

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In the context of surgical revascularization, off-pump coronary artery bypass surgery (OPCAB) is gaining renewed appreciation as studies report improved outcome in high-risk patients compared with the on-pump procedure.1,2 Despite avoiding cardiopulmonary bypass (CPB), OPCAB still requires systemic heparinization due to the obligatory period of coronary hemostasis during grafting. In addition, concerns have been raised regarding a hypercoagulable state associated with surgery-related systemic inflammatory response and warm regional myocardial ischemia/reperfusion, jeopardizing the early graft patency.3-5 Accordingly, an aggressive anticoagulation strategy maintaining a target activated clotting time (ACT) of >300 s has been advocated.6,7
Due to the conflicting demands of prevention from ischemic and hemorrhagic complications,8,9 it is crucial to define the optimal level of anticoagulation with heparin during OPCAB. Contrary to surgical revascularization using CPB, a generally accepted uniform anticoagulation strategy for OPCAB is currently lacking. Surveys of different countries report achievement of systemic anticoagulation using heparin to maintain a target ACT from 200 s to even >480 s requiring full heparinization during OPCAB.10,11
In the era of dual antiplatelet therapy, many patients present to surgery with continued clopidogrel therapy because of its ischemic benefit.12-14 Although OPCAB has been safely performed in these patients,15-17 clopidogrel therapy in proximity to surgery carries a considerable risk of hemorrhagic complications.18,19 Thus, it is reasonable to assume that these patients may benefit from a lower target range of ACT without being exposed to an increased risk of ischemic complications; however, no comprehensive studies exist.
The aim of this retrospective study is to assess an optimum target range of ACT yielding ischemic protection without the increased risk of hemorrhagic complications in patients on continued dual antiplatelet therapy within 7 days of OPCAB.
MATERIALS AND METHODS
Patients and perioperative management
After obtaining Institutional Review Board approval, we reviewed electronic medical charts of 867 patients who underwent isolated multi-vessel OPCAB between April 2007 and May 2011. Patients who had received oral aspirin and clopidogrel within 7 days of operation were selected. The daily dose of clopidogrel was 75 mg in all patients, and a single 300 mg loading dose was administered in patients with unstable angina upon coronary angiography before starting the daily dose. Exclusion criteria included any emergency surgery, history of previous cardiac surgery, myocardial infarction (MI) within 1 week from surgery, known preoperative coagulopathy, preoperative intravenous heparinization, use of any other antiplatelet or anticoagulant agents, history of chronic renal failure/previous renal transplantation surgery, emergent conversion to on-pump coronary artery bypass grafting (CABG), or excessive postoperative bleeding due to any obvious surgical bleeder.
All patients received standardized anesthetic and surgical care. General anesthesia was induced with intravenous midazolam and sufentanil. Anesthesia was maintained with sevoflurane and continuous infusion of sufentanil. Neuromuscular blockade was achieved by administering rocuronium bromide and maintained with continuous infusion of vecuronium bromide. Intravascular volume replacement was managed with crystalloid and colloid solutions to maintain the pulmonary capillary wedge pressure as measured by pulmonary arterial catheter (Swan-Ganz CCombo CCO/SvO2; Edwards Lifesciences, Irvine, CA, USA) between 8-16 mm Hg according to the baseline values. Pulmonary arterial blood temperature was maintained at 36-37℃ with a warm mattress, forced warm air blanket and fluid warmer as necessary. All surgical procedures were performed through a median sternotomy. The heart was displaced with a deep pericardial traction sutures, large gauze (12×70 cm), and a tissue stabilizer (Octopus Tissue stabilization System; Medtronic Inc., Minneapolis, MN, USA). Revascularization was carried out using a left internal mammary artery connected with an additional graft using radial artery, great saphenous vein, or both in a Y-configuration. All patients were transferred to the intensive care unit after the operation, and standardized protocol for immediate postoperative care was followed. Aspirin (100 mg) and clopidogrel (75 mg) were given orally starting from 24 hr after the surgery, and supplemental 100 mg of cilostazol was added for the patients whose vein was grafted or arterial conduit was calcified in a measure.
