

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The prevalence of type 2 diabetes (T2D) among Korean adults over 30 years of age has increased from 8.6% in 2001 to 9.7% in 2008,1,2 and the number of patients with T2D is predicted to reach about 300 million worldwide by 2025 with more than half from Asia.3 Cardiovascular diseases (CVDs) are a major cause of death among patients with T2D, and T2D is an important risk factor for CVD.4 Abnormal glucose-insulin homeostasis increases the likelihood of patients with T2D having impaired postprandial lipid metabolism, leading to conditions such as dyslipidemias with high levels of triglyceride and low levels of high-density lipoprotein (HDL)-cholesterol, which contribute to an increased risk of CVD.5,6
A healthy lifestyle that includes healthy eating is very important for preventing T2D and its complications including CVDs. Milk and dairy products, which are the best food sources of calcium, have been recommended for a healthy diet in diabetic patients. Recent studies have found that consuming milk and dairy products may reduce the risk of T2D.7-10 Tremblay and Gilbert9 reported that dairy products including calcium and vitamin D may play a significant role in reducing the risk of insulin resistance syndrome and T2D by regulating appetite, fat metabolism, and weight gain.10
Beneficial effects of consuming milk and dairy products on CVD-related mortality have been reported.11-13 The Coronary Artery Risk Development in Young Adults study, which was based on general community samples, found that dairy consumption had a strong inverse association with key risk factors for CVD including obesity, hypertension, and insulin resistance syndrome.14
However, most of the studies that have investigated the relationship between the intake of milk or dairy products and the risk factors for CVDs including lipid metabolism have been conducted in healthy populations.15,16 Few studies have evaluated the effect of milk and dairy products on lipid metabolism in patients with T2D, and there are few reports on the association between total dairy intake (not milk or fermented dairy products) and HDL metabolism.17,18 Moreover, most studies on the relationship between milk or calcium intake and lipid metabolism have involved Western populations with relatively high milk and calcium intakes,17,19,20 with few studies among populations who traditionally have a low consumption of dairy products. According to the Korea National Health and Nutrition Survey (2007-2009), Korean adults over the age of 19 years consumed 74.0±4.4 g (mean±SD) of milk and dairy products daily,2 which is markedly lower than populations in the United States (mean of 1.6 servings=156 g, 2003-2006 National Health and Nutrition Examination Survey),21 United Kingdom (259.6±180.1 g, Nutrition Diet and Nutrition Survey),22 France (205.2±160.5 g, INCA2),22 and Denmark (375.6±281.2 g, Danish Dietary Survey).22
This prospective study investigated the relationship between milk and calcium intake and lipid profiles among Korean female patients with T2D, who have a low intake of milk and dairy products and a higher risk of death caused by 627CVD than do male T2D patients.
MATERIALS AND METHODS
Study subjects
The participants were patients with type 2 diabetes who visited Huh's Diabetes Clinic in Seoul, Korea. Among the 1559 visitors to the clinic between 2005 and 2010, 1326 patients aged 35-80 years with a diagnosis of type 2 diabetes were selected and interviewed for the baseline investigation. Of that baseline sample, 647 female patients with type 2 diabetes were selected for further analysis. Of these, 138 subjects were excluded either due to insufficient or missing information, such as body mass index (BMI), dietary intake, blood glucose, and serum lipid profiles, or if they had an energy intake of <500 kcal/day or >4000 kcal/day. Therefore, 509 female patients with type 2 diabetes were eligible for this analysis. The subjects were classified into three groups (<50 g/day, 50-200 g/day and >200 g/day) based on their daily consumption of milk and dairy products: 0-<50 g/day, 50-200 g/day, and >200-1201 g/day. They were also stratified into two groups based on the estimated average requirements (EARs) of calcium intake: below and above the EAR. The research protocol was approved by the Institutional Review Board of Yonsei University Medical Center, and written informed consent to participate was obtained from all subjects.
General characteristics and dietary assessments
All of the female participants were interviewed individually at the first visit by nutrition graduate students to obtain data regarding their general characteristics, lifestyle behaviors, and food consumption. Food consumption for the previous year was assessed with a food frequency questionnaire (FFQ), which included 114 food items and has been validated elsewhere.23 Dietary intakes of nutrients and food groups were analyzed using CAN-pro 3.0 software (The Korean Nutrition Society, Seoul, Korea). The daily consumption of milk and dairy products was assessed by calculating the sum of the daily intake of whole milk, fat-modified milk, yogurt, ice cream, and cheese for each of the subjects.
