

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Combined antiretroviral therapy (cART) plays a critical role in suppressing viral titers and increasing CD4+ T lymphocyte counts, which translate to significantly reduced morbidity and mortality in HIV-infected individuals.1,2 However, it now appears clear that both HIV infection itself and cART are associated with a higher risk of stroke and metabolic disorders.3,4 In a cross-sectional study of 292 subjects, a CD4+ T-cell count less than 100 cells/mm3 was associated with a higher densirisk of metabolic syndrome.5 In parallel, metabolic complications were frequently observed after a few years of cART initiation.6 Many morphologic and metabolic changes correspond to metabolic syndrome criteria, according to the Adult Treatment Panel III (ATPIII) definition.7 These metabolic complications have been shown to be with an increased lifespan in HIV patients on cART, and naturally raise the question of whether HIV patients are at a higher risk for cardiovascular morbidity.8 Therefore, early detection of atherosclerosis may be necessary to prevent cardiovascular disease (CVD) in HIV-infected patients receiving cART.
Atherosclerosis is commonly observed in the carotid and coronary arteries.9 Measurement of carotid intima-media thickness (cIMT) and atherogenic plaque using ultrasound (US) is a noninvasive, sensitive and reproducible method for identifying and quantifying subclinical vascular atherosclerosis and for evaluating the risk of CVD.10 It is well known that cIMT level is a surrogate marker of atherosclerosis,11 and is significantly associated with risks for myocardial infarction, stroke and coronary heart disease in individuals without symptomatic CVD.12,13 Carotid plaque has also been shown to be associated with cardiovascular events in healthy populations, with a prognostic power similar to or better than that of cIMT.14-16 In addition, pathological carotid US findings, including the existence of plaques and/or a cIMT level of more than 0.9 mm, exhibited a highly significant direct association with all cardiovascular risk predictors including estimated Framingham risk score in cART-naïve HIV patients.17,18
Several previous studies have revealed that a decrease in estimated glomerular filtration rate (eGFR) is one risk factor for CVD19 and is correlated with cardiovascular mortality and morbidity in both high-risk groups20,21 and the general population.22
To the best of our knowledge, studies have yet to investigate risk factors of carotid plaque and subclinical atherosclerosis according to cIMT level in HIV-infected Asians receiving cART. In addition, there is little data on the clinical characteristics and associated factors of subclinical carotid atherosclerosis including eGFR among HIV-infected subjects in the Asia-Pacific region. The objective of this study was to evaluate the risk factors of asymptomatic carotid plaque and the associations between cardiometabolic factors and carotid atherosclerosis as measured by cIMT in HIV-infected Asians and to discern whether eGFR level is associated with cIMT or the existence of plaque.
MATERIALS AND METHODS
Study population and design
HIV-infected Koreans, who had continuously received cART comprising more than three antiretroviral drugs for at least six months with good clinical compliance to regular trimonthly visits at a university-affiliated tertiary care referral hospital (Seoul, Republic of Korea), were requested to participate in the present study. We prospectively enrolled a total of 145 HIV-infected patients, excluding participants with a medication history of anti-platelet agents or statins that can affect cIMT level and plaque. The study protocol was approved by the Institutional Review Board of the Clinical Research Institute of Severance Hospital. Written informed consent was obtained from each participant.
Carotid IMT measurement
Carotid US was performed by a single specialist to determine the extent of subclinical carotid atherosclerosis. Scanning of the extracranial common carotid artery, carotid bulb, and internal carotid artery in the neck was performed bilaterally from three different longitudinal and transverse projections.23 The average distance between the inner echogenic line representing the luminal-intimal interface and the outer echogenic line representing the media-adventitia interface was calculated by automatic IMT measurement software (Intimascope; Media Cross, Tokyo, Japan).23,24 The mean value of the bilateral average cIMT level was used as Mean-IMT in the analysis, and the greatest value among the measured cIMT levels was used as Max-IMT. For carotid US, a high-resolution real-time B-mode US with a 10-MHz linear probe (LOGIQ 7; GE Medical Systems, Milwaukee, WI, USA) was used. Carotid plaque was defined as the presence of focal wall thickening that was at least 50% greater than that of the surrounding vessel wall, or as a focal region with a cIMT greater than 1.5 mm that protruded into the lumen and was distinct from the adjacent boundary.25
Body composition measurement and collection of laboratory and clinical data
Height, body weight, waist/hip circumference, and systolic and diastolic blood pressure (BP) were directly measured on the day of carotid US evaluation in all participants. Body mass index (BMI) and waist-hip ratio (WHR) were calculated. Blood samples were obtained after a 12 h overnight fast. Circulating levels of total cholesterol (T-C), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglyceride (TG), fasting insulin, and fasting glucose were analyzed using an enzymatic colorimetric assay and lipoprotein electrophoresis (Hitachi, Tokyo, Japan). Homeostasis model assessment of insulin resistance as a marker for insulin resistance (IR) was calculated according to the following formula: [fasting glucose (mmol/L)×fasting insulin (µIU/mL)/22.5].26 CD4+ T lymphocyte count was measured by flow cytometry (Beckman Coulter, Fullerton, CA, USA), and plasma HIV-RNA viral load (VL) was obtained by Roche diagnostics (COBAS AMPLICOR HIV-1 MONITOR, version 2.42; Roche, Basel, Switzerland) with a lower detection limit of 40 copies per milliliter.
