

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
At present, a prostate specific antigen (PSA) level of 4 ng/mL is widely used as the cutoff value for recommendation of a prostate biopsy. In this cutoff value, the sensitivity is 67.5-80%, but the specificity is only 20-30%.1-3 Other indexes such as PSA velocity (PSAV) and PSA density (PSAD) were introduced thereafter in order to compensate the low specificity of PSA level, and several previous studies proved the effectiveness of these new indexes for the early detection of prostate cancer (PCa).4,5 However, despite a possible relationship between these indexes and PCa, the roles of these indexes in early detection of PCa remains a matter of controversy.6-8
To compensate the low specificity of PSA level and to confirm other important factors for PCa detection at biopsy, we investigated the relationship between various factors including the initial and last PSA level, age, PSAV, PSAD, prostate volume, and follow-up period and outcomes of prostate biopsy through cumulative PSA follow-up data of a cohort in our hospital's health promotion center.
MATERIALS AND METHODS
Study population
The current study was a single center, retrospective analysis. A cohort of 1035 men who visited our hospital's health promotion center and were tested for their serum PSA levels more than two times between January 2001 and November 2011 were the subjects of this study. Among them, 17 men with an elevated PSA level due to chronic prostatitis or with a history of 5-α-reductase use for benign prostate hyperplasia treatment were excluded from this study. Finally, 116 men who had a change in the PSA level from less than 4 ng/mL to more than 4 ng/mL underwent transrectal ultrasound (TRUS) guided prostate biopsy. Median age was 55.9 years (range 41-78). The mean follow-up period was 83.7 months (range 12-127).
Measurement
PSA levels were measured by using ARCHITECT total PSA assay (Abbott Diagnostics inc., Abbott Park, IL, USA) in our hospital. Levels were measured before digital rectal examination or TRUS to minimize interference. Prostate volume was calculated by the ellipsoid formula, [(π/6)×(width of the maximal transverse dimension)×(length of the maximal anteroposterior dimension)×(height of the maximal superoinferior dimension)], using values obtained from TRUS (HDI 3500, Philips Medical Systems, Seattle, WA, USA). The height, width and length of a prostate were measured from two orthogonal views (e.g. transverse and sagittal plane) with two-dimensional ultrasound in this study. The 12-core biopsy scheme was used in our institution including a standard sextant, which was originally described by Hodge, et al.9 and three core biopsies was used in case of hypoechoic lesions on TRUS. Biopsies were performed under ultrasound guidance using an 20-gauge, 22 mm, BARD® Magnum® reusable core biopsy instrument (C.R Bard inc., Murray Hill, NJ, USA). PSAV was calculated by using two-point simple method, and defined as [PSAV=(PSA level of last visit-PSA level of initial visit)/follow-up period]. PSAD was defined as [PSAD=PSA/prostate volume]. We used prostate volume and PSAD measured by TRUS at the time of prostate biopsy.
Statistical analysis
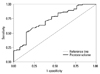
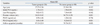
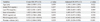
Between the PCa group and the non-PCa group, the initial PSA level, the last PSA level, the age, the prostate volume, the PSAD, the PSAV and the follow-up period were compared by Mann-Whitney U test (Table 1). To identify the predictive factors for PCa, univariate and multivariate logistic regression analysis with enter selection were conducted (Table 2). Odds ratios (ORs) and 95% confidential intervals for all covariatives were calculated. Predictive accuracy was quantified using the area under the curve (AUC) of the receiver operator characteristic (ROC) analysis (Fig. 1).10 SPSS 12.0 (SPSS Inc., Chicago, IL, USA) software was used for the statistical analyses. A p-value <0.05 was considered statistically significant. The Institutional Review Board of our medical institution approved this study (IRB No. 2013-023).
RESULTS
Of the 116 men, 26 (22.4%) were diagnosed with PCa by prostate biopsy. The PCa detection rates between PSA levels of 4.1-10.0 ng/mL was 18% (18 of 98 patients) and PCa detection rate in PSA levels over 10 ng/mL was 47% (8 of 18 patients).
The mean initial PSA and last PSA level during the follow-up was 1.91 and 8.07 ng/mL, respectively. The mean PSAV was 1.16 ng/mL/year (range 0.06-20.99). The mean prostate volume was 34.3 mL (range 9.7-106.0) and the mean PSAD was 0.28 ng/mL/mL (range 0.05-2.43).
Of the evaluated variables, the prostate volume at biopsy (36.7 mL vs. 26.0 mL, p=0.002), the PSAD at biopsy (0.24 ng/mL/mL vs. 0.41 ng/mL/mL, p=0.001) and the follow-up interval (79 months vs. 97 months) were significantly different (Table 1). On the other hand, there was no significant difference in the initial PSA, last PSA, PSAV and age between the two groups.
We conducted univariate and multivariate logistic regression analysis to identify the predictive factors for PCa in prostate needle biopsy. In the univariate logistic regression analysis, prostate volume (p<0.001, OR=0.916), PSAD (p=0.046, OR=3.322) and follow-up period (p=0.010, OR=1.025) were identified as significant predictive factors. Among these, prostate volume (p<0.001, OR=0.891) and age (p=0.022, OR=1.149) were identified as significant factors in multivariate logistic regression analysis (Table 2). Although PSAD was statistically significant in the univariate analysis, the result was challenged by the multivariate analysis. The AUC of prostate volume was 0.724 (Fig. 1). At 28.8 mL of prostate volume, the sensitivity and the specificity were 61.1% and 73.1%, respectively.
