

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Although advances in antimicrobial therapies have been achieved, approximately one-third of patients with active infective endocarditis require surgery to save the patient's life and eradicate the infection, for which the overall outcomes remain poor.1,2,3,4 Endocarditis affecting the aortic valve combined with abscess formation is particularly challenging to treat, and requires aggressive diagnostic and therapeutic approaches because of severe complications associated therewith, such as heart block, destruction of intervalvular fibrosa involving the mitral valve, fistula to other cardiac chambers, aortic pseudoaneurysm formation, and extrinsic compression of coronary arteries.5,6,7,8
Due to the aggressiveness of this disease and a wide spectrum of clinical presentations, according to the various complications, no randomized prospective study has been conducted thereon, and there are only a few retrospective studies. Therefore, we aimed to review our data to analyze 10-year clinical outcomes in patients who underwent surgery to treat active infective endocarditis combined with aortic root abscess.
MATERIALS AND METHODS
A total of 220 patients were surgically treated for infective endocarditis between February 1999 and June 2012 at Severance Cardiovascular Center, Yonsei University College of Medicine. Among these patients, data from 49 patients who underwent surgery for active endocarditis combined with aortic root abscess were retrospectively reviewed. Data were extracted from the hospital's computerized database, with additional information obtained through retrospective record review. The Institutional Review Board approved the study and waived the need for informed consent in consideration of the retrospective nature of the study.
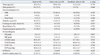
The infected valves were native in 29 patients and prosthetic in 20 patients. The patients' mean age was 50±14 years, and 36 patients were male. Surgery was performed in urgent or emergent cases in 15 patients (31%). The main indications for surgery included progressive heart failure causing hemodynamic instability in 41 patients (84%), large vegetation with recurrent septic embolism in 6 patients (12%), and early prosthetic infection (<60 days) in 2 patients (4%). Twenty-five patients (51%) had preoperative systemic embolic event, and 8 patients (16%) were in shock. Seven patients (14%) required renal replacement therapy for preoperative acute renal failure. Patient characteristics and preopera-tive echocardiographic data are described in Table 1.
Transthoracic echocardiography and transesophageal echocardiography were performed in all patients preoperatively, and coronary angiography was performed in 29 patients (59%), including 3 patients who exhibited regional wall motion abnormality on an echocardiogram or had a previous history of coronary artery disease. Aortic root abscess was diagnosed by preoperative transthoracic or transesophageal echocardiography in 43 patients (88%), and was detected during operation in the others.
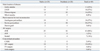
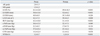
Microorganisms were identified in 33 patients (67.3%) preoperatively. Streptococcal species were the most common organisms in both types of prostheses (Table 2).
The abscess mainly involved the aortic annulus in 11 patients, left ventricular outflow tract in 18 patients, fibrous trigone in 16 patients, and mitral annulus in 4 patients. Five patients were complicated with formation of aortic false aneurysm, and 3 patients had fistula in the right atrium (1) or left atrium (2). In all patients, wide debridement of abscess and aortic valve repair or replacement with or without patch reconstruction of aortic root or annulus was performed (Table 3). The infected native or prosthetic valves were removed, and the abscess was radically excised along the edematous and potentially infected surrounding tissues. Special care was taken to minimize contamination of the operation field by changing surgical instruments and gloves after excision of all infected tissues. If a decision to reconstruct the aortic root was made, autologous pericardium was harvested and pretreated in 1.5% glutaraldehyde solution for 3 minutes, followed by further rinsing in normal saline for 3 minutes. All destructed tissues seen were excised, and pericardial patches were made 10-20% larger than the defect of the aortic root to be closed in order to minimize the chance of being detached due to tension. In cases of pericardial adhesion, bovine pericardium was used for reconstruction. In patients with extensive destruction of the annulus, a circumferential reconstruction of the annulus was performed, and the sutures for valve replacement were made through the reconstructed neo-annulus. Aortic valve replacement was performed with mechanical valves in 38 patients (78%), tissue valves in 7 patients (14%), and homografts in 3 patients (6%).
Patient clinical characteristics, echocardiographic parameters, and surgical data were obtained from review of medical records, and follow up was performed via reviewing hospital charts or conducting telephone interviews. One patient was lost to follow up; complete follow up was achieved in 97.6% (42/43) of all patients who survived.
All data are expressed as mean±standard deviation, frequency, or a percentage. Continuous variables were compared using the t-test, and categorical variables were compared using the χ2 or Fisher exact test. Survival was evaluated with the Kaplan-Meier method, and the log-rank test was used to compare the groups. All statistical analyses were performed using Statistical Package for the Social Sciences statistical software package, version 17.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
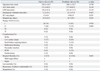
Patient characteristics for those with native valve endocarditis or prosthetic valve endocarditis were not statistically different (Table 1). Operation time, aortic cross clamp time, cardiopulmonary bypass time, intensive care unit stay, and hospital stay were also not different between the two groups (Table 4). Postoperative complications included stroke in one patient, low cardiac output in 9 patients, renal failure requiring dialysis in 3 patients, re-exploration for bleeding in 2 patients, pacemaker implantation in 1 patient, percutaneous cardiopulmonary support (PCPS) in 2 patients, and tracheostomy in 1 patient. Two patients who required PCPS eventually died. There was no significant difference in development of complications between the two valve types (Table 4).
Echocardiographic data showed a significant decrease in left ventricular ejection fraction (61.4±12.0% to 49.8±16.5%, p<0.001). However, there were significant improvements in left ventricular end diastolic dimension (58.8±11.8 mm to 52.6±8.2 mm, p<0.001), left atrial volume index (42.1±7.3 mL/m2 to 39.4±6.5 mL/m2, p=0.008), and right ventricular pressure (43.3±10.8 mm Hg to 31.1±9.8 mm Hg, p<0.001). New York Heart Association functional class was also significantly improved (mean 3.2±0.7 to 1.2±0.4, p<0.001) (Table 5).