Kidney function was assessed through eGFR, which was calculated using the Modification of Diet in Renal Disease formula as follows27: 186.3×(serum creatinine-1.154)×(age-0.203)×(0.742 if female), with the serum creatinine concentration expressed as mg/dL. Clinical information including duration of known HIV infection and total duration of cART as well as all exposed antiretroviral drugs were collected. Based on the ATPIII criteria,7 metabolic syndrome was defined as the presence of three or more or the following components: 1) waist circumference >88 cm in women or >102 cm in men; 2) systolic BP ≥130 mm Hg or diastolic ≥85 mm Hg or use of antihypertensive medications; 3) TG ≥150 mg/dL or use of lipid lowering medications (niacin, fenofibrate, and gemfibrozil); 4) fasting blood glucose ≥100 mg/dL, physician diagnosed diabetes or use of diabetic medications; 5) HDL-C <50 mg/dL in women or <40 mg/dL in men. Hypertension was defined as the second component mentioned above.
Statistical analysis
All variables are expressed as the mean±standard deviation or number (percent), unless otherwise indicated. Statistical significance was set at p<0.05. Categorical variables were compared by χ2 analysis, and continuous variables with normal distributions were compared by Student's t test. We analyzed the continuous variables for normal distribution through the one-sample Kolmogorov-Smirnov test. Variables with p<0.05 in bivariate analysis were included in the logistic regression model for multivariate analysis to estimate the odds ratio (OR) of the risk of carotid plaque, along with the 95% confidence interval (CI). Single linear univariate correlations (Pearson's correlation coefficients) and stepwise multivariate regression analyses were performed to evaluate the relationships between the value of cIMT or eGFR and other variables. The predictive power of cIMT to discriminate patients who had carotid plaque from those who did not was assessed by calculating the area under the receiver operating characteristic (ROC) curve (AUC). The AUC ranged from 0.5 to 1.0, and the greater the AUC was, the better the variables were. The optimal cutoff values of cIMT were selected to maximize the sum of the sensitivity and specificity derived from the ROC curves and the AUC analysis (Youden index). All statistical analyses were performed using SPSS 12.0 software (SPSS Inc., Chicago, IL, USA).
RESULTS
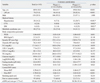
Thirty-four (23.4%) of the 145 patients had carotid atherogenic plaque. The mean age of the patients was 40.9±10.8 years, and 139 patients were male. The mean duration of known HIV infection was 53.0±44.7 months, and the mean total duration of cART was 36.7±29.5 months. The mean values of CD4+ T lymphocyte count and log10[plasma HIV-RNA VL] at the time of cIMT measurement were 349.1±176.2 cells/µL and 1.79±0.66 copies/mm3, respectively (Table 1).
Patients with carotid plaque were significantly older (49.0±10.4 yrs vs. 38.4±9.7 yrs, p<0.001) and had a higher prevalence of hypertension (38.7% vs. 7.3%, p<0.001), cerebro-vascular attack (CVA) (12.9% vs. 0.0%, p=0.002), diabetes mellitus (12.9% vs. 1.8%, p=0.021) and metabolic syndrome (41.2% vs. 23.4%, p=0.043), compared to patients without plaque. WHR was significantly higher in patients with carotid plaque than in those without (0.88±0.05 vs. 0.85±0.04, p=0.001) (Table 1).
