

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The introduction of human leukocyte antigen (HLA) genotyping, particularly by high-resolution sequence-based typing (SBT), has significantly advanced patient's survival after hematopoietic stem cell transplantation.1,2,3 However, 'ambiguous' allele combinations by the SBT are often encountered in the determination of HLA genotypes in clinical laboratories.
The HLA loci are the most polymorphic genes in human, and are characterized by extensive gene duplication and recombination.4 The homology among HLA genes as well as the extensive polymorphism in exons encoding the peptide-binding domains can obscure exact identification of an individual's HLA alleles. When HLA genotyping is based on specific international immunogenetics (IMGT)/HLA database releases, genotyping systems that can assess fewer polymorphisms will generate more ambiguous HLA genotype data. In other words, ambiguous genotyping results may arise when the polymorphisms that distinguish between highly homologous alleles are located outside of regions assessed by a SBT system. However, it is not considered cost-effective to identify all of the polymorphisms that can distinguish closely related alleles, and ambiguities in alleles with identical antigen recognition sites are usually presumed to be clinically irrelevant.5 In these circumstances, HLA genotyping results can be ambiguous in that the results for a given sample can have many cis/trans combinations of polymorphic sites and may be consistent with more than two potential alleles at a given locus (cis/trans or phase ambiguity). A previous study reported that 41% of HLA-A and 24% of HLA-B allele typing showed phase ambiguity by SBT when exons 2 and 3 of the HLA-A and -B loci were analyzed.6
Currently, a total of 10533 HLA alleles are registered in the IMGT/HLA database release 3.15.0 (January 2014).4 As more HLA alleles are identified, more ambiguity would arise from SBT, and the potential for ambiguous results increases as advanced typing methodology identifies more polymorphisms outside the conventional targets of SBT assays. In addition, a genotype that is unambiguous, based on one past IMGT/HLA database release, may become ambiguous in the context of later releases due to the newly registered homologous alleles. In these contexts, distinctive allele and haplotype frequencies in a certain ethnic or population group depending on linkage disequilibrium as well as the frequencies of common alleles are usually referenced, and the most common allele combination is often reported when SBT gives ambiguous HLA genotypes.7 However, this approach is problematic when an individual actually has rare HLA alleles that are highly homologous with common alleles, leading to incorrect interpretation of genotyping results. In addition, ambiguities that include unsequenced regions defining null or low expression alleles could be clinically significant in some instances including searching for unrelated donors.8 The failure to identify an HLA null allele, which may not actually stimulate allogenic T cells and trigger graft versus host disease, may mislead into determining as an HLA mismatched case in the stem cell transplantation setting, although prevalence of HLA null alleles may be around 0.3%.9
Post hoc sequence-specific primer or sequence-specific oligonucleotide probe assay is necessary to resolve the ambiguity in some instances. The ambiguity in an SBT may also be resolved by a group-specific polymerase chain reaction (PCR) for the separated amplification of a single haplotype or by an SBT after haplotype-specific DNA extraction.10,11 Another approach to resolve the ambiguity from the SBT is to utilize the heterozygous ambiguity resolving primers (HARPs) for the sequencing step of an SBT. The AlleleSEQR® HARPs (Celera Co., Alameda, CA, USA) are designed to sequence single allele from the mixture of amplified PCR products, when the correct types of HARPs are chosen. In a recent report, 95%, 86%, and 60% of ambiguous results in HLA-A, -B, and -DRB1 typing, respectively, could be resolved using HARPs.12 In addition, recent advances in sequencing methodologies including massive parallel pyrosequencing would be helpful in exact HLA genotyping and resolving the ambiguity, but the next-generation sequencing methods are still expensive to perform in clinical laboratories and are also labor-intensive.13,14,15,16,17
Recently, a new commercial SBT assay was developed in order to resolve the ambiguity in the high-resolution HLA typing by employing multi-group specific sequencing to reduce cis-trans isomerism as well as increasing the number of sequenced exons in some instances. In this study, we evaluated this new SBT assay for its usefulness in reducing ambiguous HLA typing by comparing the results of this new test with those from other conventional SBT.
