

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cerebral palsy (CP) is the most common condition causing chronic serious physical disability in children. Specifically, spastic type is the most common form of CP and the upper limbs are commonly affected in these children. For over a decade, botulinum neurotoxin has been used to manage spastic upper limb in children with CP. With growing evidence favoring the neurotoxin injection for enhancing upper limb functions, a wide diversity of interventions have been tried in conjunction with the neurotoxin injection to improve spastic upper limb functions. For successful outcomes of such trials, the main prerequisite is to obtain extensive knowledge of upper limb dysfunction in these children.
As the term "spastic CP" has covered a wide range of clinical presentations and functional limitations, the gross motor and upper limb functions also vary between these children. Therefore, there is a growing need to evaluate both the gross motor and upper limb functions. The Gross Motor Function Classification System (GMFCS) is widely used to assess the gross motor function in children with CP, and the Manual Ability Classification System (MACS) was developed to evaluate a child's typical manual performance in daily life.1,2 GMFCS is now universally accepted as a valid and reliable means of classifying gross motor function in children with CP.3 However, MACS has recently gained attention as a valid and reliable classification system for upper extremity functions in children with CP aged 4 to 18 years.1,4 Previous studies revealed a significant relation between these two classifications in children with CP, but the relation was not always maintained in subtypes of CP.5-7 The discrepancy between GMFCS and MACS tends to be evident in children with hemiplegia. MACS reflects the performance of the International Classification of Functioning, Disabilities and Health, but not the maximal capacity. It also has not been designed to distinguish different capacities between two hands. It can be helpful to separately classify the best capacity of each hand for planning intervention. The Modified House Functional Classification (MHC) has been used mostly to evaluate the affected hand before and after surgery.8,9 This system provides a reliable way to classify each hand function and assess its best capacity.10,11 It has worked well in both the population based setting12 and in a clinical setting.10 Therefore, we think that MACS and MHC complement each other in assessing upper limb functions in children with CP and they seem to be associated with each other. However, the relations between both upper arm functional classifications have rarely been reported.
There are now several scoring systems for upper limb functions in children with CP,13 but no single system can fully assess the functional limitations of the upper limbs in children at different ages, varying severities and types of disabilities.12 Thus, clinicians must select the tools that meet the specific needs to evaluate upper limb functions. It is not always feasible to assess the upper limb function in many children with CP using the instruments requiring extensive time, equipment, or training. The Upper Extremity Rating Scale (UERS) and the Upper Limb Physician's Rating Scale (ULPRS) are simple tools that can be used by clinicians and health care providers for assessing upper limb functions. UERS was designed to measure range of motion, whereas ULPRS is a modified version of the Physician's Rating Scale,14 which assesses the movement quality of the upper limbs at three levels (palm, forearm, and elbow). Both range of motion and the quality of movement are key components in assessing upper limb functions in children with spastic CP. Thus, UERS and ULPRS are likely to be associated with functional classifications of the upper limbs. However, the relation between UERS and ULPRS with upper limb functional classifications like MACS and MHC has not yet been elucidated. Therefore, there is a need to describe the overall relation between various manual performance classification systems and upper limb functional measures and investigate the effective way to describe upper limb functions in CP.
Limitations in hand function are common in all types of CP, but the characteristics of the disability considerably vary between subtypes of CP.12 The best capacities of upper limb function can differ between two hands in the children with unilateral CP. Meanwhile, children with bilateral CP have a wide range of gross motor and upper limb functions, but the discrepancy in upper limb functions between two hands has not been evident. Therefore, it is assumed that the associations between gross motor function, manual ability and upper limb functional scales may be different in children with bilateral CP and unilateral CP.
The objectives of this study were to describe upper limb functions in children with spastic CP using various instruments that can be easily applied in a clinical setting and also to identify the relationships between gross motor, upper limb functional classification and upper limb functional measurements in children with spastic CP.
