

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Lung cancer is one of the most common malignancies and is a leading cause of cancer-related mortality worldwide.1,2 Recent development and approval of the epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors (TKIs), gefitinib and erlotinib, have significantly changed treatment outcomes in advanced non-small cell lung cancer (NSCLC).3 Patients with adenocarcinoma who are of Asian origin, female gender, and with no history of smoking predict a strong response to EGFR-TKIs.4 In addition, molecular studies show a number of biomarkers associated with tumor sensitivity to EGFR-TKIs.5-9 The presence of EGFR mutations, in particular, is associated with dramatic response to EGFR-TKIs.5-7,9,10 On the other hand, somatic mutations of the KRAS oncogene may predict poor EGFR-TKI responsiveness.3,11-17
The RAS gene subfamily encodes a group of guanosine triphosphate-binding proteins, which are essential components of the EGFR signaling cascade and play important roles in tumor pathogenesis.18,19 Single nucleotide mutations in KRAS codons 12 and 13 compromise guanosine triphosphatase (GTPase) activity.19,20 Such mutations may not only impair the intrinsic RAS GTPase activity, but also confer resistance to GTPase-activating proteins. Consequently, RAS accumulates in its active GTP-bound state, resulting in constitutively activated RAS signaling.21 KRAS mutations are frequently observed in lung adenocarcinomas and may be smoking-related, while KRAS mutations are uncommon in squamous cell lung carcinomas and lung cancers in never-smokers.18,22,23 Interestingly, KRAS mutations occur more commonly in the lung tumors of Caucasian patients than in those of East Asians.21
Since KRAS mutations are common in NSCLC and cigarette smoking is a frequent cause of NSCLC, KRAS mutations are hypothesized to be related to tobacco exposure.18 However, studies to test the association between cigarette smoking and KRAS mutation often lack detailed patient smoking histories and include relatively small numbers of never-smokers.
The validity of the KRAS mutation as a predictive biomarker for lung cancer response to EGFR-TKIs remains uncertain. Several reports support an association between the presence of KRAS mutation and poor response to EGFR-TKIs.11-13,15,16,24,25 On the other hand, results of the IRESSA Non-Small-Cell-Lung Cancer Trials Evaluating Response and Survival Against Taxotere trial show no difference in overall survival (OS), progression-free survival (PFS), or response rate according to KRAS mutation status.10,26
Few studies provide detailed correlations of KRAS mutations with smoking history or treatment outcome following treatment with EGFR-TKIs. We, therefore, conducted this study to determine the relationship of cigarette smoking with the frequency and qualitative differences in KRAS mutations in the lung adenocarcinomas of Korean patients. In addition, based on the concurrent mutational analysis, we evaluated the power of KRAS mutation status to predict treatment outcome with EGFR-TKIs in these patients.
MATERIALS AND METHODS
Study population and data collection
For this study, we enrolled 200 consecutive patients who had lung adenocarcinomas that were newly diagnosed and histologically confirmed between October 2007 and April 2010 at the Yonsei Cancer Center in Seoul, Korea and who were available for genetic analysis. The tumor histology was classified using the World Health Organization criteria.27 Detailed smoking histories were prospectively obtained from these 200 patients with NSCLC according to a standard protocol that included the following questions:28 Have you smoked more than 100 cigarettes in your life? Are you currently smoking? How many years have you been a regular smoker; and on average, how many cigarettes did you smoke per day? The smoking questionnaire was administered by a medical oncologist. Based on their smoking status, patients were categorized as never-smokers (<100 cigarettes in their lifetime), former-smokers (quit ≥1 year ago), or current-smokers (quit <1 year ago). Pack-years of smoking were defined as [(average number of cigarettes per day/20)×years of smoking]. For all patients, medical records were reviewed to extract data based on their clinicopathological characteristics. For patients with metastatic disease, we examined treatment regimens, overall response rates, and survival outcomes (PFS, OS). Clinical responses were assessed every two cycles using computerized tomography and were classified using the Response Evaluation Criteria in Solid Tumor (RECIST version 1.0).29 PFS was measured from the first day of treatment with EGFR-TKI to progression or death, while OS was measured from the date of treatment with EGFR-TKI until the date of death. Patients were censored on July 31, 2010, if alive and progression-free. Patients with no known date of death were censored on the date of their final follow-up. This study was approved by the Severance Hospital Institutional Review Board. All patients signed a written informed consent for genetic analysis.
