

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hypermagnesemia rarely accompanies acute symptoms.1 Severe symptomatic hypermagnesemia predominantly results from excess exogenous magnesium intake in patients with renal failure1 or in patients with bowel disorders.2 Although severe hypermagnesemia can be fatal, it is frequently overlooked. Here, we report a case of hypermagnesemia in a hemodialysis patient that aggravated constipation and resulted in colonic perforation.
CASE REPORT
A 62-year-old diabetic woman on chronic hemodialysis for 7 months was admitted to our hospital because of general weakness and constipation for 1 week. She was bed-ridden for 1 month because of a fracture of L3-L4 spine due to a pedestrian traffic accident. Her vital signs were within normal ranges, and she had no fever. Physical examination revealed soft but distended abdomen and hypoactive bowel sounds. Plain abdominal radiographs showed large bowel distension with stool impaction (Fig. 1). Laboratory data showed hemoglobin of 8.6 g/dL, hematocrit 25.8%, random glucose 258 mg/dL, blood urea nitrogen 24.8 mg/dL, serum creatinine 4.1 mg/dL, sodium 129 mEq/L, potassium 4.5 mEq/L, calcium 8.0 mg/dL, phosphorus 1.7 mg/dL, and C-reactive protein 48.1 mg/L. The serum magnesium level was 3.0 mg/dL, and was 2.2 mg/dL 1 week ago (normal range, 1.8-2.6 mg/dL). She had taken magnesium-containing laxative (magnesium hydroxide 1500 mg per day) for a month, which was prescribed by another clinic. Therefore, magnesium hydroxide was discontinued and other laxatives were given.
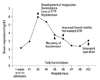
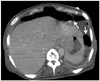
On the 3rd hospital day, the patient became lethargic and showed somnolence. Physical examination showed generally hypoactive deep tendon reflex, abdominal distension with no bowel sounds, and severe tenderness on the lower abdomen. Her vital signs were; blood pressure: 90/60 mm Hg, pulse rate: 90 beats/minute, and body temperature: 37.0℃. Electrocardiogram revealed normal sinus rhythm. The serum magnesium level was rapidly increased to 6.0 mg/dL. Plain abdominal radiographs showed more distended large bowel loops compared with those on admission. Computed tomography (CT) showed diffuse and marked dilatation of large bowel loops with fecal impaction, compatible with megacolon. The clinical course and the serum magnesium level are shown in Fig. 2. Calcium gluconate was infused for a temporary antagonizing effect of hypermagnesemia. Nasogastric tube and rectal tube were inserted for gastrointestinal decompression. Hemodialysis was performed daily for hypermagnesemia correction. After three consecutive hemodialyses, the serum magnesium decreased to 3.3 mg/dL and vital signs became normal. The patient started to have bowel movements, and abdominal distension subsided slightly with defecation. On the 11th hospital day, she complained of severe abdominal pain again. Diffuse abdominal tenderness and rebound tenderness were noticed. She was hypotensive (blood pressure 90/50 mm Hg) with a rapid pulse of 100/minute and febrile (37.5℃). The serum magnesium level was 3.1 mg/dL. Follow-up abdominal CT showed large air fluid levels in the upper pelvic cavity, representing gastrointestinal perforation (Fig. 3). Emergent Hartmann's operation was performed. Operative finding was necrosis of the transverse colon and rectum, and histologic findings were gangrenous colitis with microperforation and serosal abscess of the colon and rectum. After the operation, her abdominal pain was resolved and vital signs became normal.
DISCUSSION
Symptomatic hypermagnesemia is relatively rare because the proximal tubule and the ascending limb of the Henle's loop are highly effective in regulating magnesium levels. Even in the presence of decreased renal function, the serum magnesium level is regulated by a reduction in the gastrointestinal absorption of magnesium, which is in turn regulated by high serum magnesium levels.3 Therefore, hypermagnesemia is most frequently seen in conjunction with renal insufficiency and ingestion of magnesium-containing drugs or in patients with small bowel hypomotility disorder.3,4 Our case shows that hypermagnesemia is rapidly induced by magnesium-containing drugs and bowel hypomotility in a hemodialysis patient, and that it can result in colonic perforation despite the correction of hypermagnesemia.
Our patient had taken magnesium hydroxide for several months, but the serum magnesium level was within normal range prior to admission. On admission, she complained of aggravated constipation, and the serum magnesium level was 3.0 mg/dL. Despite the discontinuation of magnesium hydroxide, the plasma magnesium concentration was rapidly increased. We postulate that the immobility due to the late-onset lumbar fracture decreased the bowel motility and aggravated the constipation. Since the major gastrointestinal site for magnesium absorption is the upper small bowel5,6 and it occurs mainly through passive diffusion,2 bowel hypomotility may have resulted in a longer stay of magnesium-containing laxative in the intestine and the intestinal absorption of magnesium was enhanced. Hypermagnesemia can decrease bowel motility by blocking myenteric neurons and interfering with excitation-contraction coupling of smooth muscle cells.5 In addition, hypermagnesemia can block the peripheral and autonomic nervous system via antagonization of calcium effects, suppression of acetylcholine release, and reduction of postsynaptic membrane responsiveness, and depress the conduction system of the heart and sympathetic ganglia.7 Therefore, in this case, hypermagnesemia aggravated constipation and abruptly induced megacolon, hyporeflexia, somnolence, and hypotension.
Our patient developed somnolence and hypotension at a peak magnesium concentration of 6.0 mg/dL, which are usually seen when the magnesium concentration is above 7.2 mg/dL.8
Moreover, the paralytic effect of hypermagnesemia on the intestinal smooth muscle is rarely seen in clinical practice. A literature search of English-language journals was carried out using the National Library of Medicine PubMed on the internet, by employing the terms "hypermagnesemia", "ileus" or "perforation", and "case report". Four reports regarding hypermagnesemia-induced ileus or perforation were identified (Table 1).9-12 A comparison between our case and these cases showed that the peak serum magnesium concentration does not correlate with mortality or the severity of intestinal complication. Prolonged hypotension and a pressure effect of fecal impaction on intestinal circulation can induce intestinal ischemia. Since our patient had suffered from constipation with severe fecal impaction, she might have had impaired intestinal circulation, and the hypotension on the 3rd hospital day could have accelerated the ischemic colitis. Although bowel motility and cardiac compromise were gradually improved, colonic perforation developed due to prolonged ischemic colitis.
This case shows that hypermagnesemia manifests severe neurologic, cardiovascular, and intestinal complications in a hemodialysis patient. It is important to promptly correct hypermagnesemia, hypermagnesemia, since it can result in life-threatening events.


 XML Download
XML Download