

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
About 150000 children and adolescents seek evaluation of a newly developed seizure disorder each year in the United States. And the incidence of epilepsy (recurrent unprovoked seizures) in this age group seems relatively consistent across all populations, ranging from 50 to 100/100000.1 Among these, 25% of patients continue to experience seizures despite receiving the best medical management availble, and may be defined as medically intractable. In these cases, if the seizures originate in a particular area of the brain and secondarily spread to involve other brain regions, a variety of surgical treatments may be beneficial, including focal cortical resection, corpus callosotomy, functional hemispherectomy, and multiple subpial resections.2
In order for an epilepsy surgery to be successful, one must not only localize the epileptogenic lesion, but also determine the anatomic localization of the eloquent cortex and functional white matter tracts in the brain in order to spare these areas during any planned cortical excision of the epileptogenic cortex.2 Accordingly, conventional structural imaging, magnetic resonance spectroscopy, and other advanced MR imaging techniques are widely used in epilepsy surgery; however, they cannot detect all causes of pediatric epilepsy.3
Diffusion tensor tractography (DTT) enables the graphical reconstruction of the white matter pathways in the brain and spinal cord of living humans. This technique has many potential clinical applications, including the investigation of stroke, multiple sclerosis, epilepsy, neurodegenerative diseases, and spinal cord disorders.4 There are even reports of its use in the alternation of DTT in cortical dysplasia and tumors.5-7 However, there has been limited study in regards to the usefulness of DTT in pediatric epilepsy surgery in the literature. In this study, we aimed to assess the clinical relevance of DTT in pre- and post-operative evaluations of childhood epilepsy according to types of surgeries performed.
MATERIALS AND METHODS
Patients
This retrospective study was approved by the Institutional Review Board and informed consent was waived. Between March 2004 and July 2008, 203 pediatric patients underwent epilepsy surgery at our hospital. Among these, seventy two patients underwent MR imaging study including DTT within 6 months before and/or one week after the operation, comprising 40 males and 32 females with a mean age of 8.9 years (from 3 month to 24 years). The subjects had experienced a variety of seizures including complex partial seizures (n=26, 36.1%), generalized tonic-clonic seizures (n=17, 23.6%), absence seizures (n=13, 18.1%), simple partial seizures (n=9, 12.5%), infantile spasm (n=5, 6.9%) and atonic seizure (n=2, 2.7%) for a mean seizure duration of 4.9 years (range from one month to 20 years).
Imaging protocol
MRI was performed using a 3.0T scanner (Achieva, Philips Medical Systems, Best, the Netherlands) with an eight-channel sensitivity encoding (SENSE) head coil. Routine epilepsy imaging protocol included anatomical sagittal T1, axial T2 with thin section (3 mm thickness), axial fluid-attenuated inversion recovery (FLAIR) with 5 mm thickness, oblique coronal T2 and FLAIR for hippocampal evaluation, and 3-dimensional T1 weighted gradient echo coronal images reconstructed to 1 mm thickness.
DTT was performed as a routine protocol for in-patients scheduled to undergo epilepsy surgery and out-patients diagnosed with a definite lesion near the functional eloquent areas on MRI at other hospitals. DTT parameters were as follows: single-shot spin-echo echo-planar imaging with SENSE factor 2, 128 matrix with 22 cm field of view, 1.75 mm thickness, i.e. 1.75 mm3 isovoxel, echo time=60 ms; repetition time=9480 ms; number of sample averages=2, b=600 s/mm2, in 32-different diffusion gradient directions. All images were obtained perpendicular to the anterior and posterior commissural line (AC-PC line). The data were processed on a PC equipped with Philips Research Image-processing Development Environment software (Philips Medical Systems, Best, the Netherlands), based on the Fiber Assignment by Continuous Tracking (FACT) method.8
Anisotropy was calculated using orientation-independent fractional anisotropy (FA), and diffusion-tensor MR imaging-based color maps were created from the FA values and the three vector elements. Vector maps were assigned to red (x element, left-right), green (y, anterior-posterior), and blue (z, superior-inferior) with a proportional intensity scale according to the FA. Three-dimensional DTT was then achieved by connecting the voxel to voxel with the FACT algorithm. The threshold values for the termination of the fiber tracking were less than 0.2 for FA and greater than 45° for the trajectory angles between the ellipsoids. Major white matter tracts such as the corticospinal tract, optic radiation, and arcuate fasciculus were explored using multiple regions of interest methods.
Review of the relevance of DTT
We reviewed data focusing on types of surgery, lesion location, final pathological diagnosis, and how the DTT data were clinically used. Types of surgery were divided into three groups: 1) complete resection of the epileptogenic lesion (cortisectomy or lobectomy), 2) corpus callosotomy, and 3) functional hemispherectomy.
