

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Maintaining proper physical activity or exercise is an important factor in reducing metabolic risks1 as well as obesity.2 In the modern global society, many people live under circumstances where physical activity or exercise is limited due to a sedentary lifestyle or daily job-related burdens, even though they recognize the importance of health and physical activity/exercise. Moderate-intensity cardiorespiratory exercise training (≥30 min per day, ≥5 days per week, for a total ≥150 minutes per week), vigorous-intensity cardiorespiratory exercise training (≥20 min per day, ≥3 days per week, for a total ≥75 minutes per week), or a combination of moderate- and vigorous-intensity exercise to achieve a total energy expenditure of ≥500-1000 MET/min/wk is recommended to maintain general health.3 Additionally, the number of studies assessing cost-effectiveness of exercise intervention in various diseases is still limited.4 Therefore, the exact measurement of physical activity is important. On the other hand, objective measurement of physical activity is difficult due to the fact that the exact description of movement that is robust to location on the human body itself is difficult to acquire.5
Triaxial accelerometers have been used to monitor physical activity or exercise in many clinical fields,6,7 partly because quantitative monitoring of physical activity in daily life has an important role. A triaxial accelerometer is a small device that can be carried or worn on the wrist, upper arm, waist, ankle, and other body sites. It permits an objective measurement of physical activity by Signal Vector Magnitude (SVM, expressed as cm/s2) and convert those measured values into physical activity-related energy expenditure (PAEE, expressed as kcal/kg/min).8,9 However, the past literature is unclear concerning the best body site to evaluate physical activity or PAEE by the use of a triaxial accelerometer, even though some accelerometer products were developed to wear on sites including the wrist, upper arm, waist, ankle, and hip. Because the exact monitoring of physical activity has a role in the behavior modification for the maintenance of proper physical activity or exercise,10 the body location of a triaxial accelerometer during exercise at different speeds is an important consideration. Therefore, this study was undertaken to determine and recommend the most appropriate site to wear a triaxial accelerometer during different exercise speeds in healthy Korean adults, with the goal of determining the best relationship between PAEE determined by cardiorespiratory gas analyzer and SVM measured by triaxial accelerometer.
MATERIALS AND METHODS
Participants
This study was conducted in the Department of Family Practice and Community Health, Ajou University Hospital, Suwon, Gyeonggi-do, Republic of Korea. Sixty six healthy adults (26 men and 40 women), 20-49 years of age volunteered for the study and were enrolled after providing informed consent. Exclusion criteria included pregnancy, current breast feeding in women, past and/or current history of heart disease or chronic lung diseases, dyspnea or chest pain by simple exercise, an evident myocardial ischemia, and arrhythmia or cardiomegaly in 12-lead electrocardiography (EKG). All participants received a medical interview and all EKGs were normal. The Institutional Review Board of Ajou University Hospital approved this study (AJIRB-DEV-DE2-10-298).
Study design
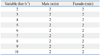
All measurements were conducted by a trained research nurse and research staff in the clinical trial center in Ajou University Hospital. All participants were requested to measure resting metabolic rate (RMR, mL/kg/min) for 5 min rest before exercise by cardiorespiratory gas analyzer. PAEE calculated by oxygen consumption also measured at different speeds on the treadmill adjusted by individual RMR. Oxygen consumption was measured by cardiorespiratory gas analyzer during exercise (walk or running, as subjects' habitual exercise) with different speeds (2, 3, 4, 5, 6, 7, 8, 9, and 10 km/h). Each was continued for 2 min, for a total of 18 min of exercise (Table 1). During exercise, the activity of exercise was measured as SVM by simultaneously applying four triaxial accelerometers on the wrist, ankle, upper arm, and waist. Accelerometer data and energy expenditure data were synchronized under the control of a computer system before measurement, which could control time set up. To acquire stable exercise data for each speed, the data of the first 50 sec and the last 10 sec in each 2 min exercise period were eliminated, since the posture of exercise during the first 50 sec and last 10 sec could be changed or influenced by the speed change, with the remaining 60 sec at each exercise speed being analyzed. All participants completed the study after 5 min rest under the close observation by the researchers. There were no adverse events during the study.
