

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Urinary tract infection (UTI) is the most common bacterial infection in infants and has been documented as an ascending infection of the patient's own fecal uropathogens, evidenced by genomic profiling study.1 Therefore, the role of lactobacillus, the most dominant urogenital microflora, has been a focus in preventing UTI.2,3
Intraurethrally instilled lactobacillus strains were proven to prevent experimental UTI in adult animal models,4-6 and clinical application of lactobacillus suppositories showed beneficial effects in reducing the recurrence rate of UTI in adult women.7-9 However, the preventive effect of oral lactobacillus probiotics against UTI has not sufficiently been investigated in adults.10,11
In early infancy when the UTI incidence is extremely high, postnatal development of genitourinary lactobacilli is considered very important in preventing UTI. It was confirmed that some maternal lactobacilli are transferred to their infants during birth and through breast milk.12-14 Probiotic lactobacilli, administered to lactating mother rats, were also proven to be transferred to their infant guts15,16 and then to genitourinary tract.17 However, a question of whether this mother to infant transmission prevents infantile UTI has not been clarified.
Therefore, we evaluated whether lactobacilli orally administered to pregnant and lactating mother rats could prevent experimental UTI of their infant rats, and compared the effects with those of intravesically instilled lactobacilli to infant rats.
MATERIALS AND METHODS
Materials
Lactobacillus mixture
For this study, we selected three lactobacillus strains (L. gasseri, L. rhamnosus, L. reuteri), which were isolated from the healthy infant feces and mixed. For optimal dosage, the lactobacillus mixture (LM) was incubated in the DeMan-Rogosa-Sharpe (MRS) agar medium to make six different dosages [106-1011 colony forming unit (CFU)/mL], which were tested for the antimicrobial activities against standard E. coli strain (ATCC No. 25922, Seattle, WA, USA). We selected the dosage 1010 CFU/mL, whose antimicrobial activity was maximal (Fig. 1).
The experimental infant rats
Forty-eight breast-fed Sprague Dawley infant rats (Seoul, Korea), whose mother rats were fed the LM (1 mL/day) via gavage tube from late pregnancy through lactation, were evenly allocated to the lactobacillus (LB) I (n=24) or II group (n=24). The control group included 20 infant rats, whose mother rats were given phosphate-buffer solution (PBS, 1 mL). All infant rats were breast-fed for 3 weeks, when the same LM (1 mL) was intravesically instilled to infant rats of the LB II group and PBS to those of the LB I and the control group. The study protocol was approved by the ethical committee of the hospital.
Urine and stool culture for lactobacillus
At age 3 weeks of infant rats, urines and stools were collected. Fecal specimens were placed to a 50 mL test tube together with sterile saline and shaken for 1 minute. For lactobacillus culture, urines and diluted fecal supernatants (200 µL) were inoculated into lactobacillus-selective MRS agar (Oxoid, Basingstroke, UK) and incubated anaerobically at 37℃ for 48 hours. Lactobacillus was confirmed by Gram-positive white, smooth bacillus, and colonies (CFU/mL) were counted.
Intravesical instillation of the lactobacillus mixture
After completion of stool and urine collection, the same LM (1 mL), given to the mother rats, was instilled into the bladder of infant rats of the LB II group using a 16-gauge silicone catheter after ketamine anesthesia. PBS (1 mL) was instilled into LB I and the control group.
Induction of experimental E. coli UTI
Twenty-four hours after intravesical instillation of the LM or PBS, 1 mL of standard E. coli strain (107 CFU/mL) was instilled into the bladder of infant rats to induce experimental E. coli UTI through a 16-gauge silicone catheter after ketamine anesthesia.
Histopathological examination
Seventy-two hours after intravesical instillation of E. coli, the infant rats were sacrificed for histopathologic examination. Both kidneys and bladder were extracted and fixed for 24 hours in 10% buffered formalin solution. The kidney was embedded in paraffin, sectioned 3 µm in thickness using a rotatory microtome, and Hematoxylin-Eosin staining and Masson-Trichrome staining were performed. According to the histopathological changes, cystitis and pyelonephritis were diagnosed and the incidence was compared. For semiquantative evaluation, the severity of inflammation in cystitis and pyelonephritis was scored. The cystitis score ranged from 0 to 3 (0 point without inflammatory cells, 1 point with a few inflammatory cells in the submucosa, 2 points with more than 5 focal inflammatory cells in the submucosa, and 3 points with diffuse inflammatory cells in the submucosa). The pyelonephritis score ranged from 0 to 4 (0 point without inflammation, 1 point with occasional inflammation in the pelvic mucosa, 2 points with continuous inflammation along the pelvic mucosa, 3 points with focal inflammation from the pelvic mucosa to the renal medulla, and 4 points with diffuse inflammation to the renal medulla).
