

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
A mandibulotomy is highly effective in removing tumors of the posterior aspect of the oropharynx and oral cavity.1-3 However, there have been reports of various related complications such as nerve injury, inadvertent fracture of the osteotomy segment, malocclusion, fistula, wound dehiscence, infection, non-union, and osteoradionecrosis.4-11 Various modifications in osteotomy design, fixation method, and technique have thus been put forth to reduce these complications.12-18
Although the complication rate associated with mandibulotomy has fallen from 35%7 to 10.5%,19 there remain unnecessary procedures such as incisor extraction19 or intermaxillary fixation.20 In our previous study, we analyzed factors contributing to mandibulotomy complications in 103 patients retrospectively and suggested a modified mandibulotomy technique based on our results.21 In another paper, we introduced our modified mandibulotomy technique, consisting of a lower lip-splitting for optimal visualization, modified stair-step osteotomy with thin saw blade and osteotome for greater bony stability, and plate-precontouring and combination fixation with monocortical osteosynthesis and bicortical osteosynthesis to reposition the hemimandibular segments to preoperative condition.22 There was no incisor extraction or intermaxillary fixation postoperatively.
This study aims to review the records of patients who received our modified mandibulotomy over a 5-year period and to assess the efficacy of our technique.
MATERIALS AND METHODS
Thirty patients who had undergone a uniform surgical technique between 2006 and 2010 consisting of a lower lip-splitting, modified stair-step osteotomy with thin saw blade and osteotome after plate-precontouring and combination fixation with monocortical osteosynthesis (miniplate) and bicortical osteosynthesis (maxiplate and bicortical screws), with at least 14 months postoperative follow-up, were selected and reviewed retrospectively.
Due to the retrospective nature of this study, the Institutional Review Board waived informed consent from the patients.
All patients were operated on in the Departments of Otorhinolaryngology and Oral and Maxillofacial Surgery. All the mandibulotomies were done by the Department of Oral and Maxillofacial Surgery.
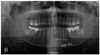
The method was as follows: after a midline lip incision, the mucoperiosteum was carefully lifted to access the planned osteotomy site anterior to the mental foramen. A panoramic radiograph confirmed the space between the teeth adjacent to the osteotomy line. Bony indentation was accomplished in a staircase fashion using a thin oscillating saw blade. This indentation served as an osteotomy marker and permitted precise placement of the miniplates. After bony indentation, a 4-hole 2.4-mm non-locking miniplate was positioned on the mandibular symphysis inferior border and fixed bilaterally with one bicortical screw. The other screw holes were predrilled. Subsequently, a 4-hole, 2-mm nonlocking miniplate was put into place 3 to 5 mm below the root apices and fixed with monocortical screws as described above. Plate contouring and preadaptation are both highly critical in preventing postoperative malocclusion. Following plate and screw removal, a thin oscillating saw blade was used to perform the osteotomy. Beginning from the alveolar portion, an osteotomy for a buccal corticotomy was performed on the preconfirmed space continuing vertically to the mandible, at which point the saw blade turned horizontally to the extent of its blade width, then turned vertically again, stopping at the inferior border of the mandible. The alveolar portion of the teeth was carefully cut in order to prevent tooth damage. A lingual corticotomy, in contrast, can be performed through the marrow space from the buccal side. A lingual osteotomy should not be completed with an oscillating saw due to the higher probability of postoperative malocclusion in the presence of a bony gap. To avoid iatrogenic fracture while malleting the osteotome, the oscillating saw should continue as close to the outer surface of the lingual cortex as possible in a lingual osteotomy, but no further (Fig. 1). Following the indentation of the lingual cortex, the lingual corticotomy is completed from the buccal side through the marrow space, using a straight osteotome to split the mandible. This intentional lingual cortical fracture prevents hemimandibular segments from rotating and promotes postoperative healing. Moreover, the inferior border of the mandible should be entirely cut to avoid unwanted splitting while malleting the osteotome due to its thick cortex (Fig. 2). After the tumor resection, the hemimandibular segments were repositioned and preformed miniplates were placed on the predrilled screw holes, then tightened. Postoperatively, the mandible can function normally without application of an arch bar.
