

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
After radical resection of rectal carcinoma, local recurrence (LR) remains a major problem, ranging in occurrence between 7.6 and 11.3%.1,2 With the introduction of novel treatment modalities such as total mesorectal excision and neoadjuvant chemoradiotherapy, the rate of local recurrence in rectal cancer has decreased significantly.3-5
Circumferential resection margin (CRM) in rectal cancer has been defined as the non-peritonealized surface of a resection specimen created by dissection of the subperitoneal aspect at surgery.6 CRM involvement occurs at a rate ranging from 7.3 to 25%.6-8 Many studies have demonstrated that CRM involvement is able to predict local recurrence and poor prognosis in patients with rectal cancer.7-11 For this reason, CRM positivity had been regarded as an important short-term end-point in well-designed clinical trial for rectal cancer.12 In contrast, some previous investigators reported that CRM involvement showed no correlation with local recurrence or long-term prognosis.13,14 These results were based upon curatively operated patients with rectal cancer of several stages treated with or without neoadjuvant chemoradiotherapy. However, studies focusing on the prognostic impact of CRM involvement, especially in stage III rectal cancer patients treated with curative resection followed by adjuvant chemoradiotherapy, are rarely reported.
The aim of this study was to evaluate whether CRM involvement could be a clinical parameter for predicting local recurrence or long-term prognosis in stage III rectal cancer patients.
MATERIALS AND METHODS
Patient eligibility
Between January 1, 1990 and December 31, 2007, a total of 811 patients diagnosed with stage III adenocarcinoma of the rectum within 12 cm from the anal verge after undergoing curative resection followed by selective adjuvant chemoradiotherapy were extracted from our prospectively collected database. Of the 811 patients, due to patient refusal, poor performance status, or other reasons, only 525 patients completed the scheduled adjuvant chemoradiotherapy. Among the 525 patients, 76 in whom CRM was not measured were also excluded. The remaining 449 patients were eligible for this study.
Surgery and follow-up
Patients were staged via either a combination of appropriate imaging studies such as chest radiography, transrectal ultrasonography, pelvic magnetic resonance imaging (MRI), abdominopelvic computed tomography (CT), or 18-FDG positron emission tomography (PET) before the operation. Patients received mechanical bowel preparation with polyethylene glycol solution the day before surgery. Prophylactic antibiotics were administered at the induction of anesthesia. The inferior mesenteric artery was doubly ligated from the aorta at its root. During surgery, care was taken to preserve the hypogastric nerve. The inferior mesenteric vein was ligated at the lower border of the pancreas. A sharp pelvic dissection was performed from the entrance to the pelvic cavity down to the pelvic floor, or the anal hiatus within the levator ani muscles along the visceral mesorectal fascia.15 Tumor-specific mesorectal excisions were performed according to the tumor distance from the anal verge. For cases of upper rectal cancer, the mesorectum was excised 4 cm from the lower edge of the tumor. Total mesorectal excision was performed for cases of mid and low rectal cancer at the level of the levator ani muscle.16 A potentially curative procedure was defined as one in which the surgeon believed that the entire tumor had been removed at the time of surgery. All of the patients registered in the prospectively collected colorectal database in our hospital made postoperative follow-up visits every 2-3 months for 3 years. After 3 years, follow-up visits were reduced to every 6 months until 5 years, and annually thereafter. A physical examination, serum carcinoembryonic antigen (CEA) level measurement, and chest radiography were performed at each follow-up visit. Abdominopelvic CT scans and bone scintigraphies were performed annually. Chest CT, pelvic MRI, or 18-FDG PET scan was performed as indicated according to the clinician's decision. Patient follow-up lasted until the cutoff date (October 31, 2010), or when the patient died. The median follow-up period for all the patients was 56.6 months (range, 4.9-230.9 months).
