

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In 1996, Majeed, et al.1 reported that laparoscopic cholecystectomy takes longer to perform than small-incision cholecystectomy and does not have any significant advantages in terms of hospital stay or postoperative recovery. However, it has been widely accepted that laparoscopic cholecystectomy is more advantageous for patients than open cholecystectomy for treating benign gall bladder (GB) diseases. Since laparoscopic cholecystectomy has become the standard method for treating benign gallbladder diseases, various technical methods have been introduced to reduce the number of trocars and surgical wounds, and efforts to minimize the invasiveness of the surgical procedure remain the foundation for surgical improvements, offering clinical advantages to patients.
Accordingly, we also previously introduced a variant type of single incision and multi-port laparoscopic cholecystectomy technique, called single-fulcrum laparoscopic cholecystectomy (SFLC),2 and suggested the technical feasibility of SFLC. The SFLC-technique eliminated the need for expensive and specially designed ports for single port surgery. Other articulating laparoscopic instruments were not necessary either. Therefore, it was easy to set-up and resulted in low cost surgery with similar cosmetic results to usual single port surgery. Now, this technique has become an alternative standard procedure for most elective laparoscopic cholecystectomies performed by our team. With knowledge of basic principles and concepts, it is thought that this technique can be easily performed by other surgeons with a short learning curve period.
In this study, we compared perioperative clinical outcomes of SFLC with those of conventional laparoscopic cholecystectomy (CLC) in treating uncomplicated benign GB disease, and again, tried to suggest the technical feasibility, safety and effectiveness of SFLC in selected gallbladder disease.
MATERIALS AND METHODS
Between March 2009 and December 2010, SFLC was performed in 130 patients by one surgeon. Among them, 105 patients with uncomplicated gallbladder disease were selected in this study. We defined uncomplicated gallbladder disease as an asymptomatic GB stone, GB polyp, and GB adenomyomatosis without inflammation. Additionally, another 105 patients with uncomplicated gallbladder disease who underwent CLC during the same period were also selected for comparative analysis. Perioperative outcomes, such as operative time, length of hospital stay after operation, blood loss, and complications were reviewed. Pain was evaluated using the visual analogue scale (VAS) at the time of immediate postoperative period and discharge day. This study was approved by the institutional review board of Yonsei University Health System.
Working mechanism of single fulcrum laparoscopic cholecystectomy
The surgical concept and technique of SFLC were well demonstrated in a recently published manuscript.2 The reason for using the term "single fulcrum" is that two working ports, a 2 mm (Autosuture-Tyco, Norwalk, CT, USA) and a 5 mm trocar (Meditech Inframed, Paju, Korea) (Fig. 1), are placed in an X-shape through a single fulcrum, able to change their acting direction whenever the dissection field changes. When the anterior aspect of the Calot's triangle is dissected, the 2 mm grasper holding the infundibulum in the right hand can be directed toward the patient's right side and dissection with a 5 mm dissector or hook coagulator in the left hand can be performed. When the posterior aspect of Calot's triangle is dissected, the 2 mm grasper holding the infundibulum in the left hand can be moved to the patient's left side to expose the posterior aspect. Dissection of the posterior aspect of Calot's triangle is then performed with a 5 mm dissector or hook coagulator placed in the right hand.2 Complete dissection of Calot's triangle and exposure of the cystic duct and artery can be made by changing the action direction of the 2 mm and 5 mm instruments throughout the single fulcrum (Fig. 2).
Surgical procedures
In brief, SFLC was performed via a conventional trocar, not a specialized one-port system. A single skin incision was made in a similar fashion as with a transumbilical vertical incision of about 2 cm to expose the fascia. A 10 mm trocar (Meditech Inframed, Paju, Korea) for the camera was inserted at the 12 o'clock position from the center of the incision. Once pneumoperitoneum was obtained, a 10 mm-30° straight video laparoscope was introduced through the 10 mm trocar and used to inspect the peritoneal cavity to discern the feasibility of performing this technique. If there was no inflammation or anatomical variation, additional 2 mm and 5 mm trocars were inserted at 6 o'clock from the center of the incision with a single fulcrum site as far as possible from the 10-mm trocar to preventing crowding of the laparoscope and working instruments. A 2 mm grasper and conventional straight 5 mm instruments (dissector, hook coagulator, laparoscopic scissor and clip) were used. The operator stood on the left side of the patient handling two working instruments and a camera assistant stood in front of the operator to control the laparoscope. For proper exposure of Calot's triangle, a 2-0 nylon suture, which was inserted into the right intercostal space at the mid-clavicular line and held by a second assistant, was applied to the gallbladder plate of the proximal fundus for upward traction of the gallbladder. Two instruments (2 mm grasper and 5 mm instruments) were positioned so that they crossed each other through the fascia layer, creating an X; this crossing of the two working instruments is the main principle of single fulcrum laparoscopic cholecystectomy. The center of the "X" is the fascia layer through which the 2 mm and 5 mm trocars were inserted, and the center of the X we deemed a "single-fulcrum". With right lateral traction of the infundibulum by a 2 mm grasper in the right hand, the anterior aspect of Calot's triangle was exposed and dissected by a 5 mm dissector and hook coagulator in the left hand. After finishing the dissection of the anterior aspect, the posterior aspect of Calot's triangle was dissected by 5 mm instruments using the right hand, maintaining left traction of the infundibulum with the 2 mm grasper in the left hand. The cystic duct and cystic artery were then meticulously isolated, clipped and divided, changing instruments through the 5 mm working trocar. The gallbladder was dissected free in a bottom-to-top fashion. Before completing the gallbladder dissection, the operative field was rechecked lifting the liver bed up via a nylon suture. The specimen was retrieved using an endo-pouch, and the fascial defect and skin was closed.
