPPB in patients with liver cirrhosis. However, all the patients in the study discontinued antiplatelet therapy 3 to 7 days before colonoscopic polypectomy. Thus, further study is mandatory to clearly elucidate association of antiplatelet use with liver cirrhosis for the risk of bleeding after colonoscopic polypectomy.
In patients with liver cirrhosis, the frequency of colon polyps has been reported to range from 8.4 to 21%.26,27,28 Due to slow progression from adenoma to cancer, some clinicians encounter the question of whether invasive polypectomy should be performed for liver cirrhosis with Child-Pugh class C. It might be possible to observe colon polyps in patients with decompensated liver cirrhosis because the life expectancy is short.29,30,31 However, with the advent of liver transplantation, patients with Child-Pugh class C can expect a dramatic change from their irreversible disease. Thus, clinicians should know which are risk factors associated with colonoscopic polypectomy in liver cirrhosis, and the decision to remove colon polyps should be made after careful consideration of patient's status.
In our study, DPPB incidence was similar with that in a previous report,10,11,12 and DPPB was not associated with the severity of liver function. With proper hemostatic control of immediate bleeding after polypectomy, DPPB can effectively be prevented even in liver cirrhosis with decompensation. However, all DPPB occurred in the proximal colon, particularly in the ascending colon, even though only five polyps of 3 patients were treated because of DPPB. Thus, endoscopists should be cautious to perform colonoscopic polypectomy in the proximal colon.
The present study has several limitations. First, it was performed retrospectively at a single center. Second, although our study included a larger population than previous studies, the sample size was still insufficient to analyze the tendency of DPPB in liver cirrhosis patients. The number of Child-Pugh class B or C patients also was small. However, the current study is the first study of post polypectomy bleeding to investigate Child-Pugh class B or C. It is difficult to recruit the Child-Pugh class B or C subjects who underwent polypectomy in retrospective study because most of endoscopists have a tendency to avoid the invasive procedure for decompensated liver cirrhosis patients. We believe that a randomized controlled study is required to validate our result and overcome these limitations.
In conclusion, liver cirrhosis itself is not an adverse factor for colonoscopic polypectomy. However, cirrhotic patients with Child Pugh class B or C have a high risk of IPPB. Thus, endoscopists should be cautious about performing colonoscopic polypectomy in those patients.





 XML Download
XML Download