Pathologic examination
Lymph nodes were retrieved after gross examination and manual palpation. All dissected and retrieved lymph nodes were stained with hematoxylin and eosin (H&E), and examined by light microscopy for the presence of tumor metastasis. After confirming their proper orientation, surgical specimens were thoroughly inspected during gross examination. CRM was then identified as described by Quirke, et al.9 In some cases, the CRMs of the freshly received specimens were stained using the Davidson Marking System (Bradley Product, Inc., Bloomington, MN, USA) and subsequently fixed for 48 h. Dissection consisted of slicing 5 mm serial sections of the whole tumor and the surrounding mesorectum in the transverse plane. Using a pathology slide (H&E stain), the shortest distance was measured from the microscopically lateral portion of the tumor to the stained CRM.11 CRM involvement was defined as a distance from the circumference margin of ≤1 mm.9 Patients were divided into two groups: "CRM-positive group" (CRM ≤1 mm) and "CRM-negative group" (CRM >1 mm) according to the shortest distance between the CRM and the tumor (Fig. 1).
Adjuvant chemoradiotherapy
In this study, 5-FU (450 mg/m2 for 5 days) and leucovorin (20 mg/m2 for 5 days) was given intravenously each month with six cycles. A total dose of 5040 cGY of external beam radiation therapy was delivered after the second round of chemotherapy (as supplied by a 6 MV/10 MV dual photon linear accelerator, CLINAC 2100 C, Varian, Palo Alto, CA, USA) in 30 fractions of 180 cGY each, five times weekly to the pelvic cavity with individually shaped portals and using a four-field box technique.17
Definition of recurrence
LR was defined as any recurrent tumor growth within the pelvic cavity or perineal area confirmed by clinical, radiological or pathological evidence. For histological confirmation, an imaging-guided biopsy was performed, when possible. Overall local recurrence rates were calculated as the sum of isolated LR and LR with concomitant systemic metastases.8 Systemic recurrence was defined as recurrence outside the pelvis.
Lymph node ratio evaluation
Lymph node ratio (LNR) was defined as the ratio of metastatic lymph nodes to total retrieved lymph nodes. Patients were categorized into three groups based on their LNR: Group 1=0<LNR≤0.099 (LNRG1); Group 2=0.01≤LNR ≤0.249 (LNRG2); or Group 3=0.25≤LNR≤1.0 (LNRG3). This cut-off value was chosen based on the tertile number of LNR in this study group.
Statistical analysis
All statistical analyses were performed using SPSS software, version 18.0 (SPSS, Chicago, IL, USA). Categorical variables were analyzed using the chi-square test or Fisher's exact test, and continuous variables were analyzed using Student's t-test. Local recurrence-free survival was defined from the date of surgery to the date of detection of local recurrence. Systemic recurrence-free survival was defined as the date of surgery to the date of detection of systemic recurrence. Differences in survival and recurrences between the groups were compared using the Kaplan-Meier method and tested with the log-rank test. Factors associated with local-recurrence free survival and systemic-recurrence free survival were analyzed by a Cox proportional hazards model done by a backward stepwise selection of variables. p-values <0.05 were considered statistically significant.
RESULTS
Patient characteristics
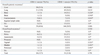
Of the 449 patients, 79 (17.6%) were classified as CRM-positive group and 370 patients (82.4%) as CRM-negative group. The clinicopathological characteristics of the patients are summarized in Table 1. There were significant differences in CRM status according to the degree of lymphovascular invasion, tumor size, pathologic T stage, and pathologic N stage.
Local recurrence (LR) and systemic recurrence (SR)
Overall, 203 patients (45.2%) exhibited recurrence during the study period. Of these patients, 42 patients (20.7%) were CRM positive and the remaining 161 patients (79.3%) were CRM negative. Isolated SR rate was higher in the CRM-positive group than that of the CRM-negative group, although the p-value thereof was only marginally significant (40.5% vs. 29.7%, p=0.062) (Table 2).
Among various patterns of SR, liver metastasis and carcinomatosis were significantly higher in the CRM-positive group than in the CRM-negative group (25.3% vs. 10.8%; p=0.001, and 6.3% vs. 1.9%; p=0.043, respectively) (Table 3).
Survival analysis
The 5-year overall survival rate was 54.2% in the CRM-positive group and 66.1% in the CRM-negative group. On univariate analysis, LNR group and pathologic N stage were shown to be significant predictors of LR, while lymphovascular invasion, circumferential resection margin involvement, LNR group, pathologic T stage, and pathologic N stage were shown to be significant predictors of SR (Table 4). Cox proportional hazards analysis showed that LNR group was an independently predictor of LR. Additionally, preoperative CEA level, CRM involvement, pathologic N stage, and LNR group were shown to be independent predictors of SR on multivariate analysis (Table 5).