Heparinization and ACT measurements during anastomoses
Baseline ACT was determined immediately before the induction of anesthesia. In the preference and discretion of the surgeon and attending anesthesiologist, initial 80-150 U/kg dose of unfractionated heparin was given to achieve a target ACT of 200, 250, or >300 sec just prior to Y graft formation. Five min after the initial dose of heparin, the ACT was measured and follow-up measurements during graft anastomoses were performed every 30 min as long as it remained within the target range. Otherwise, 1000-2000 U of additional heparin was given according to the remaining number of distal anastomoses, and ACT was re-measured after 5 min. At the end of the anastomoses, the ACT was measured again and heparin activity was neutralized with 20-50 mg of intravenous protamine sulfate to achieve the baseline ACT. A follow-up measurement of ACT was performed after 10 min. ACTs were measured by blood sampling from an arterial line, with a standardized Hemochrone device (International Technidyne Corp, Edison, NJ, USA) using Hemochron HRFTCA510 celite ACT tubes. Administration of heparin and protamine, measured ACT levels, and time intervals between the measurements were prospectively recorded to an institutional database.
Blood loss and transfusion management
In all cases, intraoperative blood loss was recorded as the amount of blood collected by a cell salvage device, which was processed and re-infused to the patients. Postoperative blood loss was recorded as the volume of chest and mediastinal tube drainage up to 24 h after the operation. Drained blood was not re-infused into patients. Allogeneic packed red blood cells (pRBC) were transfused when the hematocrit level was <24% throughout the study period. Fresh frozen plasma (FFP) was transfused when the postoperative international normalized ratio was >1.5 with excessive bleeding of >200 mL/h for 2 consecutive hours. The criteria for the transfusion of platelets were postoperative platelet count <50000/mm3 with excessive bleeding >200 mL/h for two consecutive hours. The total number of units of pRBC, FFP and platelets concentrates given during the operation and the postoperative period were recorded. Surgical re-exploration was indicated when chest tube drainage was greater than 200 mL/h for 6 consecutive hours or greater than 400 mL during the first hour despite normalized ACT and global coagulation status. All data regarding blood loss and transfusion requirement were also prospectively recorded to an institutional database.
Outcome analyses
Time weighted average ACT
We calculated time weighted average (TWA) ACT level as area under the curve for the duration of the ACT measurements

divided by duration, according to the following equation.
Endpoints
The primary end point of the current study was to compare combined hemorrhagic and ischemic outcomes in relation to the tertile distribution of TWA ACT. The hemorrhagic outcome endpoint included the incidence of significant blood loss and transfusion of two or more units of pRBC during the perioperative (intraoperative and postoperative 24 hr) period. We defined the significant blood loss as profuse bleeding of more than 30% of the estimated blood volume. The ischemic outcome endpoint was MI occurring within postoperative 7 days. MI was defined as the occurrence of increase in creatine kinase-MB (five times above the upper normal limit) and/or development of new pathologic Q wave on electrocardiogram.20 CK-MB was evaluated 1 day prior to surgery and daily for 1 week after surgery. Secondary endpoints included evaluation of the risk factors for composite of hemorrhagic and ischemic outcome endpoints including the TWA ACT tertile. The predictive role of TWA ACT tertile on the each individual endpoint was also investigated.
Additionally, thirty-day angiographic patency of bypass grafts was compared among the tertiles. It was determined by reviewing computed tomography (CT) angiogram findings, which were performed using a 16-slice CT scanner (Sensation 16, Siemens, Forchheim, Germany) with 100 mL to 120 mL of nonionic contrast agents (370 mg/mL iodine, Iopamiro; Bracco, Milano, Italy) at our institution. The graft was defined as occluded if a stump was seen or if there was no contrast in a grafted area known by operative report.
Statistical analysis
Statistical analyses were performed using SPSS 18.0 (SPSS Inc., Chicago, IL, USA). Continuous variables among the tertiles were compared by one-way analysis of variance with a Bonferroni post-hoc test. Continuous variables were compared between patients who were transfused or not by t-test for normally distributed values; otherwise, Mann-Whitney U tests were used. Proportions were compared by Fisher exact test or chi-square test as appropriate. The odds ratios and 95% confidence intervals (CI) investigating the independent predictive role of TWA ACT on the hemorrhagic and ischemic endpoints were assessed by logistic regression. Variables with p<0.2 between patients who were associated with the outcome endpoint or not were first evaluated in the univariate model. Only variables with p<0.1 were then entered into the final model of the multivariable logistic regression analysis. Categorical variables are expressed as the number of patients (%) and continuous variables are expressed as mean±standard deviation.
A p<0.05 was considered significant.
