

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Lung cancer has become one of the most common malignancies for men and women worldwide, and the majority of lung cancer patients have reached the advanced stage by the time of their diagnosis. Although the vast majority of lung cancer cases are attributed to smoking habits, it cannot adequately explain the etiology of lung cancer in nonsmokers, making us to focus on the importance of genetic susceptibility in the risk of lung cancer. Non-small cell lung cancer (NSCLC) is the most common type of lung cancer, comprising nearly 80% of all cases. Chemotherapy with third generation platinum-based doublets is the mainstay for the initial treatment of patients with advanced NSCLC, however, the chemosensitivity differs from person to person, which reflects limited advances in our understanding of the molecular mechanisms underlying lung carcinogenesis and the individual susceptibility to lung cancer. A growing body of evidence suggests that single nucleotide polymorphisms (SNPs) can help elucidate individual differences in lung cancer susceptibility and sensitivity to cytotoxic drugs.1,2
Aberrant DNA methylation is recognized as being a common feature of human neoplasia, with CpG island hypermethylation and global genomic hypomethylation occurring simultaneously in tumors.3 Folate acts as a donor for methyl groups and plays a key role in normal cell growth and replication. Low folate status could lead to DNA damage and instability, alter DNA methylation and eventually result in cell death via apoptosis, which may promote tumor initiation. Furthermore, epidemiological studies have implicated folate deficiency in the development of cancers, including cancers of cervix, colon, lung, and breast.4-7 The methylenetetrahydrofolate reductase (MTHFR) gene is located at the end of the short arm of chromosome 1 (1p36.3) (http://ghr.nlm.nih.gov/gene=MTHFR). MTHFR is a central regulatory enzyme for folate metabolism and irreversibly catalyzes 5, 10-methylene-tetrahydrofolate (THF) into 5-methyl THF,8 which serves as a methyl donor for the methylation of homocysteine to methionine and the precursor of S-adenosylmethionine (SAM). The reduced activity of MTHFR may decrease the methylation of homocysteine to methionine and in turn decrease the level of SAM, resulting in DNA hypomethylation. However, a decreased level of the MTHFR substrate, required for thymidylate synthesis, could lead to uracil misincorporation into DNA, diminished DNA repair and the increased frequency of chromosomal breaks and damage.9 A common SNP (at nucleotide position 677) in the MTHFR gene, resulting in the substitution of an alanine with a valine, has been identified as affecting enzyme activity. Individuals with the MTHFR 677TT variant genotype have approximately 30% enzyme activity in vitro compared with individuals with the 677CC wild-type, and heterozygote carriers have only 60% activity. This mutation leads to DNA hypomethylation, genomic instability and derepression of proto-oncogenes,10 all of which might contribute to carcinogenesis. Because it affects the methylation of DNA and tumor suppressor genes, the MTHFR polymorphism could potentially modulate the efficacy of cytotoxic agents.11
Many studies reported the association between MTHFR polymorphisms and lung cancer risk, but the results remain inconclusive. For example, Kiyohara, et al.12 recently reported that the TT genotype of the C677T polymorphism was significantly associated with an increasing lung cancer risk, being consistent with previous findings reported by Cui, et al.,13,14 and Siemianowicz, et al.14 However, opposite results were shown by Suzuki, et al.15 and Liu, et al.16 A meta-analysis by Zhang, et al.17 suggested that C677T polymorphism was not significantly correlated with lung cancer risk in any genetic models in the total population, and that only 677T variants could decrease the lung cancer risk in females. This discrepancy may be attributed to small sample size, various ethnic groups, diet, environment, and methodologies. In addition, there have been several studies evaluating the influence of MTHFR polymorphisms on the clinical response to platinum-based chemotherapy in advanced NSCLC; all of these studies had small sample sizes, and thus, any single study inevitably lacked the power to reflect a reliable conclusion.13,18,19 Meta-analysis is a useful method to investigate the associations of cancer with genetic variants because it can combine the results of similar studies on the same topic in a quantitative approach. Therefore, we performed meta-analysis to investigate the effect of MTHFR polymorphism on lung cancer risk and clinical response to platinum-based chemotherapy in advanced NSCLC.
MATERIALS AND METHODS
Publication search
A literature search of the PubMed, Ovid, Wanfang and Chinese Biomedicine databases was conducted using the terms: "methylenetetrahydrofolate reductase" or "MTHFR" and "lung" and "neoplasms", without any restrictions on language. All of the studies searched were retrieved, and the references cited in the studies were also reviewed to identify additional published work. Review articles were also screened to identify additional eligible studies. The study search was performed independently by two authors (Jian He and Jingwen Xia).