The operation time was recorded according to two definitions. The total operation time was defined as the time from skin incision to skin approximation. The actual operation time was measured from the start of dissection of gallbladder after trocar insertion to retrieval of the specimen. The conventional laparoscopic cholecystectomy was performed in usual manner with the four trocar method (12 mm trocar ×1 and 5 mm trocar ×3).
Statistics
Categorical variables are expressed as frequency with percentage and continuous variables are expressed as mean values±standard deviation. The chi-square test for categorical variables and Student's t-test for continuous variables were used to evaluate statistical significance between parameters. Statistical significance was set at a p-value of less than 0.05. The learning curve was statistically fitted to the power-law curve (y=a1x-a2), and analyzed by the linear regression method.3
RESULTS
Preoperative patient characteristics (SFLC vs. CLC)
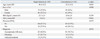
SFLC was more frequently performed in young female patients (46.4±12.2 years vs. 52.5±13.6 years, p=0.001), (76.2% vs. 59%, p=0.008), and ASA score for SFLC was lower than that for CLC (1.0±0.2 vs. 1.3±0.5, p<0.001). However, GB pathology, BMI, and history of previous abdominal surgery were similar between each group (p>0.05) (Table 1).
Operative and postoperative outcomes (SFLC vs. CLC)
There were no open conversion cases. The total operation time was longer in SFLC (56.7±14.1 min vs. 47.5±17.1 min, p<0.001); however, the incidence of drain insertion was limited in SFLC (null vs. 12 out of 105, p<0.001). In addition, pain scores immediately after operation and at discharge were lower for SFLC than for CLC (3.1±1.3 vs. 4.0±1.9, p<0.001, 2.0±0.9 vs. 2.4±0.8, p=0.002). However, there was no difference in analgesic requirement. All patients took a meal immediately after surgery with routine oral medicine including oral analgesics and digestive drugs. Few patients required intravenous or intramuscular analgesics due to unresolved pain. Total cost was lower for SFLC than for CLC (US $ 1801±289.9 vs. US $ 2003±617.4, p=0.004). There were no differences in intraoperative bile spillage (gallbladder wall perforation during dissection of gallbladder from liver bed using hook coagulator device), blood loss, complication rates, and hospital stay (p>0.05) (Table 2).
Change of operation time in SFLC
As experience was accumulated, the total operation time and actual operation time in SFLC gradually decreased (Fig. 3). The mean actual operation time was 21±8.5 min. The gray diagram depicts the total operative time (skin-to-skin) and the black diagram shows the actual cholecystectomy time (from starting dissection to detaching gallbladder from liver bed). The continuous line expressed the estimated learning curve. The estimated learning curve was fitted and defined as y=90.31x-0.13, with R (range)2=0.261. The dotted-line shows the moving average for every 10 cases of total operation time. The two graphs revealed a decreasing operation time as experience with the procedure was accumulated.
DISCUSSION
Single incision laparoscopic cholecystectomy (SILC) may refer to one of two methods. One comprises a single incision using the single port method and the other involves a single incision using the multi-port technique. SILC requires many specialized instruments, such as an articulating grasper or dissector, flexible endoscope, a specialized port, a surgical glove port,4,5 or commercial products.6 Even though a surgical glove port is feasible in SILC, a wound retractor is needed to fix the glove to the abdomen; moreover, special efforts to insert conventional ports into the glove are needed. Commercial single ports are also available. However, commercial single ports are more expensive than conventional ports. The present SFLC method uses only conventional ports without the need for specialized instruments. If other ports are needed for conversion to conventional laparoscopic cholecystectomy in difficult cases, the working 5 mm and 2 mm ports can be inserted into the upper mid abdomen and right subcostal area as in the conventional method.