MATERIALS AND METHODS
Samples
Between February 2010 and January 2012, 50 DNA preparations that showed ambiguous allele combinations for at least two HLA loci among HLA-A, -B, -C, and -DRB1 in SBT with AlleleSEQR® HLA PCR kits (Celera Co., Alameda, CA, USA) were consecutively collected from 50 unrelated Korean individuals with written consents. DNA from whole blood samples was extracted using a QuickGene-Mini 80 nucleic acid isolation instrument with the QuickGene DNA whole blood kit S (FUJIFILM Co., Tokyo, Japan), and stored at -70℃ for later uses.
Conventional SBT assay
PCR and sequencing were performed for exon 2 of the HLA-DRB1 gene as well as exons 2 to 4 of the HLA-A, -B, and -C genes using AlleleSEQR® HLA-A, -B, -C, and -DRB1 PCR kits (Celera Co.) according to the manufacturer's instructions. Condon86 HARPs were also used in sequencing PCR for exon 2 of the HLA-DRB1 locus. The resulting nucleic acid sequences were read by an ABI 3100 DNA analyzer (Applied Biosystems, Foster City, CA, USA). All sequenced results were analyzed using Assign™ SBT software ver. 3.5.1.45 (Conexio Genomics Pty Ltd., Fremantle, Australia).
Multi-group-specific SBT assay
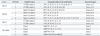
SBT was performed for all 50 samples again using AVITA™ plus HLA SBT kits (Biowithus Inc., Seoul, Korea) according to the manufacturer's instructions. The same DNA preparations that had been used for the AlleleSEQR® SBT assays were tested. The AVITA plus assay utilizes 2 or 4 PCR reaction tubes for multi-group-specific primer amplifications of HLA genes (2, 4, 2, and 4 tubes for the amplification of HLA-A, -B, -C, and -DRB1 loci, respectively). For example, different groups of HLA-B alleles are separately amplified in 4 different tubes in which different primer sets for different HLA-B groups are utilized for PCR amplification (Table 1). With the PCR products from each tube, sequencing PCR was performed for exons 1 to 5 of the HLA-A, and -C loci, exons 2 to 4 of the HLA-B locus, and for exon 2 of the HLA-DRB1 locus based on the Sanger sequencing principle, and then, nucleic acid sequences were read by an ABI 3730 DNA analyzer. The sequenced results were analyzed using BIOWITHUS SBT analyzer software ver. 2.7.4 (Biowithus Inc.).
Data analysis
The most probable HLA-A, -B, -C, and -DRB1 genotypes for the respective samples were determined based on the previous reports for allele frequencies in Koreans.18,19 Based on the reported HLA allele frequencies,18,20 expected genotype frequency in Korea and United States was calculated by the Hardy-Weinberg equation. All sequenced data from the two SBT assays were analyzed based on the IMGT/HLA database release 3.9.0 (July 2012). Ambiguous HLA alleles that had identical nucleotide sequences across the exons encoding the peptide-binding domains (exon 2 and 3 for HLA class I and exon 2 only for HLA class II alleles) were designated to the 'G' group and regarded as a single allele type. Alleles within the same G code were referred to as the current G group designation, which is available from the IMGT/HLA nomenclature website (http://hla.alleles.org/nomenclature/g_groups.html).
RESULTS
Overall agreement between the two SBT assays
When considering the allele frequencies in Koreans, the most common HLA-A, -B, -C, and -DRB1 genotypes for the respective 50 specimens, determined by the AVITA plus SBT kits, were all concordant with those from the conventional SBT assay.
Cases with ambiguous results
HLA genotypes analyzed in this study were determined according to the IMGT/HLA database release 3.9.0. The ambiguity in genotyped results and the total number of ambiguous allele combinations for each HLA locus by the SBT assays would change, depending on the version of the IMGT/HLA database release.