MATERIALS AND METHODS
Patients
We studied children who were over 4 years old and were admitted to our hospital for therapeutic intervention for spastic CP between June 2009 and February 2010. A total of 140 children were recruited for this study-105 children with bilateral CP (66 diplegia and 39 quadriplegia) and 35 with unilateral CP. The general characteristics of children with bilateral and unilateral CP are described in Table 1. This study was conducted with the approval of the Institutional Review Board (4-2009-0168), and written informed consent was obtained from all parents/caregivers before their children were enrolled in the study.
Methods
The GMFCS and MACS levels of patients were measured according to the manuals.1,15 The GMFCS levels were determined by a physician (ES Park) while MACS levels were determined by occupational therapists. House Functional Classification was developed for the evaluation of the function of a hand that had been surgically treated for thumb-in-palm deformity in children with spastic hemiplegia. The original House Functional Classification has 9 functional levels with a short description of each category.8 Koman, et al.10 developed a modified version of this system with additional descriptors for defining each category to clarify the assessment process. The modified version was preferred because its validity and reliability have been confirmed by a recent review and it may facilitate more consistent application in the clinical setting.10 Therefore, we used the modified version to classify upper limb functions. In the MHC, the original 9 levels of functions are consolidated into 4 levels (0 into non-functioning; 1 to 3 into passive assisting; 4 to 6 into active assisting; 7 and 8 into spontaneous use) and the inter-rater and intra-rater agreement were good to excellent in a previous study.11 In the present study, MHC was used to classify each hand function separately. In this study, the hand with better function was called the dominant hand, and the other the non-dominant hand. MHC of both dominant and non-dominant hands was determined by occupational therapists.
The scoring of ULPRS from videotape was done by physicians (JH Park and EG Sim).14 Each upper limb function was assessed separately with the highest possible score of 22. UERS of each hand was assessed by physicians (JH Park and EG Sim).10 Active range of motion of each segment was measured with children seated on an examination table or in their chair with back support using a goniometer.
Statistical analysis
The statistical analysis was done using SAS software (version 9.1.3, SAS Institute Inc., Cary, NC, USA). Non-weighted kappa statistics were used to measure the overall agreement between GMFCS and MACS. According to Altman, the kappa value is to be interpreted as follows: <0.20 as poor agreement, 0.21-0.40 as fair, 0.41-0.60 as moderate, 0.61-0.80 as good and >0.80 as very good agreement.5 The relationships of MACS with GMFCS, MHC, ULPRS and UERS were analyzed with Spearman's rank order correlation test. GMFCS and MACS were compared within bilateral and unilateral CP with Wilcoxon signed-rank test. The Kruskal-Wallis test was used to compare the differences between subtypes of spastic CP. Statistical significance was defined as a p-value less than 0.05.
RESULTS
MACS
The distribution of MACS levels in 140 spastic CP are shown in Table 2. Sixty-three (46.4%) children were independent in age-relevant manual activities (MACS I and II), and 10 (7.1%) children were totally dependent on others in their daily activities (MACS V). The MACS levels in children with hemiplegic and diplegic CP ranged between MACS I to IV, whereas no children with quadriplegic CP were classified as MACS I. Children with diplegic and hemiplegic CP showed significantly better MACS than children with quadriplegic CP (p<0.05).
GMFCS and MACS
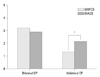
Almost half of the children (75 children, 53.5%) exhibited different levels of function on the GMFCS and MACS, and the overall agreement between the GMFCS and MACS was fair (kappa=0.31, p<0.01, weighted kappa=0.55). The Spearman's correlation coefficients between the GMFCS and MACS were r=0.60 for children with unilateral CP, r=0.72 for children with bilateral CP, and r=0.69 for all children (p<0.01). Children with unilateral CP scored higher on GMFCS than MACS (p<0.05) (Fig. 1). On the other hand, the difference between MACS and GMFCS was not significant in children with bilateral CP.
MHC
Hemiplegic and diplegic children showed better dominant hand function than quadriplegic children, but there was no significant difference between hemiplegic and diplegic children (Table 2). For non-dominant hands, diplegic children showed highest hand function, while quadriplegic children showed the poorest hand function.