DISCUSSION
Although PSA measurement has contributed to the early detection and treatment of PCa, PSA may be elevated in other non-malignant conditions such as benign prostatic hypertrophy and prostatitis, I addition, the specificity of PSA for PCa is less than ideal. Therefore, PSA cutoff values for PCa diagnosis is still controversial and decision-making on the performance of a prostate biopsy based on only PSA cutoff values has clinical limitations considering the relative low specificity of PSA. Many studies have been conducted to determine an appropriate PSA cutoff value for PCa detection. Catalona, et al.11 reported that a PSA level of 4 ng/mL or higher was appropriate as the PSA cutoff value for screening of PCa. It is suggested that lowering the PSA cutoff value from 4 to 2-3 ng/mL is appropriate because high PCa detection rate is demonstrated in those range of PSA. PSA cutoff value from 4 to 2.5 ng/mL results in an increase in the number of men who undergo biopsy and may result in an increased detection of potentially insignificant PCa.12 The adequate PSA cutoff value for prostate biopsy remains controversial. At the cutoff value of 4 ng/mL for PSA, the sensitivity is 67.5-80% and the specificity is only 20-30%. Another study reported the sensitivity and specificity of PSA were about 79% and 59% respectively.13 According to a study by Schmid, et al.,14 the PCa detection rate between PSA levels of 4.1-10.0 ng/mL is 25% and PSA levels of over 10 ng/mL has a detection rate of 50-60%. In our study, the PCa detection rate between PSA levels of 4.1-10.0 ng/mL was 18% and PSA levels of over 10 ng/mL has a detection rate of 47%, which is lower than the detection rates reported by Schmid, et al.14 The lower detection rate of PCa in Korea is likely attributable to the lower morbidity of PCa. However, our result was slightly higher than the PCa detection rate of 15.9% reported by Lee, et al.15 in patients with a PSA of 4.1-10.0 ng/mL in Korea. The low specificity of PSA and the relative low detection rate of PCa in this gray zone, have raised a question as to whether the strategy of prostate biopsy simply based on PSA cutoff values is sufficient for selecting suitable candidates for prostate biopsy. To compensate for the limitations of PSA, many potential predictive factors for PCa in biopsy such as PSAD, PSAV, age-adjusted PSA level and the ratio of free-PSA have been introduced.1 Recently, PSA-age volume, volume of transitional zone, and PSA-transitional volume density have been investigated.16,17
In the current study, there was a statistically significant difference in prostate volume, PSAD and the follow-up period between the two groups. Prostate volume was identified as a significant predictive factor of PCa detection in both the Student's t-test and multivariate logistic regression test. This is supported by the prostate volume AUC of 0.724 in the ROC curve (Fig. 1). Al-Azab, et al.18 also reported that a smaller prostate size was associated with PCa patients with PSA of 2.0-9.0 ng/mL. Other studies also demonstrated significant differences in the prostate volume between the patients with and without PCa.19-21 High PSA levels are positively related to PCa at biopsy, but a large prostate volume has a negative relationship. Prostate volume, itself is related to serum PSA and age.21 It is thought that high PCa detection in small prostate volume is caused by a relatively large PCa volume in normal prostate.
PSAD also has been introduced as a useful tool to increase the specificity in the early detection of PCa.22 In the current study, PSAD was statistically significant in the univariate analysis but the result was challenged by the multivariate analysis. It was reported that performing a prostate biopsy when the levels of PSAD is greater than 0.15 ng/mL/mL increases the cancer detection rate and can safely reduce the number of patients undergoing prostate biopsy without significantly compromising the cancer detection.23,24 The usefulness of PSAD for PCa detection is widely accepted in the PSA range of 4.0-10.0 ng/mL; however, this has been controversial and it's advantages have not been fully accepted.25,26 Prospective multi-center studies with a larger number of patients are needed to firmly establish the usefulness of PSAD.
Our study had some limitations. First, the sample size was relatively small and there was a lack of diversity in the subjects because the subjects were selected from a single hospital. Second, we only considered the first prostate biopsy. We were not able to reflect the results of repeated biopsies due to a considerable number being lost to follow-up and potential ethical issues. Among patients who were not diagnosed with PCa in the initial biopsy, 20% were diagnosed with PCa in repeated prostate biopsy.27 Third, we measured prostate volumes by means of TRUS and several experienced radiologists, not by prostatectomy specimens and only one experienced radiologist. This could be associated with inter- or intra- observer variability due to the subjective aspects of probe placement and choice of planar dimensions for measurement. If any error was made in measuring the height, width or length of the prostate by TRUS, the accuracy of prostate volume and PSAD would be reduced. However, TRUS is widely used to calculate prostate volume and is considered a reliable technique to estimate prostate size, with accuracy within 20% of the pathological weight.28 Moreover, a significant intra-observer variation in TRUS-guided prostate volume measurement could also exist even among highly experience radiologists. However, this variability is not enough to affect one's eligibility for PCa active surveillance strategy when PSAD criteria are used.29 Therefore, TRUS-guided prostate volume measurements is a reliable method of assessing prostate volume and PSAD in patients with PCa.
In men with PSA values more than 4 ng/mL during the periodic follow-up, a small prostate volume is the most important factor in the early detection of prostate cancer. It is suggested that clinicians should pay greater attention to patients with a prostate volume less than 28.8 mL as well as high PSA levels more than 4 ng/mL.
 XML Download
XML Download