Anthropometric parameters, blood pressure, and blood profiles
Standing height and body weight were measured using the In-body 4.0 system (Biospace, Seoul, Korea), with the subjects wearing light clothes and no shoes. BMI (kg/m2) was calculated and waist circumference was determined with a measuring tape (Tanita anthropometric tape, Seoul, Korea). Diastolic and systolic blood pressures were measured using an automatic blood-pressure monitor (Biospace, Seoul, Korea), with the subjects in a sitting position and after a 10-minute rest. Hypertension was defined as a systolic blood pressure of >120 mm Hg and a diastolic blood pressure of >80 mm Hg, or if the subject was taking hypertension medication.
Blood samples were drawn into EDTA-containing tubes after a minimum 12-hour overnight fast, and centrifuged at 1372×g for 20 minutes at 4℃ (Hanil Science Industrial, Seoul, Korea). Fasting serum levels of glucose were measured using a glucometer (Accutrendalpha, Boehringer, Mannheim, Germany), and hemoglobin A1c (HbA1c) was measured using an automated analyzer (HLD-723 G7, Tosoh, Tokyo, Japan). The rate of disappearance of plasma glucose was measured after an intravenous injection of regular insulin (0.1 U/kg), and the result of this insulin tolerance test (%/min) was used as an index of insulin resistance. Serum levels of total cholesterol, triglyceride, and HDL-cholesterol were determined with an autoanalyzer (Cobas Mira Roche Autoanalyzer, Hoffmann-La Roche, Basel, Switzerland). Low-density lipoprotein (LDL) cholesterol and the atherogenic index (AI) were calculated using the equations described by Friedewald, et al.24 and Lauer, et al.25 respectively. The C-peptide, insulin, apolipoprotein A-1 (Apo A-1) and apolipoprotein B (Apo B) levels were determined at the Seoul Medical Science Institute.
Statistical analysis
Data are expressed as means with SDs obtained through unadjusted analysis. Categorical values are represented by numbers and percentages. Variables with skewed distributions were log-transformed before analysis. Differences between three groups were evaluated using ANOVA, including the post hoc comparisons of Tukey, and differences between two groups were evaluated using t-test for unadjusted analyses with normal distribution variables. Food group intakes were investigated by nonparametric analysis such as Kruskal-Wallis or Wilcoxon-Mann-Whitney two-sample tests, as appropriate. Categorical variables were evaluated using the chi-square test to investigate differences between groups. After adjustment for age, BMI, total energy intake, exercise, and use of nutritional supplements and cholesterol medication, a general linear model was performed between groups. When statistically significant effects were demonstrated between three groups based on the relative consumptions of milk and dairy products, the Tukey post hoc test was used to identify group differences at p<0.05. The multicollinearity of adjusting variables was tested using coefficient or chi-square test, as appropriate. SAS 9.2 (SAS Institute, Cary, NC, USA) was used for all statistical analyses, and the level of statistical significance was set at p<0.05.
RESULTS
General characteristics, anthropometric parameters, blood glucose profiles, daily milk, and dairy products, and calcium intakes
The patients' general characteristics, anthropometric parameters, and blood glucose profiles are given relative to intakes of milk and dairy products in Table 1. The 509 middle-aged female patients with type 2 diabetes were aged 59.0±8.7 years (mean±SD). Patients with a milk/dairy products consumption of >200 g/day had significantly higher serum HbA1c concentrations than those consuming 50-200 g/day (p=0.0176).
Intakes of food and nutrients, and of daily milk, dairy products, and calcium
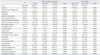
The daily food intakes of the female patients with type 2 diabetes, as assessed by an FFQ, are listed in Table 2. The average total daily intakes of food and animal and plant foods were 1348.3 g/day, 269.2 g/day, and 1079.0 g/day, respectively. Milk and dairy product intake according to calcium intake was 60.4 g/d and 178.0 g/d. Female patients with calcium intake above EAR showed significantly higher milk and dairy products consumption than the other group (p<0.0001). Most of daily food intakes showed significant differences among the three groups except meat and meat products, cereals and cereal products, beans and bean products and beverage. All of daily food intakes were significantly higher in female patients with calcium intake above EAR, except beverage, than the other group.
