

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Prostate cancer is the most common cancer among men in Western countries and the associated mortality has been high since the 1990s.1 In contrast, prostate cancer was not regarded as an issue in Asia due to a low incidence rate.2 However, a recent rapid increase in the incidence of prostate cancer in Asia has drawn the attention of many urologists in Asia to investigate new treatments for prostate cancer and to actively participate in prostate cancer studies.
In Korea, the prevalence of prostate cancer has quadrupled from 2002 to 2008, and the increased incidence rate is highest in total forms of malignancy.3 Environmental elements, such as increased population age due to the rise in average life expectancy, change to Western dietary habits, medical development of laboratory diagnosis and prostate-specific antigen (PSA) screening campaigns by the Korean Urologic Association (KUA) and other health organizations have helped to publicize the increase in prostate cancer in Korean patients.4,5 Moreover, the introduction of robotic surgery in 2006 has increased the awareness of prostate cancer in the general public and provided another option for the management of patients with prostate cancer.
Despite the increase of the prostate cancer incidence and the emergence of the robotic system in Korea, there are no recent published data regarding the practical and clinical changes in Korean prostate cancer patients. Therefore, we analyzed the database of registered prostate cancer patients from 2006 to 2010 in our outpatient clinic to investigate changes in clinical characteristics and the trends of prostate cancer management in order to generate a preliminary report for the Korean prostate cancer population.
MATERIALS AND METHODS
We analyzed a database of prostate cancer patients in the outpatient clinic from January 2006 to November 2010. Patients who registered for a second opinion for prostate cancer treatment and those patients that were lost after diagnosis were excluded from the study. Data including information on patient demographics, disease staging, choice of initial management and treatment of follow-up course were reviewed. Pathologic staging and clinical staging were determined in accordance with TNM categories as published in 2003.
For this present analysis, patients were stratified into localized prostate cancer (LPC), locally advanced prostate cancer (LAPC), advanced prostate cancer (APC), and hormone refractory prostate cancer (HRPC) based on the pathologic stage. The initial management of prostate cancer after diagnosis was also stratified into retropubic radical prostatectomy (RRP), robot assisted laparoscopic radical prostatectomy (RALP), radiotherapy (RT) only, radiotherapy with hormone therapy (RT+HT), primary hormone therapy (HT), and watchful waiting (WW). For the analysis of the trend change in prostate cancer, the proportion of treatments for prostate cancer patients by operation (OP), OP+RT, OP+HT, RT, RT+HT, HT, and WW in the outpatient clinic registration database were assessed within the designated study period.
RESULTS
In total, 546 men were registered with prostate cancer in our institute from January 2006 to November 2010. These patients visited 9053 times for prostate cancer treatment during the study period. Among them, total 417 men were newly diagnosed during the study period. Another 129 men were diagnosed and registered before 2006. of the 417 patients newly diagnosed, 17 patients were lost after prostate cancer diagnosis using the prostate biopsy and 14 patients were registered in our institute for a second opinion and were lost after just one visit. The newly diagnosed prostate cancer patients during study period comprised 386 men.
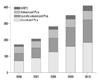
Between 2006 and 2010, the number of prostate cancer registrations increased more than 2 times from 173 to 408 men. The proportion of LPC and LAPC increased from 67.6% in 2006 to 79.1% in 2010. However, the total number of APC and HRPC patients showed no significant change, and actually declined from 33% to 21% (Fig. 1).
In newly diagnosed patients, the prostate cancer stage classifications were 43.5% LPC, 36% LAPC, and 20.4% APC. According to the distribution of initial management chosen by the patients, the proportion of men undergoing RALP was 48.9% and 10.3% opted for RRP; 10.6% of patients chose RT+HT as the initial treatment, and 26.4% chose primary HT.
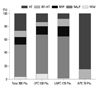
In the LPC group, the distribution of initial management modalities was 59.5%, 11.9%, 7.1%, and 13.7% treated with RALP, RRP, RT with HT, and primary HT, respectively. In the LAPC group, the distribution of initial management techniques was 64%, 14.4%, 12.2%, and 8.6% for RALP, RRP, RT with HT, and primary HT, respectively. With the LPC and LAPC groups, WW was chosen by only 4.5% as the initial treatment for the prostate cancer (Fig. 2).
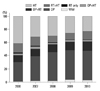
The trends for prostate cancer patients registered at our outpatient clinic are shown in Fig. 3. In 2006, 43.4% of patients were followed-up in our outpatient clinic after operation (RRP or RALP) with or without biochemical recurrence as the main treatment modality. Per annum, this proportion steadily increased to 51.9%, 56.8%, 60.3%, and 61.5%. By contrast, the primary HT group declined from 41% in 2006 to 23% in 2010.
DISCUSSION
Many reports have documented RALP is the choice of treatment for the localized prostate cancer. In the United States, RALP was performed only 10% of the total number of radical prostatectomies in 2006. However, the proportion had increased to more than 65% in 2008 through 2009.6 The same phenomenon was also reported in Korea, where RALP was increased dramatically from 8% to 77% between 2005 and 2008.7 In Korea, robot-assisted laparoscopic radical prostatectomy using the DaVinci® robotic system (intuitive surgical Inc., Sunnyvale, CA, USA) was introduced in 2005.