Selection criteria
Studies on the effect of the MTHFR polymorphism on lung cancer risk were included when the following criteria were met: 1) evaluation of the MTHFR C677T polymorphism and lung cancer susceptibility; 2) case-control study; 3) genotype frequencies available in both cases and controls; and 4) a genotype distribution of the control population that is consistent with Hardy-Weinberg Equilibrium (HWE). Accordingly, articles were excluded using the following criteria: 1) no reported genotype frequencies; 2) reviews, abstracts and repeat studies; or 3) genotype distribution in the control population that is inconsistent with HWE. For the studies with the same or overlapping data by the same authors, the most suitable study with the greatest number of subjects or the most recently published study was selected.
The inclusion criteria for the MTHFR polymorphism on the response to platinum-based chemotherapy in advanced NSCLC were as follows: 1) patients with advanced NSCLC, 2) patients receiving platinum-based chemotherapy and 3) assessment of the MTHFR C677T polymorphism and chemosensitivity. The exclusion criteria were as follows: 1) the response rate stratified by the SNP could not be obtained through any method, and 2) the article did not compare the response rate.
Data extraction
The data were manually extracted from each study by Ning Zhu and Yi Gong independently. The following information was collected from each enrolled article comparing the MTHFR polymorphisms with lung cancer risk: first author's name, publication date, country, ethnicity, source of controls, matching criteria, sample size, smoking status, and number of C677T genotypes for both cases and controls. Information about the MTHFR polymorphisms and the response to platinum-based chemotherapy was also extracted as follows: first author's name, publication date, country, ethnicity, sample size, clinical stage, number of C677T genotypes, treatment protocols, and number of responders or non-responders. Disagreements were resolved by discussion between the two authors. When necessary, another author (Xiaodong Chen) was consulted to resolve the dispute.
Statistical methods
The meta-analysis mainly examined the overall association for the allele contrast, the contrast of homozygotes, and the recessive and dominant models with lung cancer risk. The effect of association was indicated as the odds ratio (OR) with the corresponding 95% confidence interval (CI). We also evaluated the effect of the C677T polymorphisms on the response rate to platinum-based chemotherapy. In this meta-analysis, complete responders and partial responders were classified as responders, and non-responders had stable or progressive disease. The OR was taken as a measure of the positive effect of chemotherapy. The pooled OR and 95% CI were calculated. Analyses were weighted by trial size. An OR equal to 1 indicates a lack of association between the SNP and the treatment response rate. An OR greater than 1 corresponds to a direct correlation between the treatment response rate and the wild-type allele. An inverse correlation was indicated by an OR of less than 1. The heterogeneity between studies was tested using the Q statistic.20 If the heterogeneity was considered statistically significant with p<0.10, the pooled OR of each study was calculated by a fixed effects model; otherwise, a random effect model was used. Heterogeneity was quantified using the I2 metric, which is independent of the number of studies in the meta-analysis (I2<25% no heterogeneity; I2=25-50% moderate heterogeneity; I2>50% large or extreme heterogeneity).21 Publication bias was investigated by the funnel plot, in which the standard error in the log (OR) in each study was plotted against the OR. An asymmetric plot suggested a possible publication bias. Begg's test and Egger's test were used to statistically assess publication bias, and a p value of <0.05 was considered significant. HWE was tested by the chi-square test (http://ihg2.helmholtz-muenchen.de/cgi-bin/hw/hwa1.pl). The analyses were performed using the software ReviewManage (V5.0; the Cochrane Collaboration, Oxford, England) and STATA 11.0 (StataCorp, TX, USA) (http://www.stata.com).
RESULTS
Search result
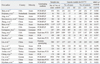
Overall, a total of 62 references were retrieved from PubMed, Ovid, Wanfang, and the Chinese Biomedicine database in the initial search. After scanning the titles and abstracts, 27 articles concerning the association between the MTHFR C677T polymorphisms and lung cancer risk or chemosensitivity for NSCLC were retained for the following screen. After reading through the full texts, six articles were excluded for the following reasons: one was not a case-control study,22 one did not have sufficient information,23 two were duplicate publications or shared the same data,24,25 and two did not assess the response rate to platinum-based chemotherapy in advanced NSCLC.26,27 Finally, nineteen studies, including 11644 cases and 12024 controls that assessed the relationship between the MTHFR C677T polymorphism and lung cancer risk, were determined to be eligible for the meta-analysis.10,12-16,28-38 Three studies including 406 patients with advanced NSCLC were eventually enrolled to evaluate the predictive value of the MTHFR C677T polymorphism on the response rate to platinum-based chemotherapy (Fig. 1).13,18,19 The characteristics of the identified studies are listed in Table 1 and 2.