To overcome limitations with the instrument's acting angle, several authors have come up with a SILC technique using articulating instruments4,7,8 or flexible endoscopes.8-10 If the concept of the "single fulcrum" described in this study is understood, articulating instruments and flexible endoscope may not be mandatory. To achieve safety in laparoscopic cholecystectomy, proper exposure of both the posterior and anterior aspects of Calot's triangle are very important. SFLC is able to achieve proper visualization of Calot's triangle using the following technique: when dissecting the anterior aspect of Calot's triangle, the straight 2 mm grasper holding the infundibulum is directed toward the patient's right side and dissection is performed with a straight 5 mm dissector or hook instrument. To dissect the posterior aspect of Calot's triangle, a 2 mm grasper holding the infundibulum is moved to the patient's left side so that the posterior aspect can be fully exposed. Dissection of the posterior aspect can then be performed with a 5 mm dissector or hook instrument.
Another point of emphasis in regards to the safety of a procedure performed via a single incision is proper traction of the GB. For the purpose of GB traction and exposure of the Calot's triangle, some authors have introduced extracorporeal sutures11 and the use of Endograb.12 In this study, we used an extracorporeal suture. A 2-0 nylon suture was applied to the GB plate of the proximal fundus (without penetration of the GB to avoid intraoperative iatrogenic bile spillage from needle insertion), which was inserted into the right intercostal space at the mid-clavicular line and held by the second assistant (Fig. 2).
SILC leaves a smaller wound than conventional laparoscopic cholecystectomy. Therefore, we can expect less pain in SILC than in CLC. Some authors reported lower pain scores in SILC,13-16 but others revealed similar scores.17 This study evaluated postoperative pain using the VAS immediately post-operation and upon discharge from the hospital. VAS pain scores immediately post-operation and on the day of discharge were lower in SFLC than in CLC (3.1 vs. 4.0, and 2.0 vs. 2.4, p<0.05, respectively). However, the difference in pain score seemed so minimal that clinical significance needs to be translated carefully.
Single incision and multi-port methods have usually been performed with conventional ports.18,19 When we use conventional ports, instrumental crowding among the heads of ports located in the extracorporeal area is a major problem, interfering with movement of the ports. For this reason, a 2 mm port and 5 mm port with a thin head (Meditech Inframed, Paju, Korea) (Fig. 1) are used in the current technique of SFLC. If the head portion of the typical camera port could be minimized like current 5-mm ports, this surgical procedure would be easier due to greater extracorporeal working space.
Love, et al.20 reported the cost differences between SILC and CLC. Their study showed no significant difference between the costs of SILC and traditional LC when standard materials were used. In this study, the total cost was cheaper for SFLC (US $ 1801 vs. US $ 1999, p=0.004) than CLC (Table 2). The number of ports used in SFLC was one less than in CLC (three vs. four). We also did not use specialized ports or articulating instruments. Lower pain score meant less need of pain killers. These factors may have reduced the total cost of SFLC.
The majority of studies comparing surgical results between SILC and CLC have shown SILC to be feasible.17,21-23 In this study, there were no differences between the two procedures in terms of bile spillage during operation, blood loss, complication rates, and hospital stay (Table 2). However, total operation time was significantly longer in SFLC (56.7 min vs. 47.5 min, p<0.001). Compared to other studies, 56.7 minutes in SILC is thought to be acceptable.21-25 In addition, operation time gradually decreased as experience with the procedure was accumulated (Fig. 3). Therefore, about 10-minute differences noted in comparative analysis are not thought to be significant in clinical practice. Previously, Qiu, et al.3 estimated the learning curve for both the scatter and split group methods. They evaluated the learning curve of 80 cases. Their results showed a similar graph pattern with this study. They divided the learning period into three phases. They defined the first 20 cases as a training phase, and cases 21-40 showed an intermediate phase characterized by unstable operative times. The final group of 41-80 patients revealed a smooth trend, which indicated a well-developed phase. In this study, the moving average for every 10 cases of total operation time was presented as being correlated with estimated learning curve (Fig. 3). Accordingly, cases 20-30 may be a training phase, suggesting a much shorter learning curve period for SFLC.
In conclusion, SFLC can be applied in uncomplicated and well-selected gallbladder disease with tolerable operation time, cost benefits, wound sparing effects, lower pain scores, and with no need for articulating instruments, flexible endoscopes, and specialized one-port devices. However, this study was a retrospective analysis and was subject to selection bias. Therefore, well-designed prospective clinical trials are necessary to analyze the role of SILC in the management of benign GB disease.




 XML Download
XML Download