Daily nutrient intakes and density, and the percentage of energy intakes delivered from each of the three macronutrients are presented in Table 3. The mean total energy intake of the patients in this study was 1768.9 kcal. The total intakes of carbohydrate, protein, and fat were 263.9 g/day, 74.8 g/day, and 47.1 g/day, respectively. Calcium intake according to milk/dairy products consumption showed significantly positive association (p<0.0001), for each group, 493.3 mg/d, 654.4 mg/d and 952.0 mg/d, respectively. The data given in Table 3 indicate that the intakes of all of the nutrients were significantly higher in those patients with a milk/dairy products consumption of >200 g/day than in those consuming <50 g/day. Female patients with a milk/dairy products consumption of >200 g/day had a significantly lower percentage of energy intakes delivered from carbohydrate (p<0.0001) and a significantly higher percentage of energy intakes delivered from protein (p<0.0001) and fat (p<0.0001) than those consuming <50 g/day. Similar results were found in female patients with calcium intake above EAR.
Serum lipid and lipoprotein levels, and daily intakes of milk, dairy products, and calcium
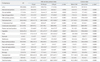
Table 4 lists the serum lipid and lipoprotein levels. The average serum level of HDL-cholesterol was significantly higher among the patients with a milk and dairy products consumption of >200 g/day than the other two groups (p<0.0001). Patients with milk and dairy products consumption of >200 g/day had a significantly higher Apo A-1 (p=0.0005) level and a significantly lower AI (p=0.0176) than those consuming <50 g/day or 50-200 g/day. Patients with a calcium intake above the EAR exhibited significantly higher serum HDL-cholesterol levels (p=0.0073) and significantly lower AI (p=0.0324) than the other EAR group.
DISCUSSION
We found that the consumption of milk and dairy products was positively associated with serum levels of HDL-cholesterol and Apo A-1, and negatively with the AI. This association appeared to be independent of other well-known risk factors, such as age, BMI, total energy intake, exercise, and use of nutritional supplements and cholesterol medication. Our findings are consistent with previous studies that found a positive association between the consumption of milk or dairy products and serum HDL-cholesterol levels in healthy subjects in Norway17 and Korea.16 However, we believe that ours is the first study showing that such an association also exists in patients with T2D. Our findings are significant when considering that the key atherogenic features of diabetic dyslipidemias are low levels of HDL-cholesterol with elevated serum triglycerides.5,26 Accordingly, our results that the serum HDL-cholesterol and Apo A-1 can be increased while the Apo B/A-1 ratio and AI can be decreased by the consumption of milk and dairy products have significant clinical implications for the development and implementation of nutritional therapeutic interventions for T2D.
Milk and dairy products contain many food components, among which calcium is the nutrient that has been related to HDL metabolism. Milk and dairy products are the best food source of calcium, and calcium supplementation has been shown to improve lipid metabolism in various experimental animals and humans.27 In our study the calcium intake-which was positively associated with the consumption of milk and dairy products-was positively related to serum HDL-cholesterol. These results suggest that consuming milk and dairy products (due to their calcium content) is protective against decreasing HDL levels in patients with T2D. Similar results have been reported previously specifically for the calcium intake.19,28,29 A daily calcium intake of 1200 mg achieved by supplementation increased serum levels of HDL-cholesterol in a Minneapolis (USA) crossover study of patients with hypercholesterolemia.28 A randomized-controlled trial involving postmenopausal women in New Zealand documented that increasing calcium intake by supplementation (1 g/day) increased serum HDL-cholesterol without elevating total serum cholesterol.29
Several mechanisms have been proposed for how calcium could benefit lipid profiles. Calcium can be bound to fatty acids and bile acids in the gut by bile salt hydrolase, thus interfering with lipid absorption.30-32 In addition to these intestinal effects, an HDL-cholesterol-increasing effect of calcium via a reduction in plasma cholesteryl ester transport protein (CETP) has also been suggested.27 Enhancing the calcium intake via milk consumption could increase serum HDL-cholesterol by decreasing CETP activity.