In considering DTT evaluation, only the preoperative MRI was evaluated in cases with lesional resection, focusing on the lesion localization and the relationship between the lesion and major white matter tracts including the corticospinal tract, optic radiation, and arcuate fasciculus. In cases of corpus callosotomy or functional hemispherectomy, both pre- and post-operative MRI was evaluated focusing on the proper or complete resection.
Postoperative neurologic complications or seizure outcomes were also analyzed according to the surgery type based on the medial record.
RESULTS
Types of surgery and pathological diagnosis
In regards to surgery types, 52 patients underwent complete resection of epileptogenic lesions, 18 patients underwent corpus callosotomy, and only two patients underwent functional hemispherectomy.
On the analysis of the pathological diagnoses of the 52 patients with lesional resection, cortical dysplasia (n=32, 44.4%) was the most commonly observed, followed by hippocampal sclerosis (n=9, 12.5%) and brain tumors (n=7, 9.7%). In the brain tumors, the final diagnosis was dysembryoplastic neuroepithelial tumor (DNET) in four patients and ganglioglioma in three patients. The remaining four cases (5.6%) showed normal brain tissue on pathology.
Preoperative DTT analysis
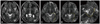
Preoperative DTT was used for evaluating the relationship between the lesion and major white matter tract in 52 patients who underwent lesional resection. The lesion location and related major white matter tracts are summarized in Table 1. There was an approximal relationship between the lesion and major white matter tract in 21 patients among 32 cortical dysplasia cases: corticospinal tract in 15 cases, arcuate fasciculus in four cases, and optic radiation in two cases (29.2% of all epilepsy surgeries). Identification of the corticospinal tract and evaluation of the relationship between this tract and primary mass was informative in three cases of frontoparietal tumors (Fig. 1). In one case of frontotemporal tumor, the relationship between the lesion and arcuate fasciculus was useful in pre-surgical planning (Fig. 2). DTT also showed a relationship between optic radiation and occipital lesion (Fig. 3). However, DTT was not clinically utilized in cases of hippocampal sclerosis.
Pre- and post-operative DTT
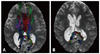
Pre- and post-operative DTT was evaluated in 20 patients with corpus callosotomy or functional hemispherectomy. Among the patients who underwent corpus callosotomy (n=18), there were no remarkable lesions on brain MR in eight patients, diffuse brain atrophy in six patients, cortical dysplasia in three patients and hippocampal sclerosis in one patient. Post-operative tractography was used for the evaluation of complete resection in these patients (Figs. 4 and 5).
Functional hemispherectomy was performed in two cases, hypoxic ischemic encephalopathy in one case and Sturge-Weber syndrome in the other. These patients did show improvement in seizures after surgery; however, DTT was not utilized for the evaluation of major white matter tract or complete resection.
Postoperative complications and seizure outcomes
There were two complicated cases. One patient with cortical dysplasia was dead immediately after lesional resection due to cardiac arrest. The other case underwent emergency reoperation after corpus callosotomy because of incomplete resection on post-operative DTT (Fig. 5). There were no other complications such as visual field defect or weakness after the operation.
Postoperative seizure outcome was free in 53 patients (53/72, 74%), improved in 12 patients (12/72, 17%), and continued in 6 patients (6/72, 8%). Lesional resection showed worse outcomes (41 seizure-free, 5 improved, 5 continued, and 1 dead) than corpus callosotomy (11 seizure-free, 6 improved, and 1 continued) or functional hemispherectomy (1 seizure-free and 1 improved). However, all cases of lesional resection due to tumor or hippocampal sclerosis showed postoperative seizure-free status.
DISCUSSION
Since the late 1990's, diffusion tensor technology has been utilized to visualize human white matter tract in vivo, as a routine clinical procedure for contemporary neuroimaging. DTT was found to be effective in neuro-oncology, neurodegenerative disease, and stroke imaging, but its clinical relevance in epilepsy surgery has still not been established. Although this study was not a well designed prospective study, we insist that the results of this review could be proof of the clinical usefulness of DTT in daily neuroimaging of epilepsy patients.