Measurement of RMR, PAEE, and SVM
RMR in mL/kg/min of each participant was measured using an Ultima PFX cardiorespiratory gas analyzer (Medical Graphic, St. Paul, MN, USA) after 5 min rest without fasting. This gas analyzer measures energy expenditure using the ratio of O2 to CO2. Pulmonary Exercise Ultima PF is indirect calorimeter that calculates respiratory exchange ratio (CO2·O2-1). Each participant wore the Ultima PF, while performing each activity and throughout the rest periods. The Ultima PF is a gas exchange system that measures ventilation, expired concentration of oxygen and carbon dioxide, which then estimates energy expenditure. The Ultima PF is small in size and lightweight, 36×33×36 cm and 12 kg. It has a range of ±18 L·sec-1, accuracy ±3% or 50 mL, whichever is greater (meets or exceeds ATS/ERS clinical performance standards), and resolution 8.64 mL·sec-1. For the RMR measurements, we used the latter half of the exercise period (2.5 min) to get the stable data. The reason for the omission of fasting was our view that the actual RMR without fasting is more important in daily life and is based on the oxygen consumption at rest, which is different from the basal metabolic rate. In addition to measuring RMR, we obtained two kinds of activity-related oxygen consumption (METs): Calculated METs and Actual METs. To calculate Actual MET, the measured oxygen consumption at a particular speed was divided by the individual RMR. For the Calculated MET, the measured oxygen consumption at each speed was divided by 3.5 mL/kg/min. Calculation of PAEE using oxygen consumption was based on the assumption that 1 liter of oxygen produces 5 kcal. Simultaneously, SVM was measured using a Fitmeter triaxial accelerometer (Fit. Life, Suwon, Korea), which was sum of total acceleration values of all three axes (x, y, z cm/s2). Usually, the accelerometer is worn on a belt positioned around the participants' ankle, waist, wrist, and upper arm. The Fitmeter accelerometer was positioned on the ankle, waist, wrist, and upper arm and the Actical accelerometer was positioned on the ankle, waist, and wrist. The Fitmeter accelerometer is a small (35×35×12 mm) and lightweight (13.5 g) devices that uses triaxial vector data in activity that measures accelerations in the range of -8-+8 G. These values correspond to the range in which most human activities are performed. Samples at a rate of 32 Hz and these values are then summed over a specified time period (epoch). The Fitmeter was worn on the ankle, waist, wrist, and humerus sites in nylon pouch that was secured to a belt provided by the manufacturer. The device was initialized using 1/32 sec epochs and converted to 1-min epoches for the data analysis. The results were downloaded directly to a PC compatible computer using a USB cable. The predictive accuracy of the algorithm in calculating Actual METs in the four selected body sites were 86.1-90.0%, which was considered high enough to represent the PAEE in different sites (Table 2).
Other measurements
Body weight and height were measured with a test gown using an automatic height-weight meter before each exercise test. Results were described by 0.1 cm and 0.1 kg, respectively. Body mass index (BMI) was calculated as weight (kg)/height (m)2.
Statistical analyses
All measured values showed normal distribution. General characteristics, calculated METs, Actual METs, PAEE, and SVM were expressed as mean±standard deviation. Actual METs were divided by three exercise speed categories: low (<3.00 MET), moderate (3.00≤MET<6.00), and high (MET≥6.00). The corresponding actual exercise speed of low METs was 2-4 km/h, moderate was 5-7 km/h, and high was 8-10 km/h. After the division of actual exercise speed, we used the partial correlation method to evaluate the association of PAEE using oxygen consumption with measured SVM in different wearing sites in the speed category after age, sex, and BMI adjustments. Finally, to determine the proper wearing site of triaxial accelerometer for the matching of PAEE with SVM at the different speeds, linear regression analysis was used. Data were analyzed using SPSS 18.0 (SPSS Inc., Chicago, IL, USA) with p<0.05 were considered statistically significant.