EGFR and KRAS mutation analysis
Nucleotide sequencing of the kinase domain of EGFR (exons 18 to 21) was performed using nested polymerase chain reaction amplification of the individual exons.17 The sequencing protocol has been previously described.13,28 Specific mutations in KRAS exon 2 (codons 12 and 13) were identified from published data.13,28
Statistical analysis
Data were summarized using standard descriptive statistics. Significant differences in the variables between genotypes were tested using the χ2 test, Fisher's exact test, and t-tests where appropriate. The Kaplan-Meier method was used to estimate PFS and OS, and the differences between genotypes were compared using the log-rank test. The adjusted hazard ratios (AHRs) for the risk of progression or death with treatment were compared between genotypes using a Cox regression model that included age, gender, smoking history, and performance status as independent variables. All p values were two-sided.
RESULTS
KRAS mutation and smoking history
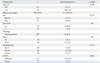
This entire cohort included 93 men and 107 women patients with a median age of 58 years (range: 28-84). All histologic types were adenocarcinomas (Table 1). Based on smoking history, patients were classified into three groups: never-smokers (n=120, 60%), former smokers (n=40, 20%), and current smokers (n=40, 20%) (Table 1).
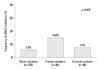
Among the 200 patients, 87 (43.5%) had EGFR mutations and 16 (8%) had KRAS mutations in codons 12 (n=14) or 13 (n=2). One patient had both an EGFR mutation (exon 19, del 2235-2249) and a KRAS mutation (Gly12Cys, GGT→TGT). Patients with a KRAS mutation and those with wild-type KRAS (WT) did not differ in baseline characteristics including age, gender, Eastern Cooperative Oncology Group (ECOG) performance status, histology, stage at initial diagnosis, and smoking history (Table 1). Presence of the KRAS mutation was not significantly related to smoking history (Mantel-Haenszel χ2 test, p=0.435). KRAS mutations were identified in 5.8% (7/120) of never-smokers, 15% (6/40) of former smokers, and 7.5% (3/40) of current smokers (Fig. 1). Moreover, age at first cigarette, total pack-years, total smoke-years, and smoke free-years were not correlated with KRAS mutations (Supplementary Fig. 1).
Never-smokers were significantly more likely than former- or current smokers to have a transition mutation (substitution of a purine for a purine, e.g., G→A or a pyrimidine for a pyrimidine, C→T) than a transversion mutation (substitution of a purine for a pyrimidine or conversely, G→T or G→C), which are known to be smoking-related (p=0.011) (Table 2).
Treatment outcome with EGFR tyrosine kinase inhibitors
Of 153 patients with advanced lung adenocarcinoma, 97 received EGFR-TKIs (Supplementary Table 1). Among them, one patient had both EGFR and KRAS mutations detected and received a combination treatment of erlotinib and sorafenib in a clinical trial. This patient showed a partial response (PR) lasting more than 15 months. Among the 41 patients with EGFR mutations, 25 (61.0%) showed a clinical response to EGFR-TKIs, 11 (26.8%) had stable disease (SD), and 5 patients (12.2%) had progressive disease (PD). In the 8 patients with KRAS mutations, one (12.5%) showed a clinical response to EGFR-TKIs, 2 (25.0%) had SD, and 5 (62.5%) had PD on EGFR-TKIs (Table 3). In 47 patients with wild-type EGFR and KRAS (WT/WT), 5 (10.6%) had PR, 16 patients (34.0%) had SD, and 26 patients (55.3%) had PD on EGFR-TKIs. As a group, patients with KRAS mutations had a significantly poorer clinical response to EGFR-TKIs than those who had EGFR mutations (12.5% vs. 61.0%, p=0.004), but did not differ in clinical response from those with WT/WT (10.6% vs.12.5%, p=0.876).