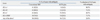
The numbers of cases with ambiguous results by the two SBT assays are summarized in Table 2. Among the four HLA-A, -B, -C, and -DRB1 loci for the 50 samples, an average of 3.28 loci per sample showed ambiguous results with the conventional SBT assay. The average numbers of possible allele combinations for HLA-A, -B, -C, and -DRB1 in the 50 samples were 6.92, 5.86, 5.08, and 2.64, respectively, with the conventional SBT, and the numbers were reduced to 1.44, 2.06, 3.84, and 1.60, respectively, with AVITA plus SBT. In addition, 48 (96.0%) samples among the 50 showed a reduction in the numbers of ambiguous allele combinations for at least one HLA locus. A total of 41, 43, 42, and 38 cases showed ambiguous results for HLA-A, -B, -C, and -DRB1 typing, respectively, with the conventional SBT, and for a total of 33 (80.5%), 31 (72.1%), 17 (40.5%), and 28 (73.7%) cases among them, ambiguity was resolved by the AVITA plus kits.
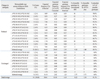
Based on the allele frequencies from the previous report,18 ambiguous allele combinations assessed in this study accounted for 50.6%, 14.9%, 41.0%, and 16.9% among all possible genotypes in Korean for HLA-A, -B, -C, and -DRB1 loci, respectively. The AVITA plus assay would be expected to resolve ambiguity for 34.4%, 11.7%, 15.5%, and 13.9% of the possible genotypes for HLA-A, -B, -C, and -DRB1 loci in the same population, respectively (Table 3,4,5,6).
Reduction in the number of ambiguous combinations according to HLA loci
The detailed genotypes and the numbers of possible allele combinations with both the conventional SBT and AVITA plus assay for HLA-A, -B, -C, and -DRB1 typing are summarized in Table 3,4,5,6, respectively. HLA-A*24:02:01G/*26:01:01, *02:01:01G/*11:01:01, and *02:01:01G/*24:02:01G accounted for 6 (14.6%), 5 (12.2%), and 5 (12.2%) cases with 10, 14, and 15 possible allele combinations, respectively, and the ambiguities were resolved in those cases by the AVITA plus assay. The average number of possible allele combinations with the conventional SBT was 8.22 for the 41 samples with ambiguity in the HLA-A locus, and the number was reduced to 1.54 with the AVITA plus test (Table 3). HLA-B*15:01:01G/*51:01:01 was the most frequent ambiguous allele type (5 cases, 11.6%) with 16 possible allele combinations, and ambiguities were also resolved in those cases with the AVITA plus assay. The average number of possible allele combinations by the conventional SBT was 6.65 for the 42 samples with ambiguity in the HLA-B locus, and the number was reduced to 2.23 with the AVITA plus test (Table 4). In the HLA-C genotyping, 17 (40.5%) out of 42 cases with ambiguous allele combinations by the conventional SBT showed a reduction in the numbers of possible allele combinations. The average number of possible genotypes with the conventional SBT was 5.86 in the 42 samples, and the number was reduced to 4.38 with the AVITA plus test (Table 5). Ambiguity in the HLA-DRB1 typing was also reduced or resolved with the AVITA plus SBT in 28 (73.7%) of the 38 cases that had ambiguous results with the conventional SBT assay, and the average number of possible genotypes with the AVITA plus assay in the 38 samples was reduced from 3.16 to 1.79 (Table 6).
DISCUSSION
The advances in HLA typing methods from serological tools using specific antibodies to molecular techniques are good examples of how technology has enhanced clinical practice and patient care. In this study, we performed high-resolution SBT using a new commercial AVITA plus assay, which was previously developed in order to resolve common types of ambiguous allele combinations that often arise from the conventional SBT. This new assay utilizes a group-specific PCR principle for single allele separation. A previous study reported a similar strategy for HLA-A typing with 10 primer sets for exons 2 and 3,10 and the AVITA plus assay expanded this strategy to HLA-B, -C, and -DRB1 typing with the inclusion of exons 1, 4, 5 of HLA-A and -C loci and exon 4 of HLA-B locus in the amplified regions. Consequently, the AVITA plus SBT assay resolved the ambiguity in 80.5%, 72.1%, 40.5%, and 73.7% of cases, which had showed two or more possible allele combinations with a conventional SBT for HLA-A, -B, -C, and -DRB1, respectively. The AVITA plus assay would also be expected to resolve ambiguity in more than 12% to 34% of all possible genotypes for each HLA locus in Korean population, when considered that there would be other HLA genotypes which were not included in our study.