RESULTS
There were 8 women and 22 men, with an average age of 56.5 years (range: 38 to 72 years). All the patients involved malignancies were squamous cell carcinoma. The main primary sites of the patients who underwent a mandibulotomy were the tonsil [14 (46.7%) patients], the base of tongue [7 (23.3%) patients], the oral tongue [4 (13.3%) patients], the retromolar pad area [2 (6.7%) patients], and others [3 (10%) patients]. Others included buccal cheek, floor of mouth (FOM), and soft palate. 23 patients received postoperative radiation therapy, among whom 8 patients also received chemotherapy. Four (13%) mandibulotomy-related complications occurred in 4 (13%) patients, consisting of one case of orocutaneous fitula due to osteomyelitis, one of periodontal abscess, one of non-union, and one case of tooth-pulp necrosis. However, only 2 (6.7%) required additional operation under general anesthesia. One patient required incisor extraction due to lack of osteotomy space because of dental crowding.
DISCUSSION
A mandibulotomy, indicated for tumors of the tonsil, retromolar pad, and base of tongue when there are no clinical or radiological findings of bony invasion, can provide a clear surgical view of the primary lesion and facilitate an en-bloc resection.1-3 In this study, 70% of patients had tumors in the posterior oral cavity and oropharynx. Other patients had tumors in the buccal cheek, FOM, and soft palate where lack of access made peroral approach impracticable.
An ideal mandibulotomy technique requires no intermaxillary fixation, preserves the occlusion in a precise way, enables early function, entails no secondary procedures, and is free of complications.23
The main problem with the original mandibulotomy technique concerned the postoperative fragment mobility due to a bony gap on the osteotomy line. In spite of rigid flxation, the bony gap remains, and mobility of unstable fragments increases the probability of postoperative complications such as malocclusion, nonunion, and osteoradionecrosis following postoperative irradiation. Advanced instruments and surgical skills notwithstanding, these postoperative complications continue to arise.20
According to Engroff, et al.23 because the mandible is restored to its premorbid state, a small continuity defect is created matching the thickness of the saw blade. Because no interfragmentary friction, buttressing, or load sharing exist, principles of fracture reduction and fixation do not apply in this situation. Our modified mandibulotomy was designed to reduce these complications by inducing intentional fracture and utilizing corresponding fixation. The technique described here consists of a modifled bicortical splitting of the symphysis which leaves the lingual cortex untouched and concludes with a fine osteotome. The bony gap is thus restricted to the buccal cortex and bony marrow, enabling intimate lingual bony contact during reconstruction without dental arch distortion. Moreover, predrilled screw holes ensure accurate alignment of the buccal and marrow segments during reconstruction.
In our previous study,21 it was possible to restore preoperative occlusion and function immediately with 1 monocortical osteosynthesis and 1 bicortical osteosynthesis fixation without intermaxillary fixation. Moreover, with a median or paramedian stair-step fashioned osteotomy, it was possible to avoid damage to the mental nerve and digastrics muscle in the inferior border and to promote bony healing due to maximal bony contact.
Controversy has arisen regarding the efficacy of a simultaneous extraction of the teeth adjacent to the osteotomy site during mandibulotomy. Dubner and Spiro24 advocated preserving the teeth for a more stable occlusion postoperatively. In our technique, it is possible to preserve the mandibular incisor because osteotomy with an oscillating saw is complete within the final 2 to 3 mm of interdental alveolar bone. A thin osteotome is then used to complete the lingual osteotomy and the alveolar portion as described above. In this study, the only patient who underwent an incisor extraction to obtain osteotomy space due to dental crowding experienced normal postoperative healing without complications. Considering postoperative additional prosthetic costs, it is preferable to preserve the teeth unless specific periodontal problems cause complications.
In esthetic terms, lip-splitting mandibulotomy also provides satisfactory results in scarring and low self-perception of disfigurement for patients.25
Four (13%) mandibulotomy-related complications occurred in 4 (13%) patients. One case of tooth pulp necrosis and one case of periodontal abscess were considered minor dental complications manageable under local anesthesia with endodontic treatment and curettage. One case of orocutaneous fitula due to osteoradionecrosis was also considered a minor dental complication because the lesion was confined to the alveolar ridge, but the patient passed away before the treatment due to tumor recurrence and general weakness. One case of non-union required additional extraction and iliac crest bone graft. Therefore, only two (6.7%) required additional operation under general anesthesia. Although it is generally believed that non-union may result from excess motion at the osteotomy site,23 the effect of postoperative radiation therapy could not be excluded in this case.
In conclusion, of a total four (13%) mandibulotomy-related complications, only two (6.7%) required additional operation under general anesthesia. Therefore, our modified mandibulotomy meets the criteria for an ideal mandibulotomy technique relatively well because it requires no intermaxillary fixation, can preserve the occlusion in a precise manner, allows early function, requires no secondary procedures, and results in few complications (Fig. 3).


 XML Download
XML Download