At the time of analysis, the median follow-up duration of patients with advanced lung adenocarcinoma was 17.4 months. At the time of analysis, 103 (51.5%) of the 200 patients were still alive. In this survival outcome analysis, we excluded one patient who had both EGFR and KRAS mutations and who was treated with erlotinib/sorafenib because this dual inhibition of the EGFR and vascular endothelial growth factor (VEGF) pathways could influence survival outcome and cause a bias. Thus, the final analysis of survival outcome included 96 patients.
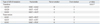
The three genotypes according to the presence of EGFR or KRAS mutation showed significant differences in median OS with EGFR-TKI treatment (26.7 months for the EGFR mutant, 8.2 months for WT/WT, and 9.2 months for the KRAS mutant, p=0.001) (Fig. 2A). In a Cox regression model adjusted for age, gender, smoking history and performance status, the AHRs for OS were 0.453 (95% CI, 0.260-0.787; p=0.005) for the EGFR mutant and 1.274 (95% CI, 0.571-2.842, p=0.554) for the KRAS mutant (Table 4).
The three genotypes differed significantly in median PFS (12.8 months for the EGFR mutant vs. 1.2 months for the KRAS mutant vs. 1.9 months for WT/WT, p<0.001). In a pair-wise comparison, the EGFR mutant showed a significantly longer median PFS than did the KRAS mutant or the WT/WT. The KRAS mutant and WT/WT did not differ significantly (p=0.588) (Fig. 2B). In a Cox regression model adjusted for age, gender, smoking history and performance status, the AHRs for the risk of disease progression with EGFR-TKI treatment was 0.246 (95% CI, 0.144-0.421; p<0.001) for the EGFR mutation and 1.278 (95% CI, 0.586-2.790; p=0.537) for the KRAS mutation (Table 4). These data identified the EGFR mutation as an independent positive predictive factor for treatment outcome with EGFR-TKIs and showed that the KRAS mutation did not predict treatment outcome with EGFR-TKIs. The outcome is totally driven by presence or absence of EGFR mutation.
DISCUSSION
To our best knowledge, this is the largest comprehensive analysis of the KRAS mutation and its association with smoking history performed to date in East Asian patients with lung adenocarcinomas. The main finding of our study was a lower incidence of the KRAS mutation in these tumors among our Korean study group compared to that reported for Western populations. Interestingly, cigarette smoking did not influence the frequency of KRAS mutation, but rather the type of KRAS mutation; and KRAS mutation did not independently predict outcome of EGFR-TKI therapy.
The low frequency of KRAS mutation in our study (8%, 16 of 200) is in good agreement with previous findings of KRAS mutation of less than 10% in East Asian patients with lung adenocarcinoma, compared with the recorded 30% or more among Caucasian patients.24,30-35 This difference might be explained by ethnic and environmental factors, in addition to reported differences in gender and smoking status distributions.34
The frequency of KRAS mutation did not differ according to smoking status in our study. In addition, the specific characteristics of smoking such as cumulative dose (pack-years), age at first exposure, and smoke-free years did not correlate with KRAS mutation frequency. A strong association between KRAS mutation and cigarette smoking has been established.22,23 However, careful scrutiny of these studies reveals that they included relatively small numbers of never-smokers and neglected to present detailed smoking histories. In a study of lung adenocarcinomas from almost 500 patients (17% never-smokers), Riely, et al.28 reported the presence of a KRAS mutation in 15% of tumors from never-smokers compared to 22% in the group overall, showing that smoking history does not clearly predict KRAS mutation status. In contrast, data from a recent meta-analysis show a significantly higher KRAS mutation frequency among current- or former smokers compared to that of never-smokers (26% vs. 6%, p<0.01).3 In our study, careful interpretation will be required because the lack of statistical significance might be caused by insufficient sample size. The association of KRAS mutation (i.e., presence of the mutation in the tumor) with smoking history, which includes cumulative smoking dose, age at first exposure, smoke-free years, and other factors, awaits further observation and analysis of large populations with detailed smoking histories.