Diffusion tensor imaging captures anisotropic diffusion of water to delineate microstructural tissue organization. In brain imaging, the diffusion of water in white matter is greater in directions parallel to fiber tracts, allowing for axonal fiber delineation. In DTT, voxels are color coded according to the most prominent direction of water diffusivity in the axial, sagittal, or coronal plane. Conventionally, red is used for tracts in the left-to-right direction, green for the anterior-to-posterior direction, and blue for the superior-to-inferior direction. Three-dimensional image formation is also possible.9
Cortical dysplasia is one of the most common epileptogenic substrates responsible for intractable epilepsy in children, with a nearly 80% incidence in children younger than 3 years of age.10,11 Circumscribed lesionectomy of focal dysplastic lesions provides seizure relief in medically intractable patients with temporal and extratemporal epilepsy.12 Accordingly, precise lesion localization on presurgical imaging is important in these patients. Decreased anisotropy of white matter adjacent to the malformed cortex and an aberrant course of major fiber pathways due to dysplastic white matter are common findings in cortical dysplasia. And DTT can identify these microstructural changes based on elevated mean diffusivity and reduced anisotropy in the subcortical white matter of MR imaging-visible cortical dysplasia.5,6,11 In our study, 21 of 32 patients with cortical dysplasia had approximal proximity with major white matter tracts, i.e. located along the course of the corticospinal tract, dominant hemispheric deep white matter, etc. DTT clearly depicted a spatial relationship between the lesion and white matter tract and preoperative information aided neurosurgeons in avoiding injury during lesion resection.
Neoplasms of the central nervous system in pediatric patients often manifest clinically as seizures, and these are the second most common causes of epilepsy in pediatric patients.13 These tumors include ganglioglioma, gangliocytoma, desmoplastic infantile ganglioglioma, DNET, and pleomorphic xanthoastrocytoma.14 Our study also included cases of DNET and ganglioglioma. In regards to performing DTT in these patients, Yu, et al.7 showed that DTT allowed for visualization of the exact location of tumors relevant to eloquent tracts and was found to be beneficial in neurosurgical planning and postoperative assessment. Our study also showed the usefulness of DTT in four out of seven patients.
Hippocampal sclerosis is rare in pediatric patients.13 On DTT, diffusion anisotropy may reveal abnormalities in mesial temporal lobe epilepsy in adult patients.15,16 However, in children with a shorter duration of epilepsy, such changes may have not yet emerged.17 Our study also showed no change in DTT for patients with hippocampal sclerosis. A recent study showed that Meyer's loop of the optic radiation could be damaged after anterior temporal lobectomy and that the heterogenous anterior extent of Meyer's loop could be evaluated with DTT.18 However, there was no significant anterior extent of Meyer's loop in our patients and no visual field deficits were observed after operation. We deduced that DTT is not useful in pediatric patients with hippocampal sclerosis.
Corpus callosotomy, while not curative, may reduce the rapid generalization of discharges from the ictal onset zone and prevent harmful drop attacks from occurring, finally improving the quality of life for children.19,20 DTT and fiber tractography can reveal the hemispheric fiber connections of the corpus callosum.5 Accordingly, we applied DTT in pre- and post-surgical evaluation of corpus callosotomy, and the fiber connections were well-demonstrated in all cases, including the one case of incomplete resection. Therefore, we discerned that DTT is a useful sequence in the MR imaging evaluation of patients with corpus callosotomy for both before and after surgery.
In cases with functional hemispherectomy, lesions showed a loss of white matter tract on pre-operative study and DTT was not utilized for the evaluation of major white matter tract or complete resection on both pre- and post-operative imaging.
There are some limitations of our study. Firstly, DTT was not performed in all patients who underwent pediatric epilepsy surgery. DTT was not performed in the emergency unit. And if there was a tumor in some epilepsy patients, tumor protocol was performed without DTT. If DTT was not performed within 6 months before and/or one week after operation, these data were excluded. Additionally, as children grow, brain lesion can change during follow up. Therefore, we felt that performing imaging studies more than 6 months before operation is too long. We also thought that early postoperative DTT could be more accurate in evaluating complete resection. However, there may be selection bias. Secondly, we included not only pediatric patients, but also young adult patients (who were older than 18 years old, n=6). However, these patients suffered from epilepsy for a long duration, since childhood (duration range 10-20 years, mean 13.7 years). Moreover, the final diagnoses of these patients were cortical dysplasia in three patients, hippocampal sclerosis in two, and normal brain tissue in one. Therefore, we believe that these inclusions are appropriate. Thirdly, we did not evaluate DTT quantitatively. We only evaluated the relationship of the major white matter tracts and epileptogenic lesions, but did not measure the fiber volume or fractional anisotropy. Quantitative image analysis could provide more objective information and suggest a guideline for tissue characterization and surgical strategy. Accordingly, further study is needed to address this point.
Neuroimaging study in pediatric epilepsy surgery should be multimodal, and DTT is a useful technique for the evaluation of epilepsy surgery. DTT was shown to be more helpful in cases of focal epilepsy caused by cortical dysplasia and low grade brain tumors. Pre- and post-operative tractography was also shown to be useful in callosotomy procedure. In conclusion, DTT is a suitable routine pulse sequence for performing proper epilepsy surgery in children.




 XML Download
XML Download