RESULTS
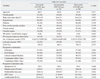
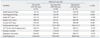
Three hundred and five patients were enrolled in this study. The overall mean TWA ACT was 320±56 sec, and the median value was 311 sec. The ranges of TWA ACT levels according to the tertile distribution were 212 to 291 sec, 292 to 334 sec, and 335 to 485 sec. Patient characteristics were similar in relation to tertile distribution of the TWA ACT levels (Table 1). Intraoperative characteristics of the tertiles were also comparable except for ACT values and dose of weight-adjusted heparin and protamine administered, as expected. Total heparin doses were 100±30 U/kg, 123±50 U/kg, and 139±37 U/kg, respectively (p<0.001) (Table 2). The overall percentage of patients who achieved target ACT levels by the first heparin dose was 93%, and 25% of patients needed extra heparin during the whole grafting period. This was distributed similarly among the tertiles.
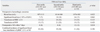
The amount of perioperative blood loss was 937±313 mL, 1014±340 mL, and 1076±383 mL, respectively (p=0.022). The incidences of significant perioperative blood loss and transfusion of pRBC ≥2 U were lower in the first tertile compared to the other tertiles, but without statistical significance. A significantly greater number of patients in the third tertile developed postoperative MI compared with those in the first and second tertiles (p=0.034). The composite of significant blood loss, transfusion of pRBC ≥2 U, or postoperative MI occurred in 20%, 28%, and 30% of the patients for each tertile, respectively (p=0.190) (Table 3).
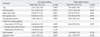
In the univariate analysis of predictors for adverse combined hemorrhagic and ischemic outcomes (a composite of significant perioperative blood loss, transfusion of pRBC ≥2 U, or postoperative MI), age, female gender, body mass index (BMI), preoperative hematocrit level and platelet count, TWA ACT tertile, the number of grafts, and the operation time had a p<0.1. In the multivariate analysis, female gender, lower BMI, lower level of hematocrit, TWA ACT tertile, and longer operation time remained independent risk factors. The first tertile was associated with a 52% risk reduction of combined hemorrhagic and ischemic outcomes (95% CI: 0.25-0.92, p=0.027) (Table 4).
Thirty-day follow-up CT angiograms were available in 246 patients (90%, 76%, and 75% in each tertile, respectively). The remainder did not undergo CT for various reasons such as follow-up loss, cost, or the patient refusal. The incidence of impaired graft patency was comparable (8%, 14%, and 8%, respectively, p=0.294).
DISCUSSION
The current study demonstrated that a lower degree of anticoagulation, represented by the first tertile of TWA ACT (212-291 sec) may provide net clinical benefit of hemorrhagic and ischemic outcomes following OPCAB in patients with recent exposure to clopidogrel, compared with those in the higher tertiles. The first tertile of TWA ACT was associated with 77% risk reduction of significant perioperative blood loss. Moreover, for composite blood loss, pRBC transfusion ≥2 U, postoperative MI, and the first tertile of TWA ACT was associated with a 52% reduced risk.
As dual antiplatelet therapy has become the cornerstone of the management strategies for coronary artery disease, an increasing number of patients referred for surgical revascularization are brought to surgery with recent exposure to clopidogrel for the ischemic benefit.13 Despite concerns for consequent excess of hemorrhagic complications, several reports have suggested that platelet inhibition, to a certain extent, may improve postoperative outcomes.12,14 OPCAB has been especially proposed as a safe surgical technique that can be performed without increasing the risk of bleeding in patients under a sustained influence of clopidogrel.15-17 On the contrary, concerns have been raised about the procoagulant activity associated with OPCAB that increases the risk of venous thrombosis and potentially endangers the patency of coronary anastomoses.21-25 These aspects have led to the use of an aggressive perioperative anticoagulation strategies incorporating systemic heparinization to maintain a target ACT of >300 s during surgery with early-resumed postoperative dual antiplatelet therapy.26,27 While a uniform standardized heparinization protocol is lacking for OPCAB, a European survey revealed that 41% of surgeons consider the lower limit of the target ACT >300 s and 16% of surgeons even consider full heparinization despite avoiding CPB.28
In patients with a recent exposure to dual antiplatelet therapy to OPCAB, maintaining a target ACT of >300 s may put patients at an unnecessary risk of periprocedural bleeding without the added ischemic benefit. Thus, optimal intraoperative anticoagulation that can minimize the procoagulant activity while avoiding the hemostatic deteriorations is of critical importance. Yet, the clinical effect of the anticoagulation levels on the outcomes following OPCAB in such patient populations has not been addressed. Numerous studies reported the impact of the degree of heparinization on clinical outcomes in the setting of percutaneous coronary intervention (PCI), during which antiplatelet agents are loaded.29-34