MTHFR polymorphisms and lung cancer risk in the total population
The brief results of this meta-analysis are summarized in Table 3. For studies evaluating the MTHFR C677T polymorphism in the total population, the overall OR for the 677T allele vs. the 677C allele was 1.11 (95% CI, 1.01-1.22; p=0.02). There was high heterogeneity (p<0.00001) among the 19 studies, and thus, a random-effect model was used. The overall OR for variant-type TT homozygote vs. wild-type CC homozygote was 1.24 (95% CI, 1.04-1.48; p=0.02) in the random-effect model. This analysis showed that the TT homozygote was significantly correlated with lung cancer risk in the recessive model (TT homozygote vs. CC homozygote and CT heterozygote) (OR=1.19; 95% CI, 1.03-1.37; p=0.02). However, the dominant model (TT homozygote and CT heterozygote vs. CC homozygote) produced a negative result (OR=1.11; 95% CI, 0.98-1.24; p=0.09).
Subgroup analysis
The enrolled studies were stratified for further analysis by ethnicity, histological type, smoking status and gender. The results are listed in Table 3. Twelve studies evaluated the MTHFR C677T polymorphism and lung cancer risk in Asians.12,13,15,16,29,30,32,35,37-40 Among them, nine studies assessed the association in the Chinese population.13,16,29,30,32,35,38-40 Six studies reported the association in European populations.10,14,28,31,33,34,36 However, when stratified by ethnicity, there was no significant association observed in any genetic model of the MTHFR C677T polymorphism. In the subgroup analysis by histological type, data on the MTHFR C677T polymorphism in NSCLC were obtained from five studies,13-15,36,38 and data on SCLC were reported by only two studies.14,36 We found that the genetic models of the MTHFR C677T polymorphism were significantly correlated with increasing risk of NSCLC (677T allele vs. C allele: OR=1.18; 95% CI, 1.06-1.33; p=0.004; TT homozygote vs. CC homozygote: OR=1.57; 95% CI, 1.05-2.34; p=0.03; the dominant model: OR=1.28; 95% CI, 1.02-1.60; p=0.03), with the exception of the recessive model (OR=1.50; 95% CI, 0.97-2.31; p=0.07). No relationship was observed in small cell lung cancer for any comparison model. Five studies evaluated the relationship with smoking status.12,16,31,36,38 We found that the dominant model and the variant T allele of the MTHFR C677T polymorphism showed a significant association with the lung cancer susceptibility of ever smokers (the dominant model: OR=0.83; 95% CI, 0.72-0.97; p=0.02; 677T allele vs. 677C allele: OR=0.88; 95% CI, 0.78-0.99; p=0.03), however, that the results of other genetic models were negative. In addition, three studies assessed the relationship according to gender.31,36,38 We found that male TT homozygote carriers had a 36% higher risk (OR=1.36; 95% CI, 1.01-1.84; p=0.04), but a protective effect of lung cancer susceptibility was observed in females in the allelic contrast and homozygote models (677T allele vs. 677C allele: OR=0.81; 95% CI, 0.68-0.97; p=0.02; TT homozygote vs. CC homozygote: OR=0.63; 95% CI, 0.41-0.95; p=0.03). Other genetic models showed null results in either males or females.
MTHFR 677 C→T polymorphism on the response to platinum-based chemotherapy for advanced NSCLC
The number of variant TT homozygote carriers was 71, and the number of CC homozygote or CT heterozygote carriers was 318. The overall response rate of the TT carriers was 46.5%, and that of the CC or CT carriers was 33.7%. The results concerning the overall response rates showed no heterogeneity among the trials (p=0.31, I2=16%). The pooled OR was 1.72 (95% CI, 1.01-2.93, p=0.04), which indicated that patients with the MTHFR 677TT genotype showed a better response to platinum-based chemotherapy in advanced NSCLC in the recessive model (Fig. 2).
Publication bias
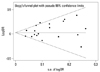
Publication bias was assessed by Begg's funnel plot and Egger's test. The shape of the funnel plots appeared symmetrical in the MTHFR 677T allele versus C allele for lung cancer risk, suggesting the absence of publication bias (Fig. 3). Then, Egger's test was used to provide statistical evidence of funnel plot asymmetry (t=1.37, p=0.187), which indicated a lack of publication bias of the current meta-analysis. Other results also did not suggest any evidence of publication bias (TT homozygote vs. CC homozygote, t=1.30, p=0.211; TT homozygote vs. CC homozygote+CT heterozygote, t=1.32, p=0.204; TT homozygote+CT heterozygote vs. CC homozygote: t=1.00, p=0.334). Similarly, no publication bias was detected for the association between the recessive model for the MTHFR C677T polymorphism and the response rate to platinum-based chemotherapy (t=-2.98, p=0.206).