RESULTS
Clinical characteristics of study subjects
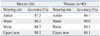
The mean age of participants in this study was 36.0±10.3 years, mean BMI was 23.4±3.0 kg/m2, and the measured RMR by cardiorespiratory gas analyzer after 5 min rest was 4.03±0.60 mL/kg/min (Table 3).
Comparison of METs, PAEE, and SVM at each exercise speed
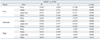
Mean actual METs of study subjects at exercise speed of 2, 3, 4, 5, 6, 7, 8, 9, and 10 km/h was 2.14±0.29, 2.56±0.38, 2.92±0.51, 3.56±0.72, 4.58±0.94, 5.96±1.08, 7.11±1.09, 7.77±1.19, and 8.40±1.17, respectively. For each exercise speed (values from each MET divided by 3.5 mL/kg/min), the Actual MET values were lowered than Calculated MET values. Therefore, the use of Calculated MET may overestimate the real exercise intensity. Mean calculated PAEE using oxygen consumption at exercise speeds of 2, 3, 4, 5, 6, 7, 8, 9, and 10 km/h was 1.45±0.40, 1.98±0.50, 2.43±0.61, 3.22±0.83, 4.51±1.14, 6.22±1.28, 7.68±1.42, 8.60±1.62, and 9.51±1.78 kcal/min, respectively. Measured SVM (cm/s2) by the Fitmeter triaxial accelerometer were also determined at the wrist, ankle, upper arm, and waist. All values increased as the exercise speed increased (Table 4). Overall relation between METs and SVM showed a high correlation with the ankle in low intensity (r=0.751, p<0.001), waist in moderate intensity (r=0.821, p<0.001), and ankle in high intensity (r=0.559, p<0.001) after adjustments with age, sex, and BMI.
Regression analysis of PAEE with SVM at different wearing sites for the exercise speed categories
Linear regression analysis was used to determine the most appropriate site to represent the association between PAEE using oxygen consumption and SVM measured using triaxial accelerometers during exercise at the designated speeds. Similar to the correlation analysis, results also showed prominent significant relation between PAEE and SVM. At low speed, moderate speed, and high speed, the most significant site was the ankle (R2=0.564, p<0.001), waist (R2=0.674, p<0.001), and ankle (R2=0.312, p<0.001), respectively, even though other sites also showed a significant relationship (Table 5).
DISCUSSION
In this trial to determine the best appropriate body location of a triaxial accelerometer, at low and high exercise speed, the ankle was the best site to represent that association. For moderate exercise speed, the waist was the best site to represent the association, even though other sites showed significant results.
Many studies have addressed the relationship between physical activity or PAEE and diseases such as osteoarthritis,11 early aerobic endurance training intervention in patients with coronary artery diseases,12 and weight loss maintenance behavioral intervention in a diverse population of high-risk patients,13 as well as an intervention study to evaluate the changes in visceral fat in a group of subjects who exercised vigorously with restricted caloric intake.14 In many clinical trials, however, accurate measurement of physical activity or PAEE is essential to guarantee research quality and reduce measurement error.
With careful consideration, individual differences of physical activity during exercise may exist, such as accelerometer wear time,15 measurement of physical activity in level-ground, treadmill walking at self-selected speeds16 or correlation of moderate-to-vigorous physical activity in different racial/ethnic groups, which might require culturally tailored strategies.17 In one study, to obtain optimal results with accelerometers in clinical trials, the authors recommended detailed protocols for monitor use, calibration of monitors and validation of data quality and use of validated equations for analysis.18 However, there has been no recommendation of the wearing site of triaxial accelerometer during exercise with different speeds or exercise intensities. In a study reporting the validity of three accelerometers during treadmill walking and motor vehicle travel,19 the researchers followed the recommendations of each accelerometer user guideline; in which the location of the accelerometer was the anterior thigh, ankle, and waist. Moreover, most clinical trials have been conducted based on the recommendations from the manufacturer and all participants were instructed to wear the device at certain locations. For example, consistent with the anatomical location of the anterior iliac spine, with the accelerometer is placed in a vertical position and the accelerometer worn on the belt or waistband of the clothing. Alternately, subjects were provided with a belt to secure the accelerometer to the proper location at the waist in the event that it could not be attached properly to their clothing,20 which seemed to be the standard wearing site. But, a triaxial accelerometer can be worn on various sites, such as wrist, ankle, upper arm, and waist using a band or other accessories.