Considering each HLA locus, the ambiguous results were resolved or the numbers of possible allele combinations were reduced mostly in the HLA-A typing, followed by HLA-DRB1 and -B. In our data, A*24:02:01G/A*26:01:01, A*02:01:01G/A*11:01:01, and A*02:01:01G/A*24:02:01G were common genotypes with ambiguities that were resolved by the AVITA plus assay. This assay uses two separate tubes for the amplification of the HLA-A locus, i.e., A*02, 25, 26, 29, 31, 32, 33, 34, 66, 68, 69, and 74 groups were designated to be amplified in a PCR tube containing specific primer sets for the respective HLA-A allele groups, while A*01, 03, 11, 23, 24, 30, 36, 43, and 80 groups were amplified in another tube (Table 1). Therefore, ambiguous typing that had arisen from the above-mentioned combinations could be resolved, because the A*24 or A*11 groups were amplified in a reaction tube that was different from one used for the amplification of A*02 or A*26. However, in cases where ambiguities were not resolved by the AVITA plus assay, all possible HLA-A allele combinations had been amplified in the same PCR tube, hindering the resolution of the ambiguity. In the same manner, the alleles, for which the ambiguity was resolved by the AVITA plus assay, were amplified in different PCR tubes for HLA-B, -C, and -DRB1 typing. The increase of the number of reaction tubes for more subdivided allele group-specific PCR of HLA can resolve the ambiguity in more cases, but would be labor-intensive and not cost-effective. Therefore, determining adequate numbers of reaction tubes for group-specific PCRs of the respective HLA loci is the key to cost-effectiveness, and the AVITA plus SBT assay may be efficient and cost-effective in reducing the ambiguity of HLA typing with the use of 2 or 4 reaction tubes per HLA locus. Actually, the cost for the AVITA assay is similar to that of the conventional SBT.
The AVITA plus assay and the HARPs technique have a common advantage in that preliminary or additional testing phases are usually not necessary to resolve the ambiguity, and both methods seem to be effective in resolving the ambiguous genotyping. However, the HARPs method requires additional labor and cost for the selection and use of proper sequencing primer sets, while the AVITA plus assay needs additional labor to manipulate more reaction tubes for the PCR amplification step than those required in a conventional SBT. In the case of HLA-A and -C loci, the AVITA assay has an another advantage of producing DNA sequence data covering exons 1 to 5 without additional sequencing reaction, and this data can be used to discriminate alleles that have different polymorphisms in the regions outside exons 2 to 4.
Unfortunately, considering cost-effectiveness, we included limited number of specimens, because HLA SBT is one of the most costly and labor-intensive tests in the clinical laboratory. Thus, rare HLA alleles could not be analyzed in this study. Based on the previously reported HLA allele frequencies in Korean,18 ambiguous genotyping results in this study would comprise 50.6%, 14.9%, 41.0%, and 16.9% of all possible genotypes with or without ambiguity in Korean population for HLA-A, -B, -C, and -DRB1 loci, respectively. We only included specimens from Koreans, thus further study for other ethnic groups would be needed to evaluate the usefulness of the AVITA assay in resolving ambiguity for HLA alleles uncommon in Korean. Actually, ambiguous HLA allele combinations analyzed in our study showed lower expected genotype frequencies for populations other than Korean (Table 3,4,5,6). We used different DNA sequencing platforms and SBT analysis softwares for the respective SBT assays. The quality of sequenced results and difference in the base calling processes for the respective instruments and platforms may affect the interpreted results. However, the most probable HLA-A, -B, -C, and -DRB1 genotypes for the respective specimens, determined by the two assays, were all concordant with each other. Thus, errors which could occur by the different platforms in this study would not significantly affect the results.
In summary, the AVITA plus HLA SBT test reduced the numbers of ambiguous cases with high-resolution HLA typing, particularly for the HLA-A, -B, and -DRB1 loci. In many cases, this assay did not require additional tests to resolve the ambiguity compared to the conventional SBT assay. Therefore, the AVITA plus HLA SBT assay would be useful for reducing ambiguity in the interpretation of HLA typing in clinical laboratories for transplantation.



 XML Download
XML Download