Statistical methods
For statistical analysis, SPSS version 11.5 (SPSS Inc., Chicago, IL, USA) was used. ANOVA test was performed for comparison of the number of lactobacillus or E. coli, histopathological findings, the incidence and the score of cystitis and pyelonephritis between LB I, II and control groups. For the comparison of the number of lactobacillus and E. coli CFU/mL after experimental E. coli UTI, Wilcoxon signed rank test was used. p value less than 0.05 was determined to be statistically significant.
RESULTS
Lactobacillus colonization status in stools and urines of infant rats
The numbers of lactobacillus CFUs in the stools of infant rats were 3.5×108±6.6×107 CFU/mL in the LB I group, 4.1×108±2.5×108 CFU/mL in the LB II group, and 1.7×107± 7.3×106 CFU/mL in the control group (p>0.05). The numbers of lactobacillus CFUs in the urines of infant rats were 2930±314.4 CFU/mL in the LB I group, 5892±370.5 CFU/mL in the LB II group, and 1658±361.1 CFU/mL in the control group (p>0.05) (Fig. 2).
The incidence of experimental UTI
The incidence of cystitis was 95.5% (21/22) in the LB I group, 87.5% (21/24) in the LB II group, and 100% (20/20) in the control group (p>0.05). The incidence of pyelonephritis was 16.7% (4/24) in the LB II group, which was significantly lower than 75.0% (15/20) of the control group (p=0.015) (Table 1).
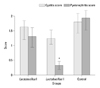
The semiquantitative inflammatory score of cystitis and pyelonephritis
The cystitis score of the LB II group (1.25±0.98) was lower than those of the LB I group (1.5±0.78) and control group (1.8±1.06) (p>0.05) (Fig. 3). The pyelonephritis score of the LB II group (0.33±0.68) was significantly lower than those of the LB I group (1.31±1.21) and control group (1.95±1.72) (p=0.006) (Fig. 3).
DISCUSSION
In preventing infantile UTI, postnatal development of genitourinary lactobacilli is considered very important. Indeed, lactobacilli in the maternal vagina are the first source of lactobacilli of newborn infants. While passing through the birth canal, maternal vaginal lactobacilli are transferred to the sterile neonate's gut for the first time.12 Lactobacilli in breast milk are the second important source of infant's gut lactobacilli.13 Approximately 6 days after birth, the number of CFU/mL of lactobacillus in the feces of breast-fed infants was 1000 times more than that of enterobacteriae, but 10 times less in the feces of bottle-fed infants.14 Probiotic lactobacilli, supplied during pregnant and lactating period, were proved to colonize the infant's gut.15,16 These vertically transmitted lactobacilli are transferred from gut to genitourinary tract.17
Many earlier studies demonstrated that the number of urogenital lactobacilli is significantly decreased in infants with UTI18 as well as in woman with urethritis and recurrent UTI.7-9,19-22 Antimicrobial activities of lactobacillus strains against uropathogens have been studied in many in vitro tests.23-26 Lactobacillus strains imped the adherence of uropathogens by secreting biosurfactants,23 compete with uropathogens in the binding site on vaginal epithelial cells,24 and inhibit the growth of uropathogens by secreting hydrogen peroxide, lactate, bacteriocin, and other antimicrobial molecules.25 They also enhance the local immunity of the intestinal mucosa, and improve the innate immunity and cell-mediated immunity by activating monocytes.26
The preventive effects of intravesically instilled lactobacilli against UTI have been proven in adult animal models with different strains and different dosages.4-6 When L. casei GR1 (5×109 CFU/mL), isolated from healthy adult women, was intravesically instilled to adult rats and was then swabbed twice weekly for 21 days onto the introitus before challenge with an uropathogen suspension (E. coli, K. pneumoniae, P. aerusinosa), experimental UTI was prevented in 84% of the animals.4 L. casei shirota strain (1×108 CFU/day), when administered intraurethrally to a mouse 24 hours prior to the induction of experimental E. coli, dramatically inhibited E. coli growth and inflammatory responses in the urinary tract.5 Furthermore, intraurethral instillation of the indigenous L. murinus strain (1×108 CFU/mL) also significantly prevented Proteus mirabilis ascending UTI in a mouse model.6
In the present study, intravesically instilled lactobacilli to infant rats showed the significant preventive effect against experimental pyelonephritis, whereas orally administered lactobacilli to pregnant and lactating mother rats did not prevent the infection of their infant rats. This might be due to insufficient increase of lactobacillus colonization in their stools and urines. Further studies are necessary to find ideal lactobacillus strains and an optimal oral dosage that are compatible with preventive effect of intravesically instilled lactobacillus.



 XML Download
XML Download