DISCUSSION
As a cruial enzyme, MTHFR could regulate folate metabolism, which affects DNA synthesis, repair and methylation. Several diseases have been associated with the MTHFR C677T polymorphism, including acute lymphocytic leukemia, colon cancer, cervical cancer and probable cardiovascular disease.41-44 Although previous studies have assessed the predictive value of the MTHFR polymorphisms on lung cancer risk, the results are still inconclusive and unreliable. Several meta-analyses had been reported on the lung cancer risk associated with the MTHFR C677T polymorphism,17,45,46 all of which suggested no significantly elevated lung cancer risk in any genetic models in the total population. Therefore, we performed this meta-analysis to clarify the actual association between the MTHFR C677T polymorphism and lung cancer risk or chemosensitivity.
We found that the allelic contrast, homozygous contrast and recessive model of the MTHFR C677T polymorphism were significantly associated with increased lung cancer risk in the total population. It is well known that the pathogenesis of lung cancer is complex: several factors, including ethnicity, environmental factors and gene-gene and gene-environment interactions, are all involved in this process and contribute to the genesis of lung cancer. In the subgroup analysis by ethnicity, we observed that no significantly elevated lung cancer risk was found in any genetic models in Asian, European or Chinese populations. When stratified by histological type, we found that the genetic models of the MTHFR C677T polymorphism showed a significant association with an increasing risk of NSCLC, except for the recessive model, and that no genetic model of the MTHFR C677T polymorphism was significantly correlated with the risk of SCLC; these results were consistent with the results of a recent meta-analysis by Hou, et al.47 Because smoking is the predominant risk factor for lung cancer, the interaction between the MTHFR genotype and individual smoking habits was also analyzed by stratifying the individual smoking status. The dominant and allelic contrast models showed a notably protective value on lung cancer susceptibility for ever smokers. In addition, the recessive model of C677T had a higher risk in males, and the variant TT homozygote and the T allelic contrast had a protective value in females.
As mentioned above, the MTHFR C677T polymorphism might be a genetic marker for an increased risk of NSCLC, but what about the C677T polymorphism for the response to platinum-based chemotherapy in advanced NSCLC? Platinum-based chemotherapy is still the standard chemotherapy for the treatment of advanced NSCLC patients, but the chemotherapy response rate is well known to vary from person to person. It's indicated that SNPs could partly explain inter-individual differences in drug response and toxicity. Moreover, the association between MTHFR 677 C→T polymorphism and NSCLC risk was investigated by several studies, the results are still controvential. A study by Alberola, et al.18 indicated no differences in the response rate in association with the MTHFR genotype. However, our meta-analysis found that MTHFR 677TT genotype patients could have a better response to platinum-based chemotherapy in the recessive model, which was in agreement with the result reported by Cui, et al.13 Thus, the MTHFR 677TT genotype might influence the treatment outcome of clinical response to platinum-based chemotherapy in advanced NSCLC. Both positive and negative studies have been published, and formal testing revealed no evidence of publication bias in this meta-analysis.
Several potential limitations should be taken into consideration when interpreting these results. First, the heterogeneity among the nineteen studies was extreme. To eliminate heterogeneity, we stratified the nineteen studies according to ethnicity, but the heterogeneity still existed. In the subgroup analysis of the histology subtype, the heterogeneity remarkably decreased and was even removed in some of the genetic models. Thus, the histology subtype may partially contribute to the high heterogeneity. Other possible reasons are as follows. 1) An Asian or European ethnicity is a rough classification, and there is a wide variation in the MTHFR 677T allele frequency across different populations. 2) The allele frequency is different in different histological subtypes. Arslan, et al.36 reported that the MTHFR 677T allele frequency was higher in the NSCLC group. 3) The controls and genotyping methods are not uniform. Second, our sample size was relatively small, especially in some stratified analyses. Thus, most of the associations which we have described may be due to chance. In the meta-analysis of chemosensitivity, the data for the recessive model could be obtained from three enrolled studies,13,18,19 but the data for the other genetic models could be extracted only from two of the three studies.13,19 A sample size that is too small could weaken the power of the conclusion. Thus, we just evaluated the association between the recessive model of the MTHFR C677T polymorphism and the response to platinum-based chemotherapy. Third, because of the lack of a unified grading standard of folate intake, alcohol consumption, or age in the available studies, the role of these risk factors in the MTHFR C677T polymorphism and lung cancer could not be addressed in this meta-analysis.
In conclusion, our meta-analysis suggests that the MTHFR C677T polymorphism might be a genetic marker for an increased risk of lung cancer, and that MTHFR 677TT genotype carriers could have a better response to platinum-based chemotherapy in advanced NSCLC in the recessive model. Therefore, we believe that these findings will benefit a substantial number of lung cancer patients, especially those with advanced NSCLC. However, our results still need to be confirmed by additional, larger case-control studies, especially with respect to chemotherapy in advanced NSCLC.




 XML Download
XML Download