The distribution of MHC levels of each hand is shown in children with bilateral and unilateral CP (Table 3). In 105 children with bilateral CP, 65 (61.9%) children used their dominant hand spontaneously and independently (MHC 7 or 8), and 34 (32.4%) children were evaluated as MHC 7 or 8 in their non-dominant hand. However, all 35 children with unilateral CP used their dominant hand spontaneously and independently (MHC 7 or 8), but only 5 (14.3%) of 35 children was evaluated as MHC 7 or 8 in their non-dominant hand.
MACS and MHC
In children with unilateral CP, MACS scores showed moderate association with MHC scores of non-dominant hand (r=-0.63) and dominant hand (r=-0.50). In children with bilateral CP, the relation between MACS and MHC was strong for both dominant (r=-0.87) and non-dominant hand (r=-0.83). The overall association is shown in Fig. 2.
Upper limb functional measures
ULPRS and UERS of each hand showed significant differences between CP subtypes (p<0.05). For the dominant hand, ULPRS and UERS in quadriplegia were significantly lower than that in hemiplegia and diplegia. For the non-dominant hand, the scores were significantly higher in diplegia than in quadriplegia and hemiplegia (Table 4).
MACS and upper limb functional measures
The ULPRS of the non-dominant hand were significantly related with MACS level in both bilateral CP (r=-0.75) and unilateral CP (r=-0.55). However, the relation between dominant hand ULPRS and MACS were significant only in bilateral CP (r=-0.66). In addition, UERS of the non-dominant hand was significantly related with MACS level in both bilateral CP (r=-0.71) and unilateral CP (r=-0.41). In the dominant hand, however, only bilateral CP showed a significant relation between UERS and MACS (r=-0.60).
MHC and upper limb functional measures
The ULPRS of the non-dominant hand was strongly related with MHC level in children with bilateral CP (r=0.90) and those with unilateral CP (r=0.89). However, ULPRS of the dominant hand was related with MHC level of children with bilateral CP (r=0.78) but not with unilateral CP. Similarly the UERS of the non-dominant hand was strongly related with MHC level in children with bilateral CP (r=0.85) as well as with unilateral CP (r=0.84). However, UERS of the dominant hand was related with MHC in bilateral CP (r=0.74) but not in unilateral CP.
DISCUSSION
To our knowledge, there are two population-based studies on upper limb functions in children with CP.5,12 One study described hand function in CP, while the other study investigated the association between gross motor function and manual abilities. However, these two studies derived from almost the same samples from the Cerebral Pares Uppfoljnings Program register for the counties of Skane and Blekinge in southern Sweden. Therefore, the distributions of GMFCS level and MACS level in children with spastic CP were almost the same for these two studies. In these studies, children with hemiplegic CP were distributed between MACS levels I and IV with the greatest number of subjects at MACS I. However, other previous studies revealed that the MACS levels in children with hemipelgia were distributed between MACS I and IV with the highest number of subjects at MACS II.6,12,16,17 There was a common denominator in that most children with hemiplegia were independent in manual abilities (MACS I and II), and no child was totally dependent on others (MACS V) according to previous studies. This is similar to our results.
For children with bilateral CP, some use the term "spastic diplegia" to describe spastic children who have motor involvement only in lower legs while others use this term for children who have arm involvement of lesser severity than leg involvement. However, determining the relative severity of arm and leg involvement can be challenging,18 and it is sometimes difficult to draw the boundaries for differentiating between diplegia and quadriplegia. Thus, it is recommended to use the term "bilateral CP" for both quadriplegia and diplegia in research papers and multicenter database of CP.19 Children with bilateral CP composed of diplegia or quadriplegia and were distributed between all levels of MACS in previous studies5-7,12,17 as well as in present study.