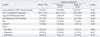
Among the serum lipid profiles, glucose, and IR parameters, T-C (181.6±36.7 mg/dL vs. 168.8±29.6 mg/dL, p=0.039), LDL-C (87.2±24.4 mg/dL vs. 74.9±25.3 mg/dL, p=0.033), glucose (106.9±25.6 mg/dL vs. 97.7±10.8 mg/dL, p=0.003), and fasting glucose-insulin ratio (13.09±13.87 vs. 8.41±7.63, p=0.023) were significantly higher in patients with carotid plaque than in those without. In addition, the carotid plaque group had a higher cIMT level (Mean-IMT; 0.68±0.17 mm vs. 0.56±0.09 mm, p<0.001 and Max-IMT; 0.82±0.22 mm vs. 0.66±0.11 mm, p<0.001) and lower eGFR (90.58±19.14 mL/min per 1.73 m2 vs. 97.22±14.59 mL/min per 1.73 m2, p=0.033) (Table 1). However, variables associated with HIV infection and cART were not significantly different between the groups (Table 2).
In the multivariate logistic regression model to identify risk factors for carotid artery plaque in HIV-infected patients receiving cART, older age (older than 40 years, OR 6.16, 95% CI 1.09-34.88, p=0.040), hypertension (OR 12.62, 95% CI 1.72-92.49, p=0.013), and higher LDL-C level (OR 1.08, 95% CI 1.01-1.16, p=0.039) were identified (Table 3).
The ability of Mean-IMT and Max-IMT to predict carotid artery plaque was further examined by ROC curve analyses. The AUCs for Mean-IMT and Max-IMT were 0.74 (95% CI 0.65-0.84, p<0.001) and 0.76 (95% CI 0.67-0.85, p<0.001), respectively. The cut-off level for the greatest sensitivity and specificity for Mean-IMT was 0.62 mm (sensitivity=0.59 and specificity=0.82), and that for Max-IMT was 0.71 mm (sensitivity=0.61 and specificity=0.76) (Fig. 1).
The levels of eGFR were inversely associated with Mean-IMT (r=-0.379, p<0.001) and Max-IMT (r=-0.389, p<0.001). Correlations between cIMT and clinical and metabolic variables are shown in Table 4. Max-IMT and Mean-IMT had a significantly positive correlation with age (r=0.591, p<0.001, and r=0.589, p<0.001, respectively), BMI (r=0.189, p<0.024, and r=0.168, p<0.044 respectively), WHR (r=0.372, p<0.001, and r=0.353, p<0.001, respectively), T-C (r=0.282, p=0.001, and r=0.242, p=0.003, respectively), LDL-C (r=0.258, p=0.006, and r=0.208, p=0.026, respectively), and fasting glucose (r=0.292, p<0.001, and r=0.294, p<0.001). In addition, the total duration of cART was significantly positively associated with Max-IMT and Mean-IMT (r=0.175, p=0.036, and r=0.177, p=0.034, respectively) in univariate analysis. In the multiple stepwise regression analyses, age (p<0.001 and p<0.001, respectively), T-C (p=0.003 and p=0.031, respectively), and fasting glucose (p=0.012 and p=0.009, respectively) remained significant clinical factors independently associated with Max-IMT and Mean-IMT (adjusted R2=0.384 and 0.345, respectively) (Table 4).
DISCUSSION
The present study revealed that older age (≥40 years), hypertension and higher LDL-C level are the independent clinical factors associated with the existence of carotid plaque in HIV-infected Koreans receiving cART. In addition, we confirmed that Max-IMT and Mean-IMT are significantly associated with the existence of carotid plaque and found that cIMT is correlated with traditional CVD risk factors in HIV-infected Koreans.
According to our multivariate analysis, the presence of documented hypertension and a 1 mg/dL increase in LDL-C were associated with 12.62 and 1.08 times higher risk of carotid plaque, respectively. In addition, older patients with HIV demonstrated a greater incidence of carotid plaque (especially those over 40). It is generally well accepted that hypertension and dyslipidemia promote atherosclerosis and consequently increase IMT in non-HIV-infected individuals.28 Prospective studies of large populations have reported a correlation between circulating concentration of total cholesterol and LDL-C with IMT in both non-HIV-infected Caucasian28 and Eskimos.29 Also, older age is known to be a major risk factor for the development of CVD.30 Endothelium-dependent dilation of vessels becomes impaired with age,31,32 and is thought to contribute to the age-associated increase in CVD risk.30 In our study, we observed similar associations between hypertension, LDL-C, age and carotid plaque in HIV-infected patients receiving cART.