Another component in milk and dairy products that could increase serum levels of HDL-cholesterol and Apo A-1 is total and monounsaturated fat in milk.33 The total dairy fat intake was found to be positively correlated with serum HDL-cholesterol, Apo A-1, and the HDL/LDL ratio in a Swedish population, with these relations remaining after adjustment for dietary calcium. Although unsaturated fatty acids are minor components among more than 400 different fatty acids in milk and dairy products, monounsaturated fatty acids such as oleic acid can potently form larger postprandial chylomicrons.34
It has been reported that people consuming high-carbohydrate and low-fat diets of a lower quality are known to have low mean serum levels of HDL-cholesterol and Apo A-1.35,36 The traditional Korean diet is high in carbohydrate and low in fat, mainly consisting of rice and vegetables, with only small amounts of high-quality animal protein such as that found in milk and dairy products.37 Milk and dairy foods are good sources of high-quality animal proteins, vitamins, and other bioactive components,33 and contribute to improving the overall diet quality, which might also favorably influence lipid metabolism. In our study the nutrient densities for protein, minerals, and vitamins were significantly higher among subjects with the highest milk and dairy consumptions or with calcium intakes above the EAR. The daily consumption of milk and dairy products may be beneficial to patients with T2D with a low intake of high-quality proteins, especially in Asian regions, by lowering the risk of diabetic CVD complications by improving serum levels of HDL-cholesterol and Apo A-1, and the AI.
The hypolipidemic effects of milk and dairy products consumption and calcium intake in only female patients that we observed in the present study have also been confirmed by earlier reports, many of which were just more than anecdotal. Calcium supplementation showed biologically significant effects on serum lipids in postmenopausal women but not in middle-aged men, in a calcium intervention study with postmenopausal women and healthy men over 40 years old.19,38 The reason for a gender difference in response is not clear. Whereas testosterone clearly has effects on cholesterol metabolism, an interaction between the hormone and the use of calcium supplementation was unexpected.19,38 Further studies should be conducted to explore the different effects of calcium on serum lipid profiles by gender.
Our study appears to show that milk and dairy products as well as dietary calcium have positive associations with HDL-cholesterol metabolism only among women. Similar findings have been observed for Korean postmenopausal women: calcium supplementation has been shown to decrease LDL-cholesterol and increase HDL-cholesterol in postmenopausal women.29 It is notable and highly significant that milk and dairy consumption can alter lipid metabolism favorably among women, since it is well known that the risk of CVD is higher in postmenopausal women than in premenopausal women or in men. Moreover, the CVD death rates among Korean T2D patients are higher in women (35.3%) than in men (26.7%).39 Our results could lead to the development of dietary guidelines for diabetic patients, including milk and dairy products for the nutritional management of T2D, especially for many Asian female T2D patients who traditionally have a low consumption of milk and dairy products. Another noteworthy result from our present study was that those subjects in the group with a high consumption of dairy foods did not have high BMI, waist circumference, or serum total cholesterol or triglyceride, despite having a higher total energy intake and a higher energy intake from fat.
Our present results are inconsistent with those from Data from the Epidemiological Study on the Insulin Resistance Syndrome (DESIR) study which has declared that dairy product consumption was inversely associated with the incidence of impaired glucose tolerance.10 However, in the DESIR study, the classification of the lowest and highest dairy product consumption was <125 g/day and >250 g/day, respectively, which was much higher than that of our subjects of Korean patients with T2D.10 The differences between the two studies in milk consumption may induce the discrepancy in reporting the relationship between dairy products and serum glucose levels. Further studies which reflect differences in the ethnicity of the subjects and the quantity of milk consumed by them should be conducted to investigate the effects of milk and dairy product consumption on glucose metabolism.
Our present study was subject to several limitations that should be addressed in future studies. We observed an association between the intake of milk and dairy products and lipid profiles only in a cross-sectional setting. We were therefore unable to determine whether the intake of milk and dairy products is a cause or a consequence of dyslipidemias. The causal relationship should be evaluated in an intervention study involving newly diagnosed T2D patients without dyslipidemias. In addition, recall bias may have affected dietary intake assessed by an FFQ, although the use of a validated FFQ, a standard protocol, and well-trained interviewers would have minimized this type of bias. Our study did not examine the history of CVDs. This disadvantage is likely to be reduced through the adjustment for cholesterol medication. Further studies are needed to investigate in more detail the mechanisms by which calcium influences serum levels of HDL-cholesterol through decreasing lipid absorption.
In conclusion, our results suggest that the consumption of milk and dairy products is independently protective against dyslipidemias in Korean female patients with T2D. An adequate intake of milk and dairy products should therefore be recommended to Korean female patients with T2D to prevent dyslipidemias, which is strongly related to diabetic complications such as CVDs. Large-scale intervention and prospective studies are needed to evaluate whether increasing the intake of milk and dairy products reduces the risk of dyslipidemias in diabetic patients with a low consumption of milk and dairy products.


 XML Download
XML Download