Even though gross motor function and manual performances in daily life are not equivalent entities in CP, a significant relationship between gross motor and manual activities in CP, measured by GMFCS and MACS, has been demonstrated.5,6 According to previous studies, the agreement between GMFCS and MACS were fair.5,6 The results of the present study are in line with those of previous studies. Previously, only one population based study investigated the correlation between GMFCS and MACS,6 in which the relation varied by subtype of spastic CP. The highest relation was found in spastic quadriplegia (r=0.76) and the lowest in spastic hemiplegia (r=0.29).6 The present study also revealed a relatively weak relation between GMFCS and MACS in children with unilateral CP compared with that in children with bilateral CP. Children with unilateral CP usually walk or try to walk, but sometimes cannot use the affected arm at all, leading to serious problems in bimanual hand function. Therefore, they often present better GMFCS levels than MACS levels. Our findings are in line with the result of the previous study.6 However, the strong correlation between MACS and GMFCS without significant differences in mean levels in children with bilateral CP suggests that the bimanual performance in children with bilateral CP correspond well with their gross motor function.
Children with spastic CP have hands with different capacities, and the difference was more evident in children with unilateral CP. MHC evaluates the 3 categories of hand function (reaching, grasping and manipulating objects) and represents the best capacity of each hand. In a previous study, MHC was recommended as a reliable tool to classify upper limb function in children with CP.3 In the present study, we identified a strong relation between MHC and MACS in children with bilateral CP. These findings suggest that bimanual performance was highly related with the best capacity of each hand in these children. Nevertheless, the relationship was not strong in children with unilateral CP in the present study. According to a previous study, a strong association (r=0.83) between unimanual capacity of the affected hand and bimanual performance was found in congenital hemiplegic CP.16 In that study, the Melbourne Assessment of Unilateral Upper Limb Function (Melbourne) was used to assess unimanual capacity whereas the Assisting Hand Assessment (AHA) was measured for bimanual performance. Although both AHA and MACS measure bimanual performance, AHA assesses the spontaneous use of the impaired upper limb in bimanual task, whereas MACS classifies the level based on the child's ability to handle objects and their need for assistance or adaptations to perform manual tasks in daily life. The differences in the relation between bimanual performance and unimanual capacity between the present study and Sakzewski, et al.'s16 study seem to have resulted from the distinct nature of the questions on these instruments used in the studies.
In a previous study, MHC was highly related with the Melbourne system (r=0.74), whereas the correlation between Melbourne and UERS was not strong (r=0.56 for the right hand, r=0.42 for left hand).10 Since UERS assesses range of motion measurements, a strong relation between UERS and Melbourne was not expected.10 The significant relation between UERS and MHC in both dominant and non-dominant hands of children with bilateral CP suggests that UERS can be a simple and useful tool to assess upper limb function in these children.
In children with unilateral CP, upper limb functional measures like ULPRS and UERS showed a relationship with MACS or MHC only in the non-dominant hand, whereas in children with bilateral CP showed a relationship for both the dominant and non-dominant hand. This suggests that upper limb function of unilateral CP should be described separately; not only with overall manual function classifications, but also with upper limb functional measures of each hand. Manual function classification alone could overestimate the non-dominant hand function of unilateral CP. However, upper limb function of bilateral CP could be described with overall manual function classifications as well.
Moreover, strong relations between ULPRS with MHC of each hand of children with bilateral CP and the involved arm of children with unilateral CP also suggest that ULPRS is a simple and useful tool for functional measurement of the upper limbs. The reliability and validity of ULPRS need to be examined for wide spread use of ULPRS.
Since this is not a multicenter study and limited to a single hospital, the results of this study should be considered carefully. Although recent publications on this subject offer results that are similar in many aspects to our study. We believe further multicenter prospective studies are needed.
In conclusion, most children with unilateral CP were independent in bimanual activities, while there was a large variation in bimanual performance and gross motor function in children with bilateral CP. Gross motor function, bimanual performance, and best capacity of each hand were closely related with each other in children with bilateral CP, while the three were often discrepant in children with unilateral CP. In clinical practice or research, upper limb functions in children with unilateral CP mightbe better described by using all three systems.





 XML Download
XML Download