The results of our study reveal that the presence of subclinical carotid plaque is a frequent occurrence among HIV-infected patient receiving cART (23.4%). Our present observation, however, could be limited by the absence of age-matched HIV non-infected controls. Nevertheless, this high prevalence is in line with other previous observations,33,34 and only 6.7% of subclinical carotid lesions have been observed in an age-matched control group of 104 HIV-negative subjects. Furthermore, 20.9% of subclinical carotid lesions have been reported in HIV-infected patients naïve to cART.18
Although the wide performance of cART has prolonged the life expectancy of individuals infected with HIV,35 the accelerated onset of CVD has emerged as a concerning complication of chronic HIV infection and long-term use of cART.36 Moreover, there is increasing evidence supporting the initiation of cART in asymptomatic HIV-infected patients and a CD4+ T lymphocyte count >500 cells/mm3.37 It is, therefore, increasingly more relevant to stratify patients for CVD risk when cART is being initiated or when treatment regimens are being adjusted.38 Arterial stiffness, a marker of CVD and an independent predictor of its corresponding risk, is associated with impaired endothelial function.39 HIV may affect the vasculature directly via endothelial damage,40 and the virus-mediated inhibition of cholesterol efflux from macrophages with consequent reduced HDL-C levels,41 which promotes arterial stiffness and contributes to atherogenesis.42 Furthermore, HIV treatment, especially protease inhibitors may accelerate atherosclerosis especially due to metabolic side effects including dyslipidemia and IR.43,44 However, we found that subclinical carotid atherosclerosis was not associated with duration of HIV infection or cART regimen. Any association of HIV with atherosclerosis remains vague because of discrepant findings among these studies and the likelihood of bias affecting some study results. cART induces not only metabolic effects including dyslipidemia, but also antimetabolic effects such as recovery from immunosuppression and HIV VL suppression. These effects might explain our results that HIV and cART were not associated with carotid atherosclerosis.
A non-dipping BP profile of abnormal diurnal BP rhythm and a reduced nocturnal BP fall was highly prevalent in cART-naïve HIV patients. And this pattern is currently regarded as a risk factor in its own right for cardiovascular events and target organ damage.45 It has been suggested that the mechanism of a non-dipping pattern involves the association of non-dipping with salt-sensitive forms of hypertension, renal function impairment and mineralocorticoid-induced forms of hypertension, but this is not yet clear.46 In our study, we could not check diurnal BP rhythm, and a BP pattern in HIV-infected patients receiving cART is warranted.
In the present study, we found that the cut-off levels of Max-IMT and Mean-IMT were 0.71 mm and 0.62 mm, respectively, for predicting the presence of carotid plaque. For the same BMI or waist circumference, Asians have a higher prevalence of hypertension and, a higher percentage of body fat, diabetes and dyslipidemia as well as clustering of these risk factors, compared with Caucasians.47-50 Although there are now ethnic-specified definitions for obesity,47 these cutoff points do not take into consideration the possible interethnic differences in body build and body fat distribution among different Asian ethnic groups.49,50 Considering interethnic differences of metabolic complications, the results of our study suggest that the cut-off values of Max-IMT and Mean-IMT might be useful for early detection of carotid atherosclerosis in Asian patients with HIV.
We also observed significant correlations between cIMT and other classical CVD risk factors such as age, T-C and fasting glucose. Increasing cIMT is known to be closely related with systemic atherosclerosis, including CAD and CVA. Many prospective studies have shown that the development of cIMT progresses to cardiovascular events.11,51,52 Therefore, elevated T-C and fasting glucose may account for early atherosclerosis in HIV-infected patients.
There are several limitations to our study. The study design was cross-sectional, which means that we cannot infer causality. Future prospective studies are required to evaluate the predictive power of risk factors on the future risk of CVD and all-cause mortality in a large multiethnic cohort. Additional limitations include the lack of an HIV-seronegative control group for comparison.
In spite of these limitations, this study has clinical significance since it is the first report to evaluate the relationships between carotid atherosclerosis and metabolic risk factors in Asian patients with HIV. In conclusion, we demonstrated that the presence of hypertension, high LDL-C and old age are independent clinical factors of carotid plaque among HIV-infected Koreans. Future studies on the process of atherosclerosis in HIV-infected patients receiving cART are needed, including direct comparison between multiethnic HIV-infected patients and non-HIV-infected subjects.



 XML Download
XML Download