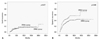
The cumulative incidences of LR and SR according to CRM status are shown in Fig. 2. The overall local recurrence rate (the sum of isolated LR and LR with concomitant distant metastases) was not different regardless of whether the patient was CRM positive or not (5-year LR rate in the CRM-positive group 13.0% vs. CRM-negative group 13.5%; p=0.677).
DISCUSSION
In this study focusing on stage III rectal cancer patients who were treated with curative resection followed by complete adjuvant chemoradiotherapy, CRM involvement proved to be an independent adverse prognostic factor. However, local recurrence rate did not differ between CRM-positive and CRM-negative patients.
The clinical relevance of CRM involvement in rectal cancer for oncological outcomes has been well documented since Quirke, et al.9 first reported the importance of CRM on prognosis. It was reported that CRM involvement increased the risks of both local recurrence and distant metastases.7-10 In contrast, Hall, et al.13 reported that although circumferential margin positive was associated with poor prognosis in terms of distant metastasis and survival in rectal cancer, CRM involvement did not greatly increase the local recurrence rate due to the early development of distant disease rather than local failure. Khani, et al.14 reported that there were no significant differences in local recurrence and survival between CRM positive and negative tumors after preoperative radiotherapy and postoperative chemotherapy. These previous studies included all stages of rectal cancer patients with or without preoperative chemoradiotherapy. In contrast, this study included a relatively large number of stage III rectal cancer patients in whom no preoperative chemoradiotherapy had been applied. Therein, a strong positive association was observed for CRM involvement with distant recurrence. However, local recurrence rate was not correlated with CRM involvement status. This result might give further evidence to the report of Hall, et al.13 In our study, the median time to diagnosis of systemic recurrence from the primary resection in the CRM-positive group was shorter than that of the CRM-negative group (13.3 vs. 19.7 months; p=0.052) (data not shown). This result might have originated from the more aggressive tumor biology in the CRM-positive group than in the CRM-negative group. For this reason, the rate of local recurrence could have appeared lower than it really was in the CRM-positive group.
It is known that low rectal cancers entails a higher positive CRM rate than upper rectal cancer.8 In the present study, the CRM positive rate in upper rectal cancer was higher than that of low rectal cancer, although this difference was not statistically significant. The reason for this phenomenon is difficult to explain. During the early periods of this study, abdominoperineal resection (APR) was frequently performed for low rectal cancer. In this data set, the CRM positivity rate was 14.5% for patients who underwent APR and 18.4% for patients who underwent a sphincter-preserving procedure (p=0.335, data not shown). From these data, we deduced that APR had been with excellently performed in our center, which could have lowered the CRM involvement rate in low rectal cancer.
With regard to local recurrence-free survival, LNR retained its significance in the multivariate analysis. With regard to systemic recurrence-free survival, preoperative CEA level, LNR, pathologic N stage, and CRM retained their statistical significance in the multivariate analysis. These results are on par with published data. Recently, LNR was reported as an effective parameter for predicting patient prognosis in node positive colorectal cancer, though debate still exist as to the ideal cut-off value.18 In our analysis, LNR also proved to be an independent prognostic factor of local recurrence-free and systemic recurrence-free survival.
Neoadjuvant chemoradiotherapy (NCRT) could further lower the local recurrence rates compared with adjuvant chemoradiotherapy in rectal cancer.5 Clinical stages of T3 or T4 and/or node positivity was regarded as a good candidate for NCRT. Due to enhancing diagnostic accuracy, especially in pelvic MRI, preoperative threatened or involved CRM was also regarded as an essential indication for NCRT to reduce CRM positive rates.19,20 According to our observations of a positive relationship between systemic recurrence and CRM involvement, threatened or involved CRM groups defined by preoperative MRI should be regarded as an immediate candidate for more urgent and intensified neoadjuvant chemotherapy in clinical trials. Accordingly, further prospective studies are warranted.
In conclusion, in patients with stage III rectal cancer treated with curative resection followed by adjuvant chemoradiotherapy, although CRM involvement was an important adverse prognostic factor, local recurrence rate was not correlated with CRM involvement status. For this reason, CRM involvement should be considered as an indicator of more advanced disease. Additionally, these features should be considered in establishing end-points in further randomized controlled trials for rectal cancer.





 XML Download
XML Download