Overall hospital mortality was 12.2% (6/49), and the causes of death included multi-organ failure in 4 patients and sepsis in 2 patients. Hospital mortality was higher for prosthetic valve endocarditis without statistical significance (Table 4).
The mean follow up duration was 68.7±40.4 months (range: 2-159 months), and there was no late death or recurrence of infective endocarditis during the follow up. One patient required reoperation for degeneration of bioprosthetic valve 4 years after the initial operation.
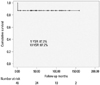
Overall Kaplan-Meier estimated survival rates at 1, 5, and 10 years were 87.2%, 87.2%, and 87.2% (Fig. 1). Kaplan-Meier estimated survival rate at 10 years was higher in native valve endocarditis than prosthetic valve endocarditis (92.9% vs. 78.9%, p=0.165) without statistical significance (Fig. 2).
DISCUSSION
Despite major advances in antimicrobial therapies, diagnostic technology, and surgical techniques, the mortality and morbidity of patients with infective endocarditis remain high.1,2,3 In contrast to infective endocarditis without root abscess, urgent surgical treatment to eradicate the infected tissue is mandatory to successfully treat patients with root abscess. Also, delay in surgical treatment often results in periannular complications such as fistula to other cardiac chambers, false aneurysms, heart block, destruction of intervalvular fibrous bodies, and involvement of mitral valve.4,5,6,7,8 Therefore, once an aortic root abscess is detected, urgent surgery is required, as antibiotics alone will fail to control the infection and delay in surgical treatment may cause fatal complications; such cases usually require a more complex operation. However, the results of surgical treatment in these patients are still unsatisfactory, with high early mortality and complication rates. The reason for high morbidity and mortality includes persistent infection, prosthetic valve dehiscence, metastatic infections, multiple organ failure, and death.9
As shown in our study, preoperatively identified microorganisms were mostly streptococcal species, which are relatively less aggressive, and many others had no microorganisms identified preoperatively (culture negative). This implicates that not only aggressive but also less aggressive microorganisms or culture negative endocarditis may result in extensive root destruction when initial diagnosis and appropriate medical or surgical treatment is delayed. Furthermore, many authors mentioned that the preoperative detection rate of paravalvular abscess with transthoracic echocardiography is very low, and due to surgical complexity, accurate preoperative diagnosis of aortic root abscess is important for proper preoperative surgical planning. Therefore, careful hemodynamic and clinical assessment of these patients with short term trans-esophageal echocardiographic follow up is mandatory to decide the proper timing and plan for appropriate treatment in patients with active aortic valve endocarditis.9,10,11
Surgical treatment in aortic root abscess is challenging, requiring the performance of complex procedures, and needs to be modified to deal with various complications. The most important aspect in the surgical treatment of these patients is radical resection of all infected tissues.9,12 The type of valve implanted seems less important than complete eradication of all infected and visually edematous tissues. Operations must be individualized because the pathology of aortic root abscess may vary. In particular, root abscess extending into the intervalvular fibrous body or into a prosthetic aortic and mitral valve is particularly difficult to treat, and in these cases, resection and reconstruction can be performed through the aortic root and dome of the left atrium.13,14
In our study, the operative mortality was 12.2%, which is similar to other studies. However, the late mortality and recurrent infection was very low, which is quite different from other previously published studies.1,4,9 Several factors might have influenced the results: first, less virulent streptococci were the offending microorganism in more than half of our patients, which is less virulent. Other studies that included a larger number of patients with staphylococcal infection or other more virulent organisms reported higher mortality and recurrence rate.9,15,16 Second, we strictly treated with intravenous antibiotics for at least 4 weeks postoperatively, even in culture negative patients. This might be associated with low recurrent rates of early and late endocarditis. Lastly, we only reviewed the patients who successfully underwent surgical treatment, and patients who refused operation due to multiple strokes or intracranial hemorrhages with comatose mental status or patients who died before operation due to unstable hemodynamics or delayed diagnosis were not included. Therefore, the mortality of the disease might have been underestimated.
The risk of early postoperative infection for mechanical and bioprosthetic valves is higher than that for homografts.17,18,19 In this study, mechanical valves were the most commonly used prosthesis, because a large portion of patients were young in age, homografts were not available in emergent situations, and the costs of homografts were too expensive; homografts were not covered by national insurance until the year 2011 in our country. However, the rate of recurrent infection was 0% in all patients, and a recent study established by Musci, et al.19 suggested that even though the results of homograft aortic root replacement is satisfactory with low recurrence rate, the risk of structural valve deterioration increases over time, especially in young patients, and reoperation remains a challenge. Therefore, mechanical valves seem to be a good substitute, even in active endocarditis with root abscess, if complete debridement of infected tissue can be achieved.
The main limitation of this study was the small sample size and its retrospective nature. However, due to the aggressiveness of this disease and the wide spectrum of clinical presentations, according to the various complications, no randomized prospective study can be easily performed. Nevertheless, our study may provide some information to clinicians who find it difficult to treat this aggressive disease.
In conclusion, surgical treatment for active endocarditis with aortic root abscess is still challenging, and was associated with high operative mortality. However, long-term survival was excellent, with good functional capacity after recovery from the early postoperative period. Preoperative accurate diagnosis, aggressive follow up for proper operative timing, and appropriate surgical strategy might improve early and long-term outcome in these patients.


 XML Download
XML Download