The benefits and drawbacks of each body location site of the accelerometer can be summarized as follows. The accelerometer can be worn at the waist by securing the device to a belt or waistband of the clothing, or carrying the device in a pocket of tight skirts, pants, or trousers. The benefits of this method are a relatively high accuracy due to the central location, irrespective of a subject's sedentary behavior, and the option of hiding the accelerometer underneath the clothing for subjects concerned with the appearance of the device. An accelerometer positioned on the wrist or upper arm is likely to yield relatively low accuracy in a subject with a sedentary lifestyle because of an overestimation due to higher arm movement compared with whole body movement. However, a wrist or upper arm location carries the benefit of device use as an accessory or watch that makes it easy for a subject to monitor their calorie use and physical activity. Additionally, wearing an accelerometer on the upper arm enables music during exercise, if the accelerometer provides MP3 function. An accelerometer positioned on an ankle is better for accurate recording of subjects with a sedentary lifestyle, since leg movement is not typically as pronounced as arm movement in such subjects. But, an ankle location can be inconvenient to install and wear, which may lower the compliance of use.
Many clinical trials are likely to use the triaxial accelerometer worn on the waist or central core of the body. The present results indicate that this and other body locations are acceptable to represent the relationship between PAEE and SVM. Contrary to our expectation, however, the ankle was the most appropriate site for low speed and high speed exercise or intensity, and best reflected the relationship between PAEE and SVM in these conditions. For moderate speed exercise or intensity, the waist proved to be the most appropriate site. Given that accelerometers are sensitive to the changes in treadmill speed,21 the possible influence of changing speed should be taken into account when selecting an accelerometer site in terms of evaluating PAEE or SVM. Most of clinical trials are likely to compare physical activity or PAEE measured at a single accelerometer body location during the entire period of exercise, which creates the possibility of low correspondence with actual physical activity or PAEE, given the different speed measured by different wearing sites.
This study had some limitations. Study subjects were comprised of one ethnic group and healthy population. All participants were requested to engage in their exercise as their usual exercise posture or pattern, and so variations between individuals would occur. SVM might also vary with adoption of different postures during exercise at different speeds. There were several strengths of the study. The study is the first to evaluate the relationship between PAEE and SVM at different body locations at different exercise speeds. This study design revealed the benefit of different accelerometer body sites at different exercise speeds for most accurate measurements. The study also determined that measuring PAEE and SVM at one site during the entire period of exercise can potentially produce a measurement error. Therefore, to best evaluate PAEE and SVM, the body site should be considered with respect to the intended speed or intensity of the exercise, as well as proper adjustment of the wearing site. Furthermore, development of a proper algorism according to the wearing site is important. Actually, in real outdoor activity, wearing an accelerometer on the ankle may be inconvenient, therefore, wearing it on the waist for low and moderate speed exercise and the wrist for high speed exercise is recommended.
In conclusion, when measuring the PAEE and SVM at low (2-4 km/h or <3.00 METs) and high (8-10 km/h or ≥6.00 METs) exercise speeds, the ankle is the best site for an accelerometer. For moderate exercise speed (5-7 km/h or 3.00≤METs<6.00), the waist is the best site to represent the association between PAEE and SVM. Research designed to evaluate the PAEE and SVM at different speeds should consider the most appropriate site of wearing a triaxial accelerometer under the exercise conditions.


 XML Download
XML Download