Importantly, KRAS mutations observed in never-smokers are significantly more likely to be transition mutations than those in current- and former smokers, which is consistent with previous data.28 Similarly, transition mutations in TP53 are more common in never-smoker patients than transversions. This prevalence for transversions in TP53 may identify a molecular signature for the action of specific carcinogen(s) in cigarette smoke.28,36 Thus, the qualitative differences in KRAS mutations in lung tumors from never-smokers may be related to intrinsic tumorigenesis rather than to exposure to extrinsic carcinogens such as second-hand tobacco smoke.
The role of KRAS mutation in predicting survival with EGFR-TKIs treatment remains unclear.3,19 Although most studies show that a KRAS mutation predicts a poor response to EGFR-TKIs, these data do not strongly support an association between KRAS mutation and survival outcome because the reported treatment outcomes are not survival outcome such as OS or PFS, but response rate.3,11,13,15-17 Additionally, because EGFR and KRAS mutations are mutually exclusive, patients with KRAS mutations do not harbor EGFR mutations, whereas those with wild-type KRAS may potentially harbor EGFR mutations. Given the extreme sensitivity of EGFR mutant tumors to EGFR-TKIs, even a small proportion of patients with EGFR mutation in a cohort with KRAS wild-type tumors could confound or bias the association between mutation type and treatment outcome with EGFR-TKIs. To clarify the prognostic significance of KRAS mutation for these treatment outcomes, concurrent mutational analysis of EGFR and KRAS is mandatory.
To overcome these problems, we compared the PFS and OS of EGFR-TKIs treatment among three tumor groups, namely those with the EGFR mutant, the KRAS mutant, and WT/WT, with a concurrent analysis of EGFR and KRAS mutations. In particular, we compared the treatment outcomes between patients with KRAS-mutant and WT/WT tumors to detect clinically relevant differences in EGFR-TKI effectiveness. As expected, patients with the EGFR mutations showed significantly longer median OS and PFS than did those with KRAS-mutant and WT/WT tumors. However, those with KRAS-mutant and WT/WT tumors did not differ significantly in outcome even though there is a limitation by small number of KRAS mutation positive patients (n=8). This result is consistent with report by Jackman, et al.8 that the presence of the KRAS mutation should not be used as a predictive biomarker to exclude patients from EGFR-TKI treatment.
Although use of the KRAS genotype as a basis for treatment with EGFR-directed agents is controversial, it may be used to guide appropriate targeting of other treatments. Evidence suggests, for example, that dual inhibition of VEGF and EGFR pathways may overcome primary and acquired resistance to EGFR-TKIs.37 In vivo xenograft models, including some with KRAS mutations, show a stronger anti-tumor response to a dual blockade of VEGF/EGFR pathways, either by vandetanib or a combination of bevacizumab and erlotinib, than to erlotinib or gefitinib alone.37 In these models, EGFR-TKI resistance is associated with increased tumor- and host-derived VEGF.37 Thus, a VEGFR/EGFR dual blockade may plausibly be used to overcome EGFR-TKI resistance in NSCLC with the KRAS mutation.
In conclusion, this study found no differences in KRAS mutation frequencies among lung adenocarcinomas according to cigarette-smoking status, but did show qualitative differences, in that never-smokers were significantly more likely than current or former smokers to have transition mutations rather than transversions. Furthermore, even though testing for KRAS mutation in lung adenocarcinoma may have little use in the decision to treat with EGFR-TKIs, it may guide the targeting of individualized treatments, which might include a dual blockade of EGFR and VEGF pathways and use of RAF or MEK inhibitors.



 XML Download
XML Download