In the current study, a lower degree of anticoagulation during OPCAB (TWA ACT <290 sec) was associated with a reduction in significant perioperative bleeding without increasing postoperative MI in the patients with recent exposure to clopidogrel. This is in agreement with the finding of the Precursor to EPILOG (PROLOG) study that demonstrated a diminished risk of bleeding without compromising the peri-PCI ischemic outcomes, by reducing the heparin dosing for patients treated with platelet glycoprotein IIb/IIIa inhibitors.35
In contrast to the PCI setting, during which anticoagulation is obtained with one-off bolus of heparin, repeated administration of heparin to maintain the target ACT for multi-vessel OPCAB is common. We, therefore, evaluated the effect of anticoagulation on the outcomes in terms of TWA ACT that contain an element of time rather than a simple heparin dose. A significantly reduced risk of perioperative bleeding in the first tertile of TWA ACT is due, in part, to a smaller dose of total heparin compared to the higher tertiles. A total heparin dose should be greatly influenced by initial heparin administered to achieve target ACT. The actual initial doses given to achieve a target of >250 sec and >300 sec were 100±5 and 149±6 U/kg, respectively. On the contrary, the initial dose administered in the first tertile of TWA ACT was 91±16 U/kg, while overall 88% of the total study population exceeded their goal ACT by more than 10% on the first heparin dose. Therefore, it can be inferred that the initial dose reduction can decrease perioperative bleeding without sacrificing the efficacy in patients with recent exposure to dual antiplatelet therapy close to surgery.
Regarding the ischemic endpoint, the incidence of MI was greater in the third tertile than compared with the lower two tertiles. This is in accordance with the analysis derived from six randomized controlled trials of antithrombotic regimens for PCI that demonstrated U-shaped curve for a relationship between ACT and ischemic events.29 ACT values greater than 350 sec at activation of devices were associated with a greater rate of MI or urgent revascularization for 7 days after procedure than those of lower levels. One suggested explanation for this greater thrombotic risk observed at higher ACTs was the platelet activation by high doses of heparin. Indeed, heparin activates platelets, forces them to express many of their GP binding sites, and consequently enhances their aggregation even at its therapeutic concentrations.36,37 Moreover, bleeding and subsequent transfusion of blood products have been reported to aggravate the occurrence of ischemic events.38 Another analysis of four large clinical PCI trials demonstrated that higher ACTs did not protect against ischemic events.13 The lack of an inverse relationship between ACT and ischemic complications was explained on account of concurrent GP IIb/IIIa inhibitors or clopidogrel therapy of their study populations (89% and 81%, respectively). Consistent findings from our study that the highest incidence of MI was in patients with the highest TWA ACT tertile, indicate that a higher-dosing heparin regimen during OPCAB is no longer need but rather detrimental for the patients with recent exposure to dual antiplatelet agents.
The main limitation of this study is its retrospective design. Although all patients were managed according to an institutional standardized protocol and all data was collected prospectively, targeted ACT was not determined by randomization. Another limitation of this study is that we did not assess individual responses to clopidogrel. However, there is currently no generally accepted platelet function assay with enough clinical evidence to support its influence on ischemic or hemorrhagic outcome. Advances over clopidogrel in terms of less interpatient variability in plasma concentrations and antiplatelet effects have been reported with a newer antiplatelet agent, ticagrelor. Of note, ticagrelor has a reversible action on the P2Y12 receptor with faster offset-a promising feature for patients undergoing surgery. As cumulating evidence supports its beneficial role in the PCI setting, further clinical experience and research regarding the optimal intraoperative anticoagulation management in patients treated by ticagrelor are warranted.
The current study suggests that for the patients with recent exposure to clopidogrel, a lower degree of anticoagulation during multi-vessel OPCAB appears to be beneficial in terms of surgery related ischemic and hemorrhagic complications. Based on this analysis, decreased initial heparin dosing targeting a lower ACT, just greater than 200 sec, should be considered for this subset of patients. Additional prospective randomized controlled trials are needed to establish the optimal anticoagulation management during OPCAB in an era of aggressive dual-antiplatelet treatment.
 XML Download
XML Download