According to a 2010 report from the National Evidence-based Healthcare Collaborating Agency, Korea becomes the fifth largest nation in the world with robotic surgical equipment. They reported that after the Korean Food and Drug Administration (KFDA) approval in 2005, the urologic robot surgery performance cases were estimated to be 6000 cases on October, 2010.8 However, during the study period, we performed RALP in only 189 cases after equipment of the robotic system, even though our institute became the second in Korea to initiate the use of robotic surgery in 2007. According to report form the Health and Welfare statistics,9 the large number of the patients who newly diagnosed prostate cancer is registered for treatment in hospitals that rank among the top 4 urologic departments in Korea. For this reason, most RALP have been performed intensively in a limited number of hospitals in Korea. Nevertheless, we found interesting changes in the clinical characteristics and trends of prostate cancer management.
First, the registration of prostate cancer patients in our institute has increased more than 2 times during 5 years. Especially in LPC and LAPC, the number of prostate cancer patients increased by 79% in 2010 compared to 67% in 2006. Second, the proportion of operations including RALP and RRP as initial treatment choice was the highest in comparison to other treatments. Lastly, this result brought about the gradual increase of the patients who had underwent operations as the main treatment modality in outpatient clinics. This also drove the patients who treated with the adjuvant therapy including RT or HT due to biochemical recurrence to increase gradually. In contrast, we found that the number of the patients who chosen primary HT had decreased. We suspected that these changes were due to not only the effect of the robotic surgery system but also the increase of the prostate cancer incidence in Korea.
Recently, the increase in the rate of prostate cancer was reported at almost 12% per annum, which is the highest rate increase relative to the five major cancers in Korean men including stomach cancer, colon cancer, lung cancer, liver cancer, and prostate cancer.3 The prevalence rate of prostate cancer has increased threefold from 5.5 men out of 100000 in 2000 to 14.3 men out of 100000 in 2005.3 According to the National Health Insurance Corporation, the number of prostate cancer patients in outpatient clinics increased from 4843 men in 2002 to 20498 men in 2010.9
The number of prostate cancer patients in Korea increased sharply due to a rapid increase in the elderly population, a change in dietary habits to a Western-like diet, the development of diagnostic techniques using PSA, the continuous promotion of prostate cancer by the mass media, and the BLUE RIBBON campaign for PSA screening organized by the KUA. The Korean government does not include prostate cancer in the free cancer-screening program as of yet, but if this does occur, the increase in prostate cancer incidence is expected to increase. For these reasons, the detection of prostate cancer could be more likely in earlier stages in men. An increase of the early diagnosis in younger men at the LPC and LAPC stage would allow the patients to consider operations including RALP and RRP as the initial management tool.
The proportion of WW as the initial therapy was only 3.6% in the total group (14 of 386 patients). In 14 patients, 13 patients were LPC stage. The proportion of WW was similar to the results reported from Japan and the United States.10,11 In contrast, conservative treatment including WW was the main modality in low risk LPC in the United Kingdom.12 In Korea, despite the indolent nature of prostate cancer, patients strongly desire definite treatment for a complete cure and urologists do not want to face legal problems if the disease progresses without treatment even though WW is an option for prostate cancer. Therefore, the United Kingdom-like trend for prostate cancer management is not available in Korea.
We found a different approach to prostate cancer treatment when comparing with Japan. The authors of a Japanese study reported that the initial choice of treatment for prostate cancer was mainly primary HT.13 Hinotsu, et al.14 reported that primary HT has been used in Japan for over 80% of low-risk patients. However, our findings indicate that the main treatment after diagnosis of prostate cancer is radical prostatectomy including RRP and RALP. This finding is not true for only our institute.7 The advantages of robotic surgery are introduced to patients intensively by the mass media, and radical surgery for prostate cancer is simultaneously advertised as a definite curative option. Moreover, Korean cancer patients tend to prefer a complete cure with a radical operation over daily hormonal medications and monthly hormonal injections. This trend would decrease the proportion of primary HT gradually in Korea.
Recently, the National Comprehensive Cancer Network published an Asian Consensus Statement on prostate cancer. In statement, 10 the treatment options for patients with negative metastasis are listed in order of preference as RT+HT, HT, and observation.15 However, considering all of the findings; this statement is not consistent with the present analysis. Our present analysis shows that the practical guidelines for treating prostate cancer support operations over a pharmacologic, radiation, or conservative management. Our trend of prostate cancer management is similar to that in the United States16 and there is a vast difference with regard to initial management preference compared to Japan, despite its close geographic proximity.13
The present study has some limitations. The period for analysis needs to be followed-up for longer than 2006 in order to analyze the trend of prostate cancer incidence for the early 2000s, and the database of our institute does not represent the entire status of the Korean population. To overcome these limitations, data form a large-scale observational longitudinal study cohort such as the cancer of the prostate strategic urologic research endeavor (CaPSURE) in United States is needed.17 The CaPSURE represents not only United States but also serves as one of the most famous and reputable study groups in the scope of urology. Japan also has a large-scale database of observational longitudinal data to investigate safe and effective hormone therapy in prostate cancer patients.18 Although the Japan study group of prostate cancer (J-CaP) does not represent the entire status of prostate cancer in Japan, they could represent trend and characteristics of primary hormone therapy in Japanese prostate cancer patients can be investigated. There is still no large-scale database being used to determine the nationwide trend of the management and changes in the clinical characteristics in Korea. However, we believe that a large Korean prostate cancer database will come soon and prove the change of the prostate cancer trend in Korea